Creating A Usable Measure of Actuarial Value Gary Claxton Vice President
advertisement

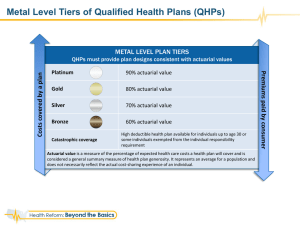
Creating A Usable Measure of Actuarial Value Gary Claxton Vice President Kaiser Family Foundation 10/17/2011 Roles for Actuarial Value in the ACA • Tiers of coverage for individuals and small businesses (and some others) • • • • 60% AV = Bronze 70% AV = Silver 80% AV = Gold 90% AV = Platinum – Concept: Different levels of cost sharing applied to defined benefit package (EHB) – But: Benefit package may not be well defined, so other elements, like benefit limits, could affect AV • Premium tax credits tied to silver tier • Reductions in cost sharing for lower-income individuals – Reduced deductibles and other cost sharing raise AV of silver plans to different levels for people at different incomes • Minimum value for ESI: Plan’s share of the total allowed costs of benefits provided under the plan must be at least 60% of such costs Estimating Cost Sharing Under the ACA • Study asked three different consulting firms to estimate cost sharing for nongroup coverage • Common Assumptions – Assumed typical employer plan as PPO covering broad range of services, with 82% actuarial value – Benchmarked to same average premium; assumed 10% for administration – Prevention covered without cost sharing • Simplifying assumptions included deductibles and coinsurance that applied to all services (other than prevention) • Firms estimated cost sharing combinations for some of the AVs relevant to the ACA – Focus on bronze and silver level plans, with upward adjustment for cost-sharing subsidies Estimates of Plan Designs Meeting Selected ACA Actuarial Value Thresholds, 2014 Actuarial Research Corporation Aon Hewitt Towers Watson Actuarial Value Out-OfPocket Maximum Deductible Coinsurance Deductible Coinsurance Deductible Coinsurance 60% $6,350 $6,350* 0% $4,350 20% $2,750 30% 70% $6,350 $4,200 20% $2,050 20% $1,850 20% 70% $4,200 $4,200* 0% $2,650 20% $1,550 30% 70% $3,200 $3,200* 0% $3,200* 0% $2,050 30% 73% $3,200 $3,200* 0% $3,200 0% $1,750 25% 87% $2,100 $1,050 20% $250 20% $150 20% 94% $2,100 $60 10% $200 5% $0 8% Note: Amounts shown for the out-of-pocket maximum and deductibles are per person; figures for families would be double these amounts. Where an asterisk appears, the firm was unable to construct a plan design within the constraints of the actuarial value and out-of-pocket maximum. The deductible shown in these cases is equal to the out-of-pocket maximum, which is the highest it can be. The out-of-pocket maximum amounts are based on those for high-deductible plans that qualify to be paired with a Health Savings Account, inflated forward to 2014. Why the Differences? • There are pretty big differences in the estimates • Firms assumed same average premium/cost, but – Different data with different distributions of spending – Different estimates of the impact of cost-sharing provisions on service use – Different estimates of the impact of first-dollar coverage for prevention • Using common data/service risk distribution would reduce differences • Over time, differences would shrink as vendors become familiar with new market structure and covered population Minimum Value for ESI Offers • Generally people offered coverage through a job cannot claim a tax credit for choosing coverage in an exchange unless the coverage offered – Is not affordable – Does not have a minimum value • Minimum value is an actuarial value test – Plan’s share of the total allowed costs of benefits provided under the plan must be at least 60% of such costs • Unlike exchange coverage, plans offered by large employers and selffunded plans are not required to offer essential health benefits – So 60% of what (how limited can the package be and still be health coverage)? – Potential for an objective benchmark (a benchmark package or a dollar amount) that could be used in determining whether 60% is met Much More to Come • We are awaiting regulations to describe how actuarial value will be determined for the different purposes of the ACA • An important open issue is how actuarial value will be determined if there is flexibility in definition of essential health benefits • There are a number of other important issues, for example – What is the standard population for each of the benefit tiers (risk adjustment probably cannot fully offset selection against lower cost-sharing tiers)? – Will actuarial value calculations be audited or mostly rely on certifications from plan actuaries? – How will higher use from subsidized cost sharing be incorporated in the actuarial value calculations for plans?