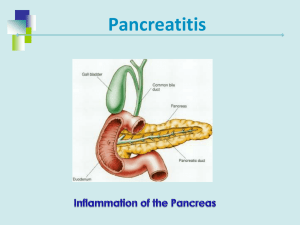
PANCREATITIS
advertisement

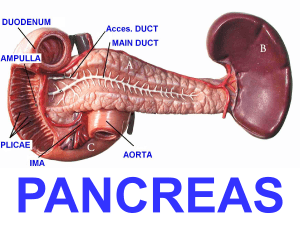
Lecture 36- Pancreatitis • a. Define • b. Discuss the causes and clinical features • c. Describe the morphological changes. A Pancreatitis • Pancreatitis is inflammation of the pancreas a\w injury to the exocrine parenchyma. • Normally digestive enzymes secreted by the pancreas are not active until they reach the intestinal tract. • When the pancreas is inflamed, the enzymes attack and .damages the tissue that produce them. • Duration of the disease can range different from: a transient attack to a permanent loss of function. • Classified into to form: 1. Acute pancreatitis- usually reversible 2. Chronic pancreatitis- irreversible. 2 What is acute pancreatitis? • Acute pancreatitis is in most instances a sterile (noninfectious) chemically mediated inflammation of the pancreas resulting from injury of the exocrine pancreas. • Reversible if the underlying cause is removed. • Patients typically present with: Epigastric pain with radiation to the back a\w increased pancreatic enzymes: (Amylase, trypsin and Lipase) in blood or urine. • Biliary tract disease and alcoholism account for approximately 80% of cases in West. 3 What is acute pancreatitis? • It occurs in two forms: 1. Interstitial or edematous pancreatitis: Mild inflammation with edema & widening of interstitial spaces. No or only minor necrosis. • Mild elevation of pancreatic enzymes in blood. • It requires no treatment and heals spontaneously. 2. Acute hemorrhagic pancreatitis: Severe and life-threatening condition, which is not common. “Pancreatic& peripancreatic” • Prominent enzyme-mediated destruction. 4 Etiologic Factors in Acute Pancreatitis >than 85 drugs , furosemide, ER Fall 10 A Jalan 5 Pathogenesis of acute pancreatitis 1. Pancreatic duct obstruction edema compression of blood vessels ischemia acinar cell injury. 2. Acinar cell injury release of pancreatic & lysosomal enzymes activation of enzymes autodigestion of pancreas. 3. Defective intracellular transport of proenzymes Fall 10 within acinar cells. 6 The morphology of acute pancreatitis 1. Acute inflammation. 2. Microvascular leakage causing edema. 3. Enlargement. 4. Proteolytic destruction 5. Destruction of blood vessels and subsequent interstitial hemorrhage. 6. Necrosis of fat by lipolytic enzymes. A Jalan 7 45years old male subjected to abdominal direct trauma, followed by sever abdominal pain- operation findings? Fat necrosis- white chalky deposits Fat necrosis • Fat necrosis, results from enzymatic activity of lipase. • The released fatty acids combine with calcium to form insoluble salts that impart a granular blue microscopic appearance to the fat cells. • Acute necrotizing pancreatitis, acinar and ductal tissues as well as the islets of Langerhans are necrotic. Fall 10 Clinical findings of acute pancreatitis • is a medical emergency ”acute abdomen”. • All cardinal manifestation of acute inflammation. • Acute pancreatitis attributed to release of toxic enzymes, cytokines, and other mediators. • Patients present with: – Severe, mid-epigastric pain with radiation to the upper back “band-like”. – Fever, nausea and vomiting. – Peripheral vascular collapse and shock. – Cullen sign & Grey Turner sign – Paralytic ileus “no bowel sound heared”. 10 Grey Turner sign ( flank hemorrhage), Cullen’s sign (periumblical hemorrhage), 11 Investigations 1. Increased serum lipase (MORE SPECIFIC)-72-96hrs. 2. Increased serum & urinary amylase (less specific)- 24 hrs. • Other causes of hyperamylasemia include: Mumps,small bowel infarction and a ruptured ectopic pregnancy. 3. CBC: Neutrophilic leukocytosis. 4. Serum calcium: Hypocalcemia. 5. Blood glucose: Hyperglycemia (destruction of beta islet cells). 6. LFT: Bilirubin, AST 7. CT scan is the gold standard for pancreatic imaging- enlarged inflamed pancreas. 8. Endoscopic retrograde cholangiopancreatography Diagnostic criteria • Two of the following three are required to make a diagnosis: • (1) Typical abdominal pain; (band-like) • (2) Threefold or more elevation of pancreatic enzyme values in the blood; • (3) Inflammation of the gland on computed tomography (CT) scan or magnetic resonance imaging (MRI) scan. Fall 10 A Jalan 13 Complications A. Tetany: A. Hypocalcemia is caused by enzymatic fat necrosis B. Calcium binds to fatty acids leading to a decrease in ionized ca+. B. Pancreatic pseudocyst: A. Collection of digested pancreatic tissue around pancreas. C. Pancreatic abscess: high mortality unless drained D. ARDS with hypoxemia, may occur. • Circulating pancreatic phopholipase destroys surfactant • Loss of surfactant produces atelectasis. E. Hemorrhagic ascites F. Haemolysis and DIC. G. Shock with acute renal tubular necrosis & failure. Chronic pancreatitis • is defined as chronic inflammation of the pancreas with irreversible destruction of exocrine parenchyma. . • Is characterized by: 1. 2. 3. 4. 5. 6. Secondary to repeated bouts of pancreatitis. Chronic inflammatory cells infiltrates Atrophy, fibrosis and concretion. Cystic dilatation and clacification. Loss& atrophy of endocrine acini, ”islets”-late. Commonly a\w Alcohol abuse. • Results in pancreatic insufficiency: A. Steatorrhea, B. Fat soluble vitamin deficiency (A,D,E& K). C. Diabetes mellitus. Etiology of Chronic pancreatitis 1. Long-standing obstruction of the pancreatic duct by pseudocysts, calculi, trauma, neoplasms. 2. Long-standing exposure to toxin or alcohol. [Alcohol thickens ductal secretions. Also increases duct permeability to enzymes]. [70%] 3. Tropical pancreatitis, heterogeneous disease (Africa and Asia), a few cases have a genetic basis. 4. Hereditary pancreatitis. 5. CFTR gene mutations- Pathogenesis of Chronic pancreatitis • Pathogenesis of acute pancreatitis: 1. Ductal obstruction by concretions increase protein concentrations in the pancreatic juice (alcohol) – Alcohol: thickens ductal secretions. 2. Toxic effects-direct effect of toxin& alcohol. 3. Oxidative stress. Alcohol-induced oxidative stress may generate free radicals in acinar cells, leading to membrane lipid oxidation. Fall 10 A Jalan 18 Clinical features 1. Repeated attacks of mild, moderate or persistent abdominal pain, with back pain. 2. DM developed. 3. Attacks of jaundice- Gallstone-induced obstruction. 4. Weight loss and hypoalbuminemic edema -malabsorption caused by pancreatic exocrine insufficiency. 5. Pancreatic pseudocysts 10%, CANCER 40%. • 1. 2. 3. 4. Laboratory and radiographic findings: Increased amylase- elevated “During the attack”. Alkaline phosphatase- elevated. Jaundice (increase serum bilirubin ). Pancreatic calcifications (CT scan best study)