Cardiovascular: Heart
advertisement

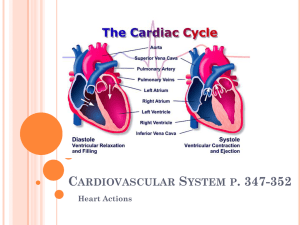
Physiology 31 Lecture Chapter 14: Cardiovascular Physiology - Heart I. Overview A. Overview of the Cardiovascular System B. Cardiac Muscle and Heart Function C. Conduction System of the Heart D. Heart Sounds E. The Cardiac Cycle F. Cardiac Output II. Overview of the Cardiovascular System A. ____________ transported by the cardiovascular system include 1. ____________ digested and absorbed from the digestive system 2. _________ in which other substances, such as ions, are dissolved in the plasma 3. Gases include a. _______ absorbed from the lungs and delivered to body tissues b. ______ picked up from tissues and taken to the lungs 4. __________, such as urea, uric acid, and creatinine, which are delivered to the urinary and digestive system for excretion 5. Chemical signals, such as ____________ and neurohormones B. The Cardiovascular System transports material in a ___________ route through the body in the following sequence: Heart → _______ → arterioles → capillaries → venules → ______ → heart C. The heart is a four chambered ________ with two basic functions 1. _________________ circulation (right heart) proceeds as follows a. Deoxygenated blood flows from the right ________ through the tricuspid valve to the right ventricle b. The right ____________ pumps blood through the pulmonary semilunar valve to pulmonary arteries and arterioles to the lungs c. In lung capillaries, ___________ diffuses into blood and _____ diffuses out d. Oxygenated blood returns to the heart via the pulmonary ______ 2. _____________ circulation (left heart) continues the circuit a. Oxygenated blood enters the left _________ and passes through the mitral (bicuspid) valve to the left ventricle b. The left __________ pumps blood through the aortic semilunar valve into the ________, which branches into arteries, arterioles, and capillaries c. From ____________, oxygen and nutrients diffuse out to tissues, and waste products diffuse from tissues into the blood d. Capillaries converge into venules, which converge into _______ transporting blood back to the heart e. The ___________ bring deoxygenated blood to the right atrium, and the pulmonary circuit begins again 2 D. ___________ vessels supply heart tissues 1. Coronary ___________ emerge from the base of the aorta to transport blood with oxygen and nutrients for heart tissues 2. Coronary _________ pick up waste products from heart tissues and transport deoxygenated blood back to the R. ________ 3. Blockage of a coronary artery due to _____________ plaque or blood clot can lead to a. __________ – loss of blood flow (oxygen) to the affected area, causing necrosis (death) of surrounding heart tissue b. ___________ pectoris – pain or heaviness in the chest, often accompanied by radiating pain into the jaw &/or left arm c. Myocardial ____________ - heart attack and possible death III. Cardiac Muscle & Heart Function A. The heart wall consists of three ___________ (outer to inner): 1. _____________ – a two layered membrane that includes a. ____________ pericardium – a tough fibrous sac that loosely surrounds the heart in the mediastinum (between the lungs) b. Visceral pericardium (_____________) – a thin mesothelium membrane that adheres to the heart surface c. Serous _______ in the pericardial cavity between the pericardial membranes minimizes friction with surrounding tissues d. ______________ is an infection of the pericardium; associated bleeding into the pericardial cavity compresses the heart (cardiac _______________) and can be lethal. 2. _____cardium – thickest region composed of cardiac muscle cells 3. ______cardium – thin endothelium that lines heart chambers a. _____________ is an infection of the endocardium, usually bacterial; can cause deterioration of heart valves B. Cardiac muscle cells rely mostly on ___________ respiration and are connected end to end by _______________ discs composed of 1. ______ junctions – protein channels that allow ions to flow from cell to cell, coordinating contractions of the cells 2. ______________ – “spot rivets” between cells that allow some stretch, and hold the cells together C. Cardiac muscle cells can contract without input from the _______ system. The two types of cardiac cells are autorhythmic cells and contractile cells 1. ______________ cells, such as those found in heart nodal tissue, initiate action potentials (and heart beats) in the following sequence a. __________ potential begins at –60 mV and rises to threshold (-40 mV) due to an influx of ____ through Na+ If channels that remain open at low membrane potentials b. Depolarization occurs at ___________ as voltage-gated ____ channels open, and Ca2+ rushes into the cell from the ECF (Na+ channels close as membrane potential rises) c. Repolarization occurs at about 0 mV when Ca2+ channels close and ___ channels open, causing K+ to move out of the cell. 3 d. When repolarization is complete, K+ channels close and the ___________ potential begins again 2. _______________ cells are stimulated by the autorhythmic cells and continue the action potential throughout the heart in the following manner a. ___________ membrane potential of contractile cells is about -90 mV. b. ___ junctions transport Ca2+, Na+, and K+ from autorhythmic cell to contractile cells, triggering the opening of voltage-gated ____ channels c. Depolarization (to +20 mV) occurs as ___ rushes into the cell, triggering the opening of voltage-gated ____ channels, and closing Na+ channels d. Ca2+ moves into the cell and opens __________-gated Ca2+ (ryanodine) channels in the sarcoplasmic reticulum (SR) e. Ca2+ from the SR binds to _________ and triggers contraction as in skeletal muscle (recall the sliding filament theory) f. Repolarization occurs as ____ moves out of the cell through K+ channels and Ca2+ channels close g. Relaxation of cells occurs as Ca2+ dissociates from troponin and is transported back into the SR via Ca2+-______ pump, and to the ECF via Na+-Ca2+ ______________ h. Resting Na+ and K+ concentrations are restored by the ___/___-_______ pump D. Autonomic neurotransmitters __________ cardiac contractile force and heart rate 1. Cardiac muscle contraction force depends on the number of _____________ formed, which depends upon how much Ca2+ is bound to troponin 2. _____ cytosolic ____ concentrations result in fewer crossbridges and weaker cardiac contraction 3. __________ and NE (sympathetic) bind to cardiac __ adrenergic receptors, and activate cAMP, which a. Phosphorylates and opens voltage-gated ___ channels, resulting in stronger cardiac contraction b. cAMP binds to open ____ If channels, so they remain open longer, speeding up depolarization and heart rate 4. The speed at which autorhythmic cells depolarize determines heart rate, and can be modified by altering cellular ___________ to ions a. Increased permeability to Na+ and/or _____ during the pacemaker potential will speed depolarization and heart rate. b. Decreased Ca2+ permeability or increased ____ permeability will slow depolarization and heart rate 5. __________ (parasympathetic) stimulation slows heart rate by a. ACh binds to cardiac ____________ cholinergic receptors that influence Ca2+ and K+ channels in autorhythmic cells b. Increase in K+ permeability ________polarizes the cells c. Decrease in Ca2+ permeability _________ the rate at which autorhythmic cells depolarize 4 IV. Conduction System of the Heart A. The cardiac conduction system consists of interconnected strands of ________ tissues (autorhythmic cells) that conduct electrical impulses through the heart, coordinating contractions. B. Sinoatrial (___) node - the “___________;” sets HR at 70-80 bpm 1. Found in R. _____ posterior wall, inferior to superior vena cava 2. Initiates the cardiac cycle by producing an __________ impulse that spreads over both atria, causing contraction 3. Atria _________ an instant after receiving the impulse from the SA node (ventricles are relaxed = diastole) 4. The impulse then passes along the ___________ pathway to the C. Atrioventricular (____) node - in the lower interatrial septum between the atrium and ventricle; it passes impulse to D. Atrioventricular bundle (bundle of ____) - extends from AV node into interventricular septum; this passes the impulse to E. L. & R. Bundle __________ - extensions of AV bundle down the L. & R. sides of the septum; these pass impulse to F. _____________ fibers - extend from the branches up into the ventricular walls; Impulses through C, D, & E cause ventricular contraction (called _________) G. An electrocardiogram (EKG or ____) records the electrical impulses through the heart as waves labeled P, Q, R, S, & T: 1. __ wave = SA node depolarization atrial contraction 2. ____ complex = ventricular depolarization ventricular contraction 3. ____ segment (from end of P wave to beginning of Q wave) represents the AV node delay (between SA node and AV node depolarization) 4. ___ wave = ventricular repolarization ventricular relaxation 5. ____ segment (from end of S wave to beginning of T wave) - time in which ventricles are contracting and emptying. 6. ____ interval (from end of T wave to beginning of P wave) - time in which the ventricles are relaxing and filling with blood. 7. Note: _______ repolarization also occurs, but the small wave is obscured by the _____ complex. 8. Heart ______ (HR) is timed from the peak of one P wave to the next P wave a. Normal resting HR is about ___-___ beats per minute (bpm) b. _______cardia is a HR of 100 bpm or more c. _______cardia is a HR of less than 60 bpm 9. EKGs can be used to diagnose abnormal heart _______, arrhythmias, and damaged heart muscle H. _______ rhythm – normal heart rate is 70-80 bpm, triggered by the _____ node; vagus nerves inhibit contractile cells at rest to maintain this rate I. Damage to the SA node can cause other nodal tissues (e.g., ___ node) to set the heart rate at a slower rate (_________ rhythm - typically about 40-60 bpm) 5 J. Any abnormal cardiac rhythm is called ______________, such as 1. _________ flutter - impulse waves circulate within the atrial myocardium; result is rapid atrial contractions (200 bpm) 2. Heart _________ – atria contract regularly, but the ventricles occasionally fail to be stimulated to contract after atrial contraction; due to a damaged conduction system 3. Ventricular __________ - ventricles contract rapidly in a weak, uncoordinated manner; caused by a damaged conduction system; can result in death if not corrected quickly V. Heart Sounds A. “Lub-dup” heart sounds are caused by the opening and closing of heart _________ 1. The “lub” is caused by the closing of ____ valves, when the ventricles contract at ___________ 2. The “dup” is caused by the closing of the ___________ valves, when the ventricles relax at the beginning of ____________ B. Body areas at which the valves may be listened to are called valvular ______________ areas, and include: 1. __________ area - 2nd intercostal space right of sternum 2. ____________ area - left, 2nd intercostal space left of sternum 3. Tricuspid & __________ areas are both near the 5th intercostal space, with the bicuspid more lateral C. Heart ___________ are caused by valve leakage or restriction and the turbulence of the blood as it passes through the heart. Three types of murmurs are: 1. Valvular ____________ - heart valves do not form a tight seal; causes a blowing sound after the valve closes 2. __________ - walls surrounding a valve are roughened or constricted; stiffened valves don’t open properly; produces a “click” sound during ventricular systole 3. _______ valve prolapse - inherited weakness of valve collagen & chordae tendinae that allows blood backflow through valve into atrium during systole; detected by a click followed by a swish 4. ___________ murmur - caused in children by the blood turbulence during heavy exercise; not serious VI. The Cardiac __________ (one contraction & relaxation) involves pressure changes in the heart and the way the pressure changes affect the heart valves and blood flow. The three phases include A. Ventricular __________ (in mid to late ventricular _________) 1. Blood flows passively into atria, through open AV valves, into _____________ 2. _____ contract (_ wave), forcing remaining blood into ventricles 3. End diastolic volume (_____) in ventricles is about 130 mL 6 B. Ventricular __________ 1. Isovolumetric _________ – ventricles contract (____ wave) and interventricular pressure rises, closing ____ valves; atria relax 2. Ventricular __________– ventricular pressure forces ____ valves open, blood is ejected into pulmonary trunk and aorta a. Each ventricle ejects a _______ volume of about 70 mL b. The blood remaining behind (60 mL) is the end systolic volume (_____) C. Isovolumetric _____________ – ventricles relax (__ wave), interventricular pressure drops, some blood flows backward, ___ valves close. Cycle then repeats. D. _______________ heart failure results from the failure of either ventricle to eject blood effectively, usually due to heart disease; causes pulmonary or systemic edema VII. Cardiac output is the amount of blood ________ by each ventricle per minute A. Cardiac __________ (CO) is the product of heart rate (____) and stroke volume (____): [CO = HR x SV], and averages about _____ L/min (recall that total blood volume in the body is 4-6 L) B. Normal adult HR averages about ___ bpm C. Heart _____ is raised by positive chronotropic agents and lowered by negative chronotropic agents in the autonomic nervous system 1. __________ oblongata contains a sympathetic cardioaccelatory center and a parasympathetic cardioinhibitory center a. Cardioaccelatory center nerves secrete nor_____________, which speeds HR & increases CO b. Cardioinhibitory center sends nerve impulses to the SA & AV nodes via the ______ nerves, which secrete ____, slowing HR to the normal rate 2. _________ceptors in muscles and joints inform the cardiac center of changes in physical activity 3. _______receptors (pressure receptors) in the ________ and internal carotid arteries send signals to the cardiac center if BP drops or rises, increasing or decreasing HR to compensate 4. ________receptors in aortic arch, carotid arteries, and medulla, sense changes in blood pH, CO2, and O2 and alter HR 5. Adrenal _________ secretes epinephrine and norepinephrine in response to arousal, stress, and exercise, which __________ HR 6. Other substances, such as caffeine, nicotine, and thyroid hormone _____________ HR 7. Electrolytes, such as Ca2+ and especially ____ ions, can increase or decrease HR D. Stroke ______ is governed by three factors: preload, contractility, and afterload 1. __________ is the amount of tension in the ventricular myocardium just before it begins to contract; this increases with physical activity – the more ventricles are _____________ with increased blood flow, the harder they contract a. Frank-_________ law – the more blood there is in a ventricle at the beginning of a contraction (increased EDV), the _______ the stroke volume b. EDV is determined by _________ return of blood to the heart, which is affected by 1) Skeletal __________ contractions 2) ____________atic contractions (respiratory pump) 7 3) Constriction of veins by _____________ NS activity 2. ______________ – contractile force of the myocardium for a given preload. a. Postive ionotropic factors, such as _____, epinephrine, norepinephrine, and glucagon _________ contractility and SV b. Negative ionotropic factors, such as low ____ and the vagus nerves ____________ contractility and SV 3. _____________ is the blood pressure in the arteries just outside the SL valves, which opposes the opening of the valves. Increased afterload ___________ stroke volume E. _____________ influences cardiac output via its effects on proprioceptors and on the venous return to the heart. Habitual exercise increases _____________ size and stroke volume, and reduces the resting ____.