Authorization to Release Information – WIC Program - SAMPLE FORM (WORD) - 11/5/14
advertisement
 - 11/5/14")
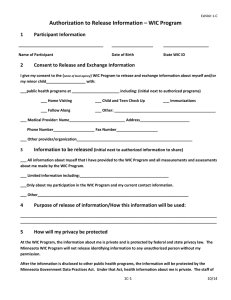
Authorization to Release Information – WIC Program Instructions: The local agency representative should assist the WIC participant in completing this form when used for the WIC Program. Completion of this form is optional. The participant may decide to release no data and the decision will have no impact on WIC Program eligibility or participation. However, all sections of this form must be complete in order to authorize release/exchange of data. Please be as specific as possible when completing sections 2-4 to limit the release/exchange of data, as needed. 1 Participant Information _________________________________________ ____________________ ______________________ Name of Participant Date of Birth State WIC ID 2 Consent to Release and Exchange Information I give my consent to the (name of local agency) WIC Program to release and exchange information about myself and/or my minor child___________________ with: ___Public health programs at _______________________ including: (initial next to authorized programs) ___ Home Visiting ___ Child and Teen Check Up ___ Immunizations ___ Follow Along ___ Other: _________________________________________________ ___ Medical Provider: Name___________________________ Address________________________ Phone Number____________________ Fax Number____________________ ___ Other provider/organization________________________________________________________ 3 Information to be released (initial next to authorized information to share) ___ Only limited information:_____________________________________________________________ ___ All information about myself that I have provided to the WIC Program and all measurements and assessments about me made by the WIC Program. ___Only my participation in the WIC Program and my current contact information. ___ Other_________________________________________________________________________ 4 Purpose of release of information/How this information will be used: (to be completed by person initiating the release/exchange of information) ________________________________________________________________________________________ ____________________________________________________________________ 11/14 5 How will my privacy be protected At the WIC Program, the information about me is private and is protected by federal and state privacy law. The Minnesota WIC Program will not release identifying information to any unauthorized person without my permission. WIC Program regulations also require my consent to release WIC data to any 3rd parties not listed here. The information will be protected by the Minnesota Government Data Practices Act. Under that Act, health information about me is private. The staff of the public health programs will have access to the information to the extent needed to perform their job duties for the programs. My medical doctor must protect the privacy of my health information under federal and state data privacy laws. 6 Whether I need to sign I understand that I do not have to agree to the release of information described in this document. I also understand that refusing to sign this authorization will not affect my eligibility or participation in the WIC Program or any other public health program, will not affect the current or future care I receive from any health care provider, and will not cause any penalty or loss of benefits to which I am otherwise eligible. However, if I do not sign the authorization and participate in more than one program, (name of local agency) may need to ask me the same health information questions or take the same measurements more than once. 7 Cancelling my permission I may cancel my permission at any time. In order to cancel my permission, I need to send or deliver a letter to (name and address of contact person at local agency) and include in the letter my request that my permission be cancelled, my name and date of birth, and my signature. This authorization expires 1 year from the date of my signature, unless it is revoked at an earlier date by me. ___________ ____________________________________ ____________________________________ Date Signature of Participant Printed Name of Participant 11/14 USDA is an equal opportunity provider and employer. 11/14