This article appeared in a journal published by Elsevier. The attached
copy is furnished to the author for internal non-commercial research
and education use, including for instruction at the authors institution
and sharing with colleagues.
Other uses, including reproduction and distribution, or selling or
licensing copies, or posting to personal, institutional or third party
websites are prohibited.
In most cases authors are permitted to post their version of the
article (e.g. in Word or Tex form) to their personal website or
institutional repository. Authors requiring further information
regarding Elsevier’s archiving and manuscript policies are
encouraged to visit:
http://www.elsevier.com/copyright
Author's personal copy
Journal of Experimental Social Psychology 47 (2011) 1214–1218
Contents lists available at ScienceDirect
Journal of Experimental Social Psychology
j o u r n a l h o m e p a g e : w w w. e l s ev i e r. c o m / l o c a t e / j e s p
Reports
Physiological, psychological and behavioral consequences of activating
autobiographical memories☆
Kathy Pezdek ⁎, Roxanna Salim
Claremont Graduate University, USA
a r t i c l e
i n f o
Article history:
Received 17 October 2010
Revised 20 January 2011
Available online 19 May 2011
Keywords:
Autobiographical memory
Priming
Belief
Memory
a b s t r a c t
Activating an autobiographical memory for a specific childhood event can have immediate and robust
physiological, psychological, and behavioral consequences. The target behavior was public speaking, a vital
skill about which many people are socially anxious. In this study, it was suggested to subjects that they had a
positive public speaking experience in early childhood; they then thought about and retrieved details of this
true childhood memory. Compared to a control condition in which a different suggestion was made, subjects
in the treatment group exhibited superior public speaking performance on the Trier Social Stress Test (TSST).
Further, physiological measures of cortisol and a self-report measure of anxiety (STAI-S) reflected a
significantly smaller increase in anxiety from before to after the TSST in the treatment than control condition.
Activating autobiographical memory for an event increases the accessibility of that memory and consequently
affects performance on related behaviors.
© 2011 Elsevier Inc. All rights reserved.
A number of researchers have reported that creating or changing
autobiographical beliefs can result in changes in autobiographical
memories (Mazzoni & Kirsch, 2002; Scoboria, Mazzoni, Kirsch, &
Relyea, 2004). More recently, Geraerts et al. (2008) and Scoboria,
Mazzoni, and Jarry (2008) reported that changing autobiographical
beliefs can have behavioral consequences as well. Specifically,
Geraerts et al. (2008) falsely suggested to participants that as a
child, they had gotten ill after eating egg salad. A significant minority
of their subjects came to believe that this event had occurred, and
both immediately and 4 months after the false suggestion, they
demonstrated a significantly reduced consumption of egg salad
sandwiches. However, having demonstrated the link between
planting false autobiographical beliefs and behavior, these authors
warned, “Scholars should consider this when conducting research on
false beliefs, because some subjects might experience adverse
outcomes from an experimentally induced false belief (p. 752).”
There are also serious concerns about the generalizability of these
findings based on the target events used in these studies. Results of
Pezdek and Freyd (2009) suggest that the food-aversion results of
these studies are restricted to less appealing foods that are less
☆ This study is part of the research supported by a BLAIS Challenge Fund to Kathy
Pezdek. We thank Mr. David Chamberlain, Mr. Michael Callahan and the students at
Claremont High School, and Mr. Ballingall and the students at Damien High School.
Without their cooperation, this study would not have been possible. We also thank Jaya
Roy, Luke Meyer, Khemara Has, Chandrima Batacharia, Matt O'Brien, Stacia Stolzenberg,
and Michael Schnapp for their help in collecting and encoding data, and Nicole Weekes
for her suggestions regarding the research.
⁎ Corresponding author.
E-mail address: Kathy.Pezdek@cgu.edu (K. Pezdek).
0022-1031/$ – see front matter © 2011 Elsevier Inc. All rights reserved.
doi:10.1016/j.jesp.2011.05.004
frequently consumed (e.g., egg salad but not chocolate chip cookies) –
that is, foods less likely to be the cause of overweight and obesity –
thus raising concerns about both the generalizability and the utility of
these findings. The purpose of the present study is to assess the
relationship between autobiographical memories and behaviors
without the ethical limitations of the false feedback procedure,
using a behavior about which there are fewer generalizability
concerns. Specifically, this study examines how activating true
autobiographical memories affects behavior.
Although psychologists have long known of the link between
beliefs and behavior (e.g., Ajzen, 2005), heretofore this research has
not examined the behavioral consequences of autobiographical beliefs
(i.e., beliefs about having performed a specific behavior in one's past),
nor has this research addressed the role of suggestibility in this
process. Cognitive psychologists have predicted that the link between
autobiographical beliefs and behavior is mediated by autobiographical memories (Mazzoni & Kirsch, 2002). That is, beliefs about one's
past (e.g., I was athletically active as a child) bidirectionally influence
one's memory for one's past 1 (e.g., specific memories of having been
athletic), and the question then is whether these beliefs and
memories affect one's current behavior (e.g., performance in a specific
new athletic endeavor). Although the results reported by Geraerts
et al. (2008) and Scoboria et al. (2008) suggest that the answer to this
question is, yes, there are likely to be limitations in the generalizability
of their findings in this regard.
1
There are, however, rare exceptions in which people can have vivid autobiographical memories for events that they no longer believe happened to them
(Mazzoni, Scoboria, & Harvey, 2010).
Author's personal copy
K. Pezdek, R. Salim / Journal of Experimental Social Psychology 47 (2011) 1214–1218
There is also a substantial social psychology literature in which it has
been demonstrated that individuals' behavior can be implicitly changed
as a consequence of activating relevant stereotypes, traits, and other
constructs (see Dijksterhuis & Barhg, 2001 and Wheeler & Petty, 2001
for reviews). Although the social psychology accounts of these “primeto-behavior effects” do not specifically implicate autobiographical
memory as part of this process, one of the frameworks for explaining
these effects is the Active-Self account (for a review see Wheeler,
DeMarre, & Petty, 2007). According to the Active-Self account, behavior
is guided by the active self-concept, and primed constructs can affect
behavior by temporarily altering the active self-concept. The current
study is derived from the relevant research on autobiographical
memory. Although the hypothetical construct, self-concept, surely
relies on information in autobiographical memory, the research on the
Active-Self account has not specifically assessed how priming autobiographical memory per se influences behavior. This is the focus of the
current study. The findings of this study will have implications for the
memory mechanisms likely to underlie the active self-concept.
The target behavior in this study is public speaking, a behavior that
is both socially imperative and about which many people are socially
anxious. Public speaking is associated with significantly elevated
arousal on a wide range of physiological measures of anxiety foremost
among these is cortisol level 2 (Dickerson & Kemeny, 2004; Witt et al.,
2006). In addition, at least one third of the population self-report high
levels of anxiety associated with public speaking (Stein, Walker, &
Forde, 1996), and public speaking anxiety is the most common social
anxiety in nonclinical samples (Hazen & Stein, 1995).
In this study, the treatment condition was designed to activate
participants' autobiographical memory regarding their facility with
public speaking. In the treatment condition, it was suggested to high
school students that prior to age 10, they had had a positive public
speaking experience, and they were then provided 5 min to think
about and retrieve details of this childhood memory. In the control
condition it was suggested that they had had a successful childhood
experience resisting phobias related to animals or medical experiences, and they were to think about and retrieve details of this
childhood memory. Each subject then participated in a public
speaking task, the Trier Social Stress Test (TSST), reported to elicit
significant increases in both psychological and physiological stress
responses (Kirschbaum, Pirke, & Hellhammer, 1993). If activating
autobiographical memories has a robust effect on behavior, then
participants would exhibit superior public speaking performance in
the treatment than control condition, and further, physiological
measures of cortisol and a self-report measure of anxiety would
reflect a smaller increase in anxiety from pre- to post-task in the
treatment than control condition.
Method
Participants and design
A total of 73 students participated from two high schools in
Claremont, California (μ age = 16.87 years, SD = .79, range = 14–
18 years; 33 females and 40 males approximately equally distributed
across conditions). Participants were recruited from the Speech and
Debate team and International Baccalaureate courses. Following
suggestions by Dickerson and Kemeny (2004), the exclusion criteria
were: (a) current or recent use of anti-anxiety or anti-depression
medication, (b) use of hormonal contraceptives, (c) cigarette
smoking, and (d) exercise or consumption of food or drink less than
1 h prior to testing.
2
Cortisol is a well-established marker of physiological stress and often the primary
measure included in studies utilizing the TSST to elicit a stress response.
1215
The design was a 2 (treatment versus control condition) × 2 (pre-/
post-task) mixed factorial design. The three dependent variables
were: (1) pre- and post-task markers of stress assessed by self-report
state anxiety (STAI-S), (2) salivary cortisol collected during baseline
and post-stressor periods, and (3) a behavioral measure of public
speaking anxiety assessed at one time from the video of each
participant's performance on the public speaking task. Details of
these measures are elaborated below.
Procedure and materials
The procedure used in this study was similar to that used in other
autobiographical memory studies (see for example, Pezdek, Finger, &
Hodge, 1997) except that in this study the childhood event primed
was a true event. Each participant was randomly assigned to the
control (N = 33) or experimental condition (N = 40). Approximately
1 week prior to participating in the study, volunteers completed a 30item survey that we developed and named the Affective Experiences
Scale (AES). The AES assessed possible childhood fears and phobias
experienced before the age of 10. Public speaking anxiety was
included in this list as were phobias of animals and medical situations.
In the baseline session, participants were told that their AES responses
had been computer analyzed, and each received feedback regarding
their specific responses. The treatment condition was designed to
activate participants' autobiographical memories regarding their
facility with public speaking. Participants in the treatment condition
were told that their AES responses predicted that they had
experienced some positive public speaking experiences before the
age of 10. They were then given 5 min to think about one of these
experiences and write everything they could remember about that
event. It is important to note that participants in the treatment
condition were not told that they were good at public speaking but
rather were told that in childhood they had had some positive public
speaking experiences. They were told that examples of these could be
simply effectively speaking to their family or a group of friends or
classmates. Defined this way, even poor public speakers have had
some positive public speaking experiences. Thus prompting memory
for a positive public speaking experience in childhood is not a
suggestion that the participant was necessarily a good public
speaker.
Participants in the control condition were told that their AES
responses predicted that they had experienced some positive
experiences resisting animal or medical phobias before the age of
10. They were then given 5 min to think about one of these
experiences and write everything they could remember about this
event. Every subject in both conditions provided a written description
of the prompted childhood event, and they reported that the event
have occurred to them. The manipulations in this study thus tapped
autobiographical memory for either the treatment or the control
event. The prompted events in both conditions were similar in that
each referred to a successful experience with an anxiety-arousing
event.
Volunteers participated individually in one 50 min session
consisting of a 20 min baseline period, a 10 min stressor task, and a
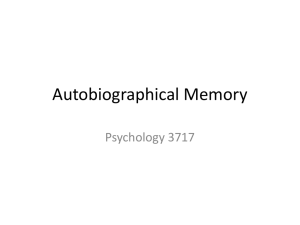
20 min post-stressor period (see timeline in Fig. 1). The 20 min
baseline period consisted of two pre-task cortisol samples (S1
collected at minute 5; S2 collected at minute 20), a pre-task state
anxiety assessment (STAI-S) at minute 10, and the AES feedback
session at minute 14. The 10 min stressor task consisted of a modified
version of the standardized Trier Social Stress Test (TSST) (Kirschbaum
et al.,1993). In this task, a second experimenter entered the room and
was introduced as an “evaluative college acceptance board member.”
The participant was asked to present a 5 min speech to the evaluator as
though they were interviewed for acceptance to their first choice
college. They were told that the evaluator would be judging them on
their communications skills. They were given 5 min to prepare their talk
Author's personal copy
1216
K. Pezdek, R. Salim / Journal of Experimental Social Psychology 47 (2011) 1214–1218
Fig. 1. Timeline including baseline period, stressor task, and post stress period. Baseline
period consisted of salivary cortisol samples at minutes 5 and 20, state anxiety assessment
(STAI-S), and AES feedback. Stressor task consisted of a modified Trier Social Stress Test
(TSST). Post-stress period consisted of state anxiety reassessment (STAI-S) and a poststress salivary sample. S = salivary sample; t = onset time for each task.
and were then instructed that they should talk for the full 5 min.3 The
20 min post-stressor period consisted of a post-task administration of
the STAI-S immediately after the TSST and a post-task salivary sample
collected at minute 40.
Self-report state anxiety
A psychological assessment of stress was measured pre- and poststressor using the Spielberger State Trait Anxiety Inventory-State
(STAI-S) scale. The STAI-S scale consists of 20 items (e.g., I am calm,
I am tense); participants stated the degree to which each statement
applies to them at the given moment, from 1 (not at all) to 4 (very
much so). Scores on the STAI-S range from 20 to 80.
Salivary cortisol
Participants provided three salivary samples using the passive
drool technique by which participants passively collect saliva in their
mouths and then drool into a cryovial tube for 2 min or until at least
one tube was full. Research indicates that the largest effect sizes of
cortisol are generated by afternoon collection and that peak cortisol
response occurs 15–30 min from onset of stressor (Kiecolt-Glasser,
2009). All experimental sessions occurred between 2:00 pm and 5:00
pm, with a post-stress salivary sample collected 18 min post onset of
TSST. 4 The average of the two pre-task salivary samples was used as
the pre-task measure of salivary cortisol.
Behavioral assessment of public speaking video (SPRS)
Three condition-blind coders rated videos of each participant's
speech using the Social Performance Rating Scale (SPRS) (Fydrich,
Chambless, Perry, Buerger, & Beazley, 1998). The SPRS is a behavioral
assessment of public speaking anxiety, in which each video is rated on
five dimensions (gaze, vocal quality, speech length, discomfort, and
conversation flow) using a 1 (very poor; highly anxious) to 5 (very
good; less anxious) scale. The sum of ratings produces a SPRS video
composite score with an overall internal consistency of alpha = .72.
Inter-rater reliability for the composite ratings of the three video
coders was high (Cohen's kappa = .86; mean Pearson r = .79; mean
proportion agreement = .82).
Results
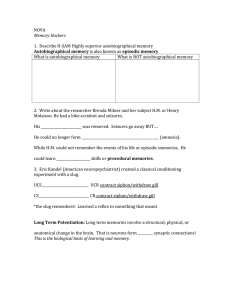
The results, presenting an impressively consistent pattern across
all three measures, are presented in Fig. 2. The data were first
analyzed with a 2 (treatment versus control condition) × 2 (pre-/post3
See Kirschbaum et al. (1993) for a more detailed description of the TSST
procedure.
4
Research indicates that passive drool contains higher concentrations of cortisol
than salivette collection techniques (Strazdins et al., 2005). Salivary samples were
frozen within 4 h of collection and stored at − 20 C until assay. Cortisol concentrations
were determined in duplicate using a fluorescent enzyme-linked immunosorbent
assay (ELISA) technique (Extended Range High Sensitivity Salivary Cortisol Enzyme
Immunoassay Kit, Salimetrics, State College, PA).
task) ANOVA performed on the STAI-S and cortisol data separately. In
the analysis of the STAI-S data, self-report ratings of anxiety increased
from pre- (μ = 50.34, SD = 15.46) to post-task (μ = 56.99, SD = 13.81),
F(1,71) = 48.13, p b .001, ηp2 = .40. Although the main effect of
condition was not significant, there was a significant interaction of
condition × pre-/post-task, F(1,71) = 26.96, p b .001, ηp2 = .28. As can
be seen in the first panel of Fig. 2, first, pre-task STAI-S measures did
not significantly differ between the control (μ = 48.88, SD = 12.91)
and treatment conditions (μ = 51.55, SD = 17.34), t b 1.00. Further,
although self-report measures of anxiety in the control condition
were greater at post-task (μ = 61.39, SD = 13.33) than pre-task
assessment (μ = 48.88, SD = 12.91), t(32) = 8.21, p b .001, d = .95, in
the treatment condition, there was no significant difference in this
measure between pre-task (μ = 51.55, SD = 17.34) and post-task
assessments (μ = 53.35, SD = 13.27), t(39) = 1.30.
The above pattern also resulted from analyses of cortisol data. Cortisol
measures significantly increased from pre-task (μ=.25 μg/dL, SD=.13)
to post-task (μ=.33; μg/dL, SD=.19), F(1,71)=33.22, p b .001, ηp2 = .32.
Although the main effect of condition was not significant, there was a
significant interaction of condition × pre-/post-task, F(1,71) = 10.32,
pb .01, ηp2 =.13. As can be seen in the middle panel of Fig. 2, first, pretask cortisol measures did not significantly differ between control
(μ = .25 μg/dL, SD = .10) and treatment conditions (μ = .25 μg/dL,
SD=.16), t b 1.00. Further, although cortisol measures were significantly
greater post-task than pre-task in both the control (μ= .39 μg/dL,
SD = .17 versus μ = .25 μg/dL, SD = .10, respectively, t(32) = 6.32,
pb .001, d=1.00) and treatment conditions (μ=.29 μg/dL, SD =.19
versus μ=.25 μg/dL, SD=.16, respectively, t(39)=1.84, pb .05, d =.23),
as predicted, this difference was greater in the control than treatment
condition.
In the analysis of the composite SPRS video coding data (higher
score = better performance; less anxious), as predicted, public
speaking anxiety was significantly lower in the treatment (μ = 18.41,
SD = 3.00) than control condition (μ = 16.33, SD = 3.96), t(71) = 2.55,
p b .01, d = .59 (see third panel of Fig. 2).
Discussion
This study shows that activating an autobiographical memory for a
specific childhood event had an immediate effect on related
behaviors, and the effect was a robust one. The manipulation in the
treatment condition – but not the control condition – improved public
speaking performance measured with SPRS ratings of video data and
affected two measures of anxiety, physiological measures of cortisol
and self-report STAI-S responses. This effect was not simply a result of
telling the treatment subjects that they were good at public speaking,
because this is not what they were told. Rather, they were told that in
childhood they had had some positive public speaking experiences —
with family, friends or classmates. Defined this way, even poor public
speakers have had some positive public speaking experiences. Thus
prompting memory for a positive public speaking experience in
childhood is not a suggestion that the participant was necessarily a
good public speaker. 5 The fact that every subject in both conditions
provided a written description of the prompted childhood event and
reported that this event had occurred to them suggests that it was
autobiographical memory that was driving these changes. And, given
that the prompted events in the two conditions were similar in that
each referred to a successful experience with an anxiety-arousing
event, the outcomes in this study are likely to have resulted from the
specific content of the autobiographical memory tapped.
5
Using another example, one could suggest to an individual that they had
experienced some unhappy events in childhood, and they could be asked to recall
one such event, without suggesting that the person had an unhappy childhood.
Author's personal copy
K. Pezdek, R. Salim / Journal of Experimental Social Psychology 47 (2011) 1214–1218
1217
Fig. 2. Mean result per condition on measures of state anxiety (STAI-S, possible range = 20–80 with higher scores indicating self reports of higher state anxiety), cortisol response
(reported in μg/dL with higher measures indicating higher anxiety), and SPRS video assessment (composite measure with possible range = 5–25; higher ratings indicating better
public speaking performance and less anxiety). Standard errors are represented by error bars.
In both this study and the previous related studies by Geraerts
et al. (2008) and Scoboria et al. (2008), beliefs or memories about
childhood events were activated and behavioral consequences
resulted. However, in both of the previous studies, the authors
suggested false beliefs and memories to participants. On the other
hand, in this study, the activated event was likely true although
probably forgotten. That is, regardless of whether someone has
always been anxious about public speaking or not, everyone has
likely had at least one successful public speaking experience before
the age of 10, even speaking to one's family, friends, or classmates,
which were included as examples in the treatment instructions. The
task in the treatment condition was to retrieve a memory for one
such true event. The treatment condition in the current study may
have been effective because it served to make memory for a
successful childhood public speaking experience – a true memory –
more accessible. Consistent results were reported in a recent study
by Kuwabara and Pillemer (2010). In this study, university students
were asked to recount a specific memory of being either satisfied or
dissatisfied with the university. Although behavioral measures
were not included in this study, compared to control subjects,
those who activated memory for a satisfying experience provided
higher ratings of their future intention to (a) donate money to
the university, (b) attend a class reunion, and (c) recommend the
university to others.
One explanation of the effect of the treatment suggestion in the
present study relates to the availability heuristic (Tversky &
Kahneman, 1973) as elaborated by Schwarz et al. (1991); that is,
people estimate the likelihood of an event by the ease of retrieving
instances of the event. Schwarz et al. had subjects recall 6 or 12
autobiographical situations in which they had behaved very assertively (or nonassertively). Subjects asked to recall 12 examples, which
was more difficult, later rated themselves less assertive (or less
unassertive) than those asked to recall 6 examples. Just as Schwarz et
al. found that people paid attention to the subjective experience of
ease or difficulty of recall in drawing inferences from recalled content,
in the present study, subjects likely concluded that if they could
remember a successful childhood public speaking experience, and
they all could, they are more likely to have some facility with public
speaking. If autobiographical beliefs and memories can influence
behaviors, then searching memory and retrieving a true memory for a
successful public speaking experience would increase the accessibility
of this and likely related memories. The more accessible memories of
successful public speaking experiences are, the more likely these
memories are to influence behavior.
This interpretation of the results of this study would also account
for the Active-Self account of prime-to-behavior effects reviewed
earlier (see Wheeler et al., 2007). According to this account, the selfconcept consists of a chronic self-concept, which includes all of the
aspects of self that are represented in long-term memory, and an
active self-concept, which includes a temporarily activated subset of
one's chronic self-concept. The active self-concept is then constructed
from one's autobiographical memory and includes a set of memories
that are relevant to the primed construct, and it is this temporarily
activated self-concept that is hypothesized to actually influence
behavior. Accordingly, priming specific autobiographical memories
increases their accessibility, and increases the probability that the
active self-concept will include aspects of self relevant to the activated
autobiographical memories.
In terms of the implications of this research for medical,
psychological and public health treatment programs, whereas ethical
principles are likely to prohibit planting false autobiographical beliefs
and memories, suggestively priming true beliefs and memories,
including those that may have been forgotten, is not unethical. The
effectiveness of the treatment condition in this study is consistent
with reports of the effectiveness of cognitive modification programs
for treating public speaking anxiety (see Allen, Hunter, & Donahue,
1989). Cognitive modification programs focus individuals on their
beliefs about, for example, their public speaking ability, and focus on
modifying those beliefs by making them more positive. Utilizing the
treatment procedures in this study to prime beliefs and memories for
positive experiences is likely to be a significant part of a successful
treatment program to enhance performance — with public speaking
and a wide range of other behaviors.
References
Ajzen, I. (2005). Attitudes, personality, and behavior (2nd ed.). Milton-Keynes, England:
Open University Press/McGraw-Hill.
Allen, M., Hunter, J. E., & Donahue, W. A. (1989). Meta-analysis of self-report data on
the effectiveness of public speaking anxiety treatment techniques. Communication
Education, 38, 54–76.
Dickerson, S., & Kemeny, M. (2004). Acute stressors and cortisol responses: A
theoretical integration and synthesis of laboratory research. Psychological Bulletin,
130, 355–391.
Dijksterhuis, A., & Barhg, J. A. (2001). The perception-behavior expressway: Automatic
effects of social perception on social behavior. In M. P. Zanna (Ed.), Advances in
experimental social psychology, Vol. 33. (pp. 1–40)San Diego, CA: Academic Press.
Fydrich, T., Chambless, D. L., Perry, K. J., Buerger, F., & Beazley, M. B. (1998). Behavioral
assessment of social performance: A rating system for social phobia. Behaviour
Research and Therapy, 36, 955–1010.
Geraerts, E., Bernstein, D. M., Merckelbach, H., Linders, C., Raymaekers, L., & Loftus, E. F.
(2008). Lasting false beliefs and their behavioral consequences. Psychological
Science, 19, 749–753.
Hazen, A. L., & Stein, M. B. (1995). Differential diagnosis and comorbidity of social
phobia. In M. B. Stein (Ed.), Social Phobia: Clinical and Research Perspectives
(pp. 3–41). Washington, D.C.: American Psychiatric Press Inc..
Author's personal copy
1218
K. Pezdek, R. Salim / Journal of Experimental Social Psychology 47 (2011) 1214–1218
Kiecolt-Glasser, J. M. (2009). Psychoneuroimmunology: Psychology's gateway to the
biomedical future. Perspectives on Psychological Science, 4, 367–387.
Kirschbaum, C., Pirke, K. M., & Hellhammer, D. H. (1993). The ‘Trier Social Stress Test’ —
A tool for investigating psychobiological stress responses in a laboratory setting.
Neuropsychobiology, 28, 76–81.
Kuwabara, K. J., & Pillemer, D. B. (2010). Memories of past episodes shape current
intentions and decisions. Memory, 18, 365–374.
Mazzoni, G. A. L., & Kirsch, I. (2002). Autobiographical memories and beliefs: A
preliminary metacognitive model. In T. J. Perfect, & B. L. Schwartz (Eds.), Applied
Metacognition (pp. 121–145). New York: Cambridge University Press.
Mazzoni, G., Scoboria, A., & Harvey, L. (2010). Non-believed memories. Psychological
Science, 21, 1334–1340.
Pezdek, K., Finger, K., & Hodge, D. (1997). Planting false childhood memories: The role
of event plausibility. Psychological Science, 8, 437–441.
Pezdek, K., & Freyd, J. J. (2009). The fallacy of generalizing from egg salad in false belief
research. Analyses of Social Issues and Public Policy, 9, 177–183.
Schwarz, N., Bless, H., Strack, F., Klumpp, G., Rittenauer-Schatka, H., & Simons, A. (1991).
Ease of retrieval as information: Another look at the availability heuristic. Journal of
Personality and Social Psychology, 61, 95–202.
Scoboria, A., Mazzoni, G. A. L., & Jarry, J. L. (2008). Suggesting childhood food illness
results in reduced eating behavior. Acta Psychologica, 128, 304–309.
Scoboria, A., Mazzoni, G. A. L., Kirsch, I., & Relyea, M. (2004). Plausibility and belief in
autobiographical memory. Applied Cognitive Psychology, 18, 791–807.
Stein, M. B., Walker, J. R., & Forde, D. R. (1996). Public-speaking fears in a community
sample. Archives of General Psychiatry, 53, 169–174.
Strazdins, L., Meyerkort, S., Brent, V., D'Souza, R. M., Broom, D. H., & Kyd, J. M. (2005).
Impact of saliva collection methods on sIgA and cortisol assays and acceptability to
participants. Journal of Immunological Methods, 307, 167–171.
Tversky, A., & Kahneman, D. (1973). Availability: A heuristic for judging frequency and
probability. Cognitive Psychology, 5, 207–232.
Wheeler, S. C., DeMarre, K. G., & Petty, R. E. (2007). Understanding the role of the self in
prime-to-behavior effects: The active-self account. Personality and Social Psychology
Review, 11, 234–261.
Wheeler, S. C., & Petty, R. E. (2001). The effects of stereotype activation on behavior: A
review of possible mechanisms. Psychological Bulletin, 127, 797–826.
Witt, P. L., Brown, K. C., Roberts, J. B., Weisel, J., Sawyer, C. R., & Behnke, R. R. (2006).
Somatic anxiety patterns before, during, and after giving a public speech. Southern
Communication Journal, 71, 87–100.