DESIGNING AN EXPLORATION ATMOSPHERE PREBREATHE PROTOCOL
advertisement

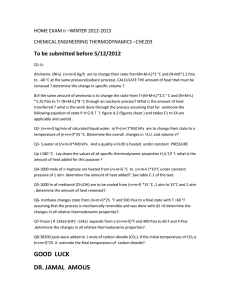
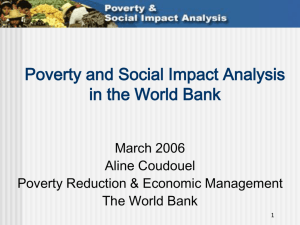
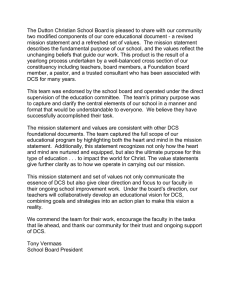
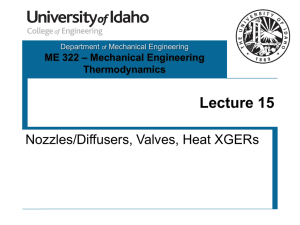
National Aeronautics and Space Administration DESIGNING AN EXPLORATION ATMOSPHERE PREBREATHE PROTOCOL J. Conkin1, A. H. Feiveson2, M. L. Gernhardt2, J. R. Norcross3, J. H. Wessel, III3. 1Universities Space Research Association, 3600 Bay Area Blvd., Houston, TX 77058, johnny.conkin-1@nasa.gov, 2NASA Johnson Space Center, 2100 NASA Parkway, Houston, TX 77058, 3Wyle Science, Technology & Engineering Group, 1290 Hercules, Houston, TX 77058. METHODS ABSTRACT EVAs will be frequent, potentially energetic, and performed after short in-suit PB; therefore, our design includes: 4 groups of 6 subjects exposed to hypobaric and mild hypoxic atmosphere in a hypobaric chamber. 48 h equilibration to 8.2 / 34 after a 3-h PB, which limits tissue N2 supersaturation on depress to 8.2 psia. 5 sequential simulated EVAs at 4.3 psia with 85% O2 by mask – repeated-measures, sequential statistical design. 6 h EVA duration – adequate to measure DCS and venous gas emboli (VGE) responses. 2 non-ambulatory groups undergo microgravity exercise and rest for about 0.45 L(STPD) / min O2 consumption. 2 ambulatory groups undergo planetary exercise and rest for about 1.0 L(STPD) / min O2 consumption. 2 technicians monitor subjects for VGE using Doppler ultrasound bubble detector at about 15 min intervals. Day of rest between EVA days. Type I DCS symptoms are treated in the hypobaric chamber (TBD), with return-to-duty per JPR 1800.3. Results must meet current accept requirements: ≤ 15% incidence of Type I DCS, ≤ 20% incidence of Grade IV VGE, both at 95% confidence, and no Type II DCS, otherwise reject at 70% confidence to stop ineffective testing. RESULTS 12 N2 Kinetics: ASSUMPTION 1 11 10 9 8 start EVA 7 6 1 2 3 4 Fig. 4. The P(DCS) from survival model increases with age in a 6-hr simulated ambulatory EVA, and not as much under a non-ambulatory condition. We do not have an estimate of P(DCS) for a simulated ambulatory planetary EVA at higher metabolic rate. The effect of age on P(DCS) is modest with uncertainty provided by the 95% CL. 5 5 4 3 • Multiple assumptions seen above in the design of a new PB protocol requires empirical validation – computations only provide guidance about design. 2 1 76 .5 10 2. 0 12 7. 5 15 3. 0 17 8. 5 20 4. 0 22 9. 5 25 5. 0 51 .0 25 .5 0. 0 0 • DCS is minimized while simultaneously conserving O2 if the nitrogen partial pressure (PN2) in the habitat approaches the 4.3 psia suit pressure. • However, a low PN2 results in an unacceptably high PO2 at 14.7 psia, so total saturation pressure (PB) must be reduced. • Operational, medical, safety, and engineering trades resulted in a candidate habitat atmosphere at 8.2 psia with 34% O2 and 66% N2, resulting in a mildly hypoxic PO2 of 2.78 psia with a favorable PN2 of 5.41 psia (5,6). 1.0 0.9 Fig. 2. Computed tissue P1N2 decreases during initial 3-hr mask PB at 14.7 psia and then during subsequent 48 hrs at 8.2 psia while breathing a PN2 of 5.4 psia. Subject dons a mask and breathes 85% O2 during 19 min depressurization (2-min to 6.0 psia, 15 min hold at 6.0 psia, then 2-min to 4.3 psia) to 4.3 psia. Computed tissue P1N2 decreases during the 6-hr simulated EVA (EVA time starts 8 min at 6.0 psia) and then increases during the rest interval between EVAs back at 8.2 psia. The computed P1N2 is approximately 5.23 psia at the start of each EVA, giving a tissue ratio (TR) of 1.21 as a measure of decompression stress for the EVA simulation. 31 29 27 bubble growth index • Extravehicular activities (EVAs) at remote locations must conserve O2, minimize in-suit prebreathe (PB) time, and minimize decompression sickness (DCS) during repeated exposures so as to minimize treatment resources. 25 Tissue Bubble Dynamics Model (3): ASSUMPTION 2 end EVA 1 2 3 4 5 23 21 19 17 15 13 11 9 7 Fig. 5. 20-foot diameter hypobaric chamber at JSC is one facility capable of supporting a multi-day, 24/7 test program with humans in enriched O2 environment. 3 0.7 0. 5 0.8 76 .5 10 2. 0 12 7. 5 15 3. 0 17 8. 5 20 4. 0 22 9. 5 25 5. 0 51 .0 25 .5 0 1 time from start of prebreathe (hrs) 0.6 8.2 psia with 0.34 FIO2 0.5 0.4 Fig. 3. A computed TR of 1.21 at the start of each simulated EVA is associated with a computed bubble growth index (BGI) of ~ 24 at the end of 6-hr simulated EVAs. BGI then returns to baseline during the rest interval between EVAs back at 8.2 psia. TR is the ratio of P1N2 / PB at the start of EVA and BGI is the ratio of final bubble radius after 6 h to initial 3 µm micronuclei radius. curve of isoburning rate 0.3 0.2 DCS Survival Model (1): ASSUMPTION 3 0.1 0.0 • Our design is based on nominal values, for example, P1N2, TR, and BGI, but each subject brings particular combinations of variables that dictate the likelihood of DCS and VGE. time from start of prebreathe (hrs) INTRODUCTION FIO2 • • • • • • • • • • • computed P1N2 (psia) INTRODUCTION: Extravehicular activities (EVAs) at remote locations must maximize limited oxygen (O2) resources and minimize the risk of decompression sickness (DCS). The proposed denitrogenation protocol requires subjects to live in a mildly hypoxic atmosphere at 8.2 psia while performing repetitive EVAs at 4.3 psia. Empirical data are required to confirm that any new protocol meets accept requirements: ≤ 15% incidence of Type I DCS, ≤ 20% incidence of Grade IV venous gas emboli (VGE), both at 95% statistical confidence, with no Type II DCS symptoms. METHODS: A repeated-measures, sequential statistical design is envisioned, in which 4 groups of 6 subjects with physical characteristics similar to active-duty astronauts first equilibrate over 48 hrs to an 8.2 psia atmosphere in a hypobaric chamber containing 34% O2 and 66% nitrogen (N2), and then perform repeated simulated 6-hr EVAs at 4.3 psia over the next 11 days. Two of the groups would simulate EVA work in microgravity, whereas the other 2 groups simulate EVA work on a planetary surface. The hypoxia at 8.2 psia is equivalent to breathing air at a 1,220 m (4,000 ft) altitude, an inspired O2 partial pressure (PIO2) of 128 mmHg. The same mildly hypoxic PIO2 was experienced in the shuttle 10.2 psia – 26.5% O2 staged and the current ISS campout denitrogenation protocols. For simulated EVAs, each subject dons a mask and breathes a normoxic mixture of 85% O2 and 15% N2, a PIO2 of 149 mmHg, while at 4.3 psia. Subjects follows a prescribed repetitive activity against loads in the upper and lower body to simulate nonambulatory work in a microgravity environment or ambulatory work in a planetary environment. Doppler ultrasound (2.5 mHz) monitoring for VGE in the pulmonary artery is performed on subjects by 2 Doppler technicians at about 15-min intervals while at 4.3 psia, then repressurization returns all to 8.2 psia and the cycle is repeated 4 additional times with a day of rest between simulated EVAs. RESULTS: At one extreme, considering independent exposures, our accept criterion for DCS permits 4 cases of Type I DCS in 60 exposures (6.6% observed). However, we account for dependency so if the best estimate of P(DCS) is 0.5% for the microgravity EVA simulation, then 12 subjects repeated 5 times has > 95% probability of meeting the accept condition. If the best estimate of P(DCS) is 2.7% for the planetary EVA simulation, then there is a 89% probability of meeting the accept condition. DISCUSSION: Many assumptions go into the design of a new prebreathe protocol, so validation with human trials is required. Our current DCS survival model calculates a low probability of DCS of 0.5% (0.3 to 1.2%, 95% CL) for each EVA for physically active nonambulatory subjects and 2.7% (1.5 to 4.9%) for physically active ambulatory subjects. DISCUSSION P(DCS) = 1 / (1+exp(-(ln(t) – 10.226 + 0.0132×BGI + 4.097×TR + 0.0241×AGE + 1.267×AMB – 0.0642×BMI) / 0.745)), 0 2 4 6 8 10 pressure (psia) 12 14 Fig. 1. The rate of combustion of common materials (paper, cotton) is similar along the curve of isoburning rate. An atmosphere at 8.2 psia with 34% O2 is not in the region of increased rate of combustion. Curve adapted from (2) with additional reference to (8). where t is in hrs from start of exposure, BGI is bubble growth index from the TBDM, TR is at start of altitude exposure, AGE is in years, ambulation status (AMB) is either 1 or 0, and BMI is body mass index, the ratio of mass in kg divided by height in meters2. • P(DCS, microgravity sim) = 0.005, AMB = 0, t = 6, BGI = 24, AGE = 32, BMI = 24, and TR = 1.21. • P(DCS, planetary sim) = 0.027, AMB = 1, t = 6, BGI = 24, AGE = 32, BMI = 24, and TR = 1.21. TABLE 1. Gas Partial Pressures in Proposed Habitat condi&on PB (psia) FIO2 PN2 (psia) PO2 (psia) PIO2 (psia) sea level 14.7 0.210 11.6 3.09 2.90 shu9le staged and ISS campout prebreathe 10.2 0.265 7.48 2.70 2.45 proposed habitat 8.2 0.340 5.41 2.78 2.47 FIO2 is dry-gas fraction of inspired O2. PIO2 = (PB – 0.91) × FIO2. • Empirical data are required to confirm that a new denitrogenation protocol meets the current accept requirements per NASA STD 3001, Vol. 1. www.nasa.gov Statistical Considerations: ASSUMPTION 4 • At one extreme, considering independent exposures, our accept criterion for DCS permits 4 cases of Type I DCS in 60 exposures (6.6% observed). • Based on few data (4,7) about repeated DCS outcomes during hypobaric exposure, an estimated standard deviation of 1.4 was used for the between-subjects random component of P(DCS) on a logit scale. • Simulations have shown that for 12 subjects, each completing 5 simulated EVAs (60 total exposures), the probability of accepting the prebreathe protocol ranges from 63.8% (planetary scenario: P(DCS) = .049) to 97.8% (microgravity scenario: P(DCS) = .012). But these estimates are conservative because they were made using upper confidence limits for P(DCS) based on fitting the log logistic DCS survival model. • Instead, using the point estimate of P(DCS) = 0.027 for the planetary scenario, the probability of accepting the protocol would be 88.8%. For the microgravity scenario, the point estimate of P(DCS) = 0.005, in which case acceptance would be a virtual certainty. Fig. 6. Artist conception of planetary exploration where safe and efficient EVAs are the key to mission success. • Prospective research with test subjects maximizes safety and mission success for astronauts. REFERENCES 1. Conkin J, Abercromby AFJ, Dervay JP, Feiveson AH, Gernhardt ML, Norcross JR, Ploutz-Snyder R, Wessel JH III. Hypobaric decompression sickness treatment model. Aviat Space Environ Med 2014 (in review). 2. Forsyth ET. Determining water suppression rates in hypobaric chambers. Johnson Space Center and White Sands Test Facility, Report TR-782-001, July 26, 1996. 3. Gernhardt M.L. (1991) Development and Evaluation of a Decompression Stress Index Based on Tissue Bubble Dynamics [dissertation]. Philadelphia: University of Pennsylvania. 4. Kumar KV, Waligora JW, Gilbert JH III. The influence of prior exercise at anaerobic threshold on decompression sickness. Aviat Space Environ Med 1992; 63:899-904. 5. NASA Exploration Atmospheres Working Group, "Recommendations for exploration spacecraft internal atmospheres: The final report of the NASA exploration atmospheres working group. NASA Technical Publication NASA/TP-2010-216134," NASA Technical Publication , 2010. 6. Norcross J, Norsk P, Law J, Arias D, Conkin J, Perchonok M, Menon A, Huff J, Fogarty J, Wessel JH, III, Whitmire S. Effects of the 8 psia / 32% O2 atmosphere on the human in the spaceflight environment. NASA Technical Memorandum NASA/ TM-2013-217377, Johnson Space Center, June 2013. 7. Weathersby PK. Individual susceptibility to DCS. In: The Physiological Basis of Decompression. Vann RD (ed). Thirty-Eighth Undersea and Hyperbaric Medical Society Workshop. Bethesda, MD; 1989:372-373. 8. West JB. Fire hazard in oxygen-enriched atmospheres at low barometric pressures. Aviat Space Environ Med 1997; 68:159-62.