Challenge of Conducting Trials of
Neuroprotection in the Asphyxiated
Term Infant
Seetha Shankaran* and Abbot Laptook†
There has been much progress in understanding the pathogenesis of hypoxic-ischemic brain injury in
the near-term and term infant. Although gaps in our knowledge base persist, advances over the past
two decades have led to the development of specific brain oriented therapies directed at critical
events contributing to tissue damage. The primary goal of these interventions is to prevent or
attenuate neurologic and developmental sequelae of brain injury. Examples of current potential
treatments include modest reductions in brain temperature, receptor antagonists of excitatory
neurotransmitters, reductions in O2 free radicals, blockade of inflammatory mediators, and inhibition
of apoptotic pathways. At present, some of these treatments have sufficient animal data that
demonstrate benefit, to justify moving experiments from the laboratory to the clinical arena. Modest
hypothermia represents the neuroprotective intervention that has been investigated in the most
complete fashion for the newborn, and there are multiple ongoing clinical trials testing its efficacy.
This review will address specific challenges that are pertinent to the evaluation of any neuroprotective
therapy implemented shortly after birth. Specific issues to be covered include the therapeutic
window, establishing a diagnosis of hypoxic-ischemic encephalopathy, patient selection, characteristics of an effective therapy, safety considerations, appropriate outcome variables, and sample size
considerations. Since clinical trials of brain hypothermia are in progress, many of these issues will be
addressed from the perspective of this specific intervention.
© 2003 Elsevier Inc. All rights reserved.
europrotection for infants at risk for brain
injury appears to be one of the most innovative and promising therapies to be introduced in
the coming decade. The challenges that are found
with this intervention are reviewed in this article.
N
Therapy as Protection or Resuscitation
One of the major challenges in successfully implementing a neuroprotective therapy is the
time of initiation of the intervention. In general,
neuroprotective therapies are more effective
when used as protection rather than resuscitation. A protective therapy is a treatment that is
initiated before a potential adverse event, and
thus requires knowledge of the time when a
From the *Department of Pediatrics, Wayne State University, Detroit,
MI; and †Department of Pediatrics, University of Texas Southwestern Medical Center, Dallas, TX.
Address reprint requests to Seetha Shankaran, MD, Children’s Hospital of Michigan, 3901 Beaubien Blvd, Detroit, MI 48201; e-mail:
sshankar@med.wayne.edu.
© 2003 Elsevier Inc. All rights reserved.
0146-0005/03/2704-0008$30.00/0
doi:10.1016/S0146-0005(03)00047-8
320
patient would be at high risk for a cerebral
insult. For example, infants undergoing cardiopulmonary bypass surgery for correction of complex congenital heart disease represent an ideal
population for implementation of treatment as
protection. A resuscitative therapy is a treatment
that is initiated after a potential adverse event
because the possibility for a cerebral insult could
not be anticipated. A resuscitative strategy is applicable to the term infant who has incurred a
hypoxic-ischemic interval proximate to delivery.
Although the incidence of peri-partum hypoxiaischemia is difficult to estimate, the relative infrequency (approximately 1-2 cases/1,000 live
births)1,2 and unanticipated nature of the responsible events, make detection prior to hypoxia-ischemia usually impossible. Even when
there is a high index of suspicion for clinically
important hypoxia-ischemia prior to delivery
(eg, possible uterine rupture or abruptio placenta), time constraints limit initiation of therapies in a clinical setting. Although less common, unanticipated catastrophic hypoxic-ischemic
events may occur following delivery (eg, tension
Seminars in Perinatology, Vol 27, No 4 (August), 2003: pp 320-332
Neuroprotection in Asphyxiated Term Infants
pneumothorax, obstructive airway lesions) and
would be amenable to a resuscitative strategy.
Given that neuroprotective therapies for the
term newborn will need to be initiated as resuscitation, the goals should be to initiate the intervention in as short a period of time following the
putative hypoxic-ischemic event. The interval of
time after an hypoxic-ischemic event for which a
neuroprotective intervention can be implemented with demonstrable efficacy is the therapeutic window. In general, there is decreasing
efficacy of neuroprotective treatments the further into the therapeutic window treatment is
started. For clinicians caring for critically ill infants following peri-partum hypoxia-ischemia,
there are important practical considerations that
temper when a brain oriented therapy can be
introduced. Relevant to hypoxia-ischemia, initial
management needs to prioritize stabilization of
the airway if intubated, adjustment of ventilator
support, establishment of intravenous and/or
arterial vascular access, correction of acid-base
disturbances, insurance of adequate perfusion
pressure, and maintenance of a normal blood
glucose concentration. Once the infant is adequately stabilized, attention needs to be focused
on establishing a diagnosis of hypoxic ischemic
encephalopathy, and determining if the severity
warrants exposure to the risks associated with
the potential therapy. Thus, the sequence of
stabilization followed by evaluation delays initiation of brain specific treatments, but probably
insures a more accurate neurologic assessment
since the latter often changes over the first hours
after birth.
Evidence for a Therapeutic Window
There is sound experimental evidence using animal models that a therapeutic window exists for
perinatal animals. At present modest brain cooling is the most effective intervention for hypoxia-ischemia, and has thus led to its use to
examine the therapeutic window. Although the
number of studies that show the presence of a
therapeutic window in the perinatal period is
limited relative to adult investigations, the available studies are extremely well done and convincing. The best studies addressing the therapeutic window were performed by Gunn et al3-5
and used in-utero sheep undergoing brain ischemia to test the therapeutic efficacy of brain
321
cooling. Cerebral hypothermia was achieved
with a cooling cap and was initiated at 1.5, 5.5, or
8.5 hours after ischemia and maintained for 72
hours. The degree of brain cooling is difficult to
judge since dura temperature was monitored,
but temperature gradients with this mode of
brain cooling insure that the outermost portion
of the cortex was the coolest.6 Cooling initiated
at 1.5 hours after ischemia reduced brain cytotoxic edema, improved preservation of electroencephalogram (EEG) activity, and decreased
the extent of neuronal injury on histologic examination.3 Benefit was also found when cooling
was initiated at 5.5 hours after ischemia but
the magnitude of the effect was attenuated.4
When brain cooling was initiated at 8.5 hours
after ischemia, a time when postischemic seizures commence in this model, neuroprotection
could not be demonstrated.5 Wagner et al,7 used
7 day rat pups undergoing hypoxia-ischemia to
show that a 7 °C reduction in brain temperature
initiated 2 hours after hypoxia-ischemia and
maintained for 26 hours resulted in brain tissue
rescue. The results are important since the presence of a therapeutic window is extended to
another species, and the neurologic benefit
(demonstrated by both magnetic resonance imaging [MRI] and behavioral assessments) is demonstrable at a time remote from the hypoxiaischemia (42 days).
Specific characteristics of how cerebral hypothermia is used will also influence the presence
and duration of the therapeutic window. For
example, the duration of the therapeutic window can be lengthened if the interval of postischemic brain cooling is increased. Consistent
with this are the reports of Gunn et al3-5 noted
above, and the observations from newborn swine
that a post-ischemic interval of only 1 hour does
not result in neuroprotection even with a short
delay before cooling.8 From the available literature, it appears that a duration of brain cooling
between 24 to 72 hours is necessary.3-5,7 Also
evident from the available studies is the concept
that cerebral hypothermia is more effective the
earlier it is started after hypoxia-ischemia. However, a recent study by Taylor et al9 differs from
this concept. Specifically, 14 day rat pups were
used to examine 6°C brain temperature reductions when initiated at intervals of 2, 4, or 6
hours after hypoxia-ischemia and maintained
for only 6 hours. Surprisingly, cooling initiated
322
Shankaran and Laptook
at 6 hours postinsult led to a better outcome
compared to cooling initiated earlier. The authors speculate that there may be a window of
time following hypoxia-ischemia when hypothermia affects the most critical pathways, and thus
obviates the need for an earlier start and longer
interval of cooling. Although provocative, these
observations need to be confirmed.
Direct evidence to support the presence of a
therapeutic window in human infants at term
does not exist. The best available evidence to
suggest the presence of a therapeutic window is
the observations of Hope et al.10 These investigators examined cerebral energy metabolism using sequential P31 magnetic resonance spectra of
brain from 10 infants with birth asphyxia. Six of
the 10 infants were studied in the first 24 hours
of life and their spectra were similar to normal
infants; subsequently, all infants demonstrated
changes in high energy phosphorylated metabolites (principally reductions in phosphocreatine and elevations in inorganic phosphorus).
The observation that changes in cerebral energy
state occur after some interval after birth asphyxia suggests that there is a window of time
when neuroprotective therapies could be initiated and be effective.
Selection of Patients for Neuroprotection
Translating preclinical studies to the clinical setting is challenging because of the following: 1)
Animal models vary in cortical, white matter and
deep gray matter structural development when
compared with the human neonate; 2) Postinjury rescue treatment seems to be the only feasible approach with acute perinatal asphyxia; 3)
The potential window of rescue neuroprotection
in perinatal animal models seems to be 6 hours
after a timed injury; 4)4 In the human neonate,
neither the timing nor the severity of the hypoxic-ischemic injury is known; and lastly a single therapeutic agent or approach may impact
only 1 step or steps in the cascade of events after
a hypoxic-ischemic event; therefore a multitreatment approach may be needed.
Early identification of acute encephalopathy
is crucial in view of the therapeutic window and
identification of infants at high risk for neurological morbidity needs to be accurate to minimize the risk of potential therapies. Encephalopathy, which generally evolves over 2 to 3 days, is
the best predictor of long-term outcome. A combination of abnormal physiologic and biochemical markers have been used with or without
encephalopathy in the immediate newborn period to identify infants at risk for brain injury.
The most common parameters used in newborn
assessments are as follows:
Apgar score. Very low and persistently low Apgar scores are associated with a high mortality
rate and cerebral palsy in survivors. Moderately
low scores and scores that improve between 1
and 5 minutes do not correlate with later neurological outcome.11 Apgar scores are lower in
neonates with seizures, compared to controls.12
In a study evaluating the relationship of Apgar
score to encephalopathy, a score of 0-3 at minute
was significantly related to encephalopathy.13
However, a low Apgar score may reflect not only
hypoxia-ischemia, but also lack of tolerance to
labor by a fetus compromised by prenatal disease, medications received by the mother, fetal
malformations, and neuromuscular and cardiopulmonary disease in the neonate.14
Fetal heart rate patterns. No specific pattern of
fetal heart rate abnormalities has been found
that is predictive of neurological abnormalities.15,16 Multiple late decelerations and lack of
beat-to-beat variability of the fetal heart rate pattern are associated with an increased risk for
cerebral palsy.17 Term infants with encephalopathy have been shown to have absence of fetal
heart rate accelerations and low variability compared to control infants with no encephalopathy.18 However, these findings have low sensitivity and specificity.
Acid base status. An association between umbilical artery pH ⬍7.0 and low 1 and 5 minute
Apgar scores, neonatal seizures and death has
been noted in a large series of consecutively
studied term infants.19 Mixed or metabolic acidosis, rather than respiratory acidosis, appears to
correlate with complications in the neonate.20
Neonatal morbidity has been shown to increase
with every 0.10 decrement in pH.21 A pH of 7.0
appears to reflect the degree of acidosis below
which end organ dysfunction is detected among
term infants with fetal distress and newborn depression.22 Umbilical arteriovenous pH, pCO2
and pO2 differences have been correlated with
neonatal morbidity and neurologic injury in
term infants with perinatal asphyxia.23 On the
other hand, term and near term infants born
Neuroprotection in Asphyxiated Term Infants
with an umbilical arterial pH ⱕ7.0 who are clinically stable at birth and are admitted to a nonintensive care setting do not have manifestations
of hypoxia-ischemia in the newborn period.24
Unanticipated acidemia in stable neonates may
be associated with induction of labor and epidural and spinal anesthesia.25,26 Furthermore,
acidemia at birth may reflect underlying disorders, including sepsis.14,27 Thus, pathologic fetal
acidemia alone does not accurately identify newborns with hypoxic-ischemic injury.
Neurological signs. In term infants, neurological
signs following acute asphyxia have been characterized by Sarnat and Sarnat28 as hypoxic-ischemic encephalopathy. Signs of central nervous
system injury evolve over 72 hours following the
insult with seizures occurring usually within 12
hours or hypotonia in the immediate neonatal
period. Neurodevelopmental outcome has been
correlated with the stage of encephalopathy.
The risk of death is 5% after moderate encephalopathy and 25%-60% after severe encephalopathy; the risk of severe handicap in survivors is
20% after moderate, and 50%-100% after severe
encephalopathy.29-31 The risk of cerebral palsy
after obstetrical complications is increased in
the presence of 3 or more signs of encephalopathy.32 However, encephalopathy has multiple
etiologies other than intrapartum asphyxia;
these include acute infections, intracranial hemorrhage, metabolic disorders, and developmental defects.33,34
Combination of clinical markers. Carter et al used
graded abnormalities of fetal heart rate monitoring, umbilical arterial base deficit, and 5 minute
Apgar score to predict risk for multiorgan injury.35 Perlman and Risser36 have shown that a
low 5-minute Apgar score, intubation in the delivery room, and severe fetal acidemia facilitated
early identification of asphyxiated infants at
greatest risk for developing seizures. Wayenberg37 evaluated the relationship between clinical and biochemical markers and the evolution
of moderate or severe encephalopathy over 72
hours: high base deficit and an abnormal early
neurological score at 30 minutes of age were
associated with moderate or severe encephalopathy. These 3 scoring systems have not been
validated by long-term follow-up studies. On the
other hand, Ekert et al38 have predicted shortterm outcome at a year of age in asphyxiated
term infants with data available within 4 hours of
323
age. Death or severe impairment at a minimum
of 12 months of age was associated with the
following: delayed onset of breathing ⬎10 minutes after birth, administration of chest compressions at birth and seizures within 4 hours of age.
Neurophysiologic markers of brain injury. Electrical
background activity is more predictive of outcome in infants than the presence or absence of
seizure activity.39,40 However, conventional multichannel recordings are too cumbersome and
are not readily available in the clinical setting.
The amplitude integrated EEG (aEEG) is a simplified form of continuous EEG monitoring that
gives an overall impression of cerebral cortical
activity. The aEEG records a single channel from
biparietal electrodes and is easy to apply at the
bedside. There is good correlation between the
aEEG and conventional EEG.41,42 In studies evaluating aEEG and outcome, descriptions of aEEG
have included both minimum and maximum
voltage and the pattern of the aEEG. The aEEG
patterns have been grouped into 5 categories as
follows: 1) Continuous normal voltage pattern
(CNV) with maximum voltage 10-50 V with
periods of increased variability due to sleep; 2)
Discontinuous normal voltage (DNV) with more
continuous normal voltage with periods of intermittent low voltage; 3) Discontinuous background pattern of burst suppression (BS) with
periods of very low voltage intermixed with
bursts of higher amplitude; 4) Continuous low
voltage (CLV) around or below 5V; and E)
Very low voltage with activity below 5V, known
as flat tracing (FT).42,43 A CNV aEEG pattern is
predictive of good outcome, and almost all asphyxiated full term infants with FT patterns either die or develop sequelae. Al Naqeeb et al44
classified the aEEG background in neonates with
encephalopathy in a more simplified manner
that included normal amplitude (upper margin
of band of aEEG activity ⬎10V and lower margin ⬎5V), moderately abnormal amplitude
(upper margin ⬎10 V and lower ⱕ5 V), and
suppressed amplitude (upper margin ⬍10V
and lower margin ⬍5 V). The aEEG appears to
be a good predictor of neurodevelopmental outcome for the infants studied within 12 hours of
birth with a sensitivity of 1.0, specificity of 0.82, a
positive predictive value of 0.85 and a negative
predictive value of 1.0.
The efficacy of measuring cerebral function
within the first 6 hours of life by aEEG was
324
Shankaran and Laptook
demonstrated in a study of 47 infants by Hellström-Westas.45 The ability to predict a normal
outcome after a normal tracing or a poor outcome with an extremely low voltage reading
were 91%, although the burst suppression pattern was less predictive. The predictive value of
the aEEG is better at 6 hours of age than at 3
hours in studies evaluating outcome from 1-6
years.43 At 3 hours, the sensitivity and specificity
of the BS pattern together with FT and CLV was
85% and 77%, respectively, while at 6 hours it
was 91% and 86% respectively. Using the criteria
at 3 hours for a neuroprotective intervention
would result in unnecessary treatment in a small
percentage of cases; on the other hand, some
infants would not be offered treatment.46
The pitfalls and caveats encountered with
aEEG monitoring have been reviewed by Hellström-Westas.47 Artifacts can occur during the
study readings with a loose electrode, gasping
respirations, high-frequency ventilation, or nonoptimum head position. Readings may be dampened because of a subgaleal hemorrhage or may
be asymmetric due to intraparenchymal infarcts.
Groenendaal and de Vries46 suggest pattern recognition requires experience and they do not
advocate the use of absolute values alone.44
Recently, Shalak et al48 showed that aEEG
coupled with an early neurological examination
enhances prediction of term infants at risk for
persistent encephalopathy. Among 50 term infants with clinical and biochemical criteria of
acute intrapartum distress, an abnormal aEEG
using criteria of al Naqueeb44 had 89% specificity, 79% sensitivity and 73% positive predictive
value. An abnormal neurological examination
had 78% specificity, 78% sensitivity and 58%
positive predictive value; the combination of
neurological examination and aEEG had specificity of 94% and positive predictive value of
85%.
Other early markers of acute intrapartum asphyxia.
Cerebrospinal fluid (CSF) levels of interleukin 6
(IL-6) obtained within 8 to 90 hours of life have
been shown to be elevated in neonates with
brain damage (imaging or pathological evidence) after perinatal asphyxia or encephalopathy.49,50 In addition, IL-8 was also related to
the degree of hypoxic-ischemic encephalopathy
(HIE).50 CSF levels obtained within 6 hours of
birth (potential window of therapy) have shown
elevated interleukin 1 and tumor necrosis fac-
tor ␣ levels that correlated with outcome.51
Another early marker that has correlated with
hypoxic-ischemic encephalopathy is an elevated
urinary lactate to creatinine ratio evaluated
within 6 hours of age by proton nuclear magnetic resonance spectroscopy. The ratio of urinary lactate to creatinine ratio was also significantly higher in infants who had adverse
outcomes at one year.52 These markers may not
be available in a clinical setting.
The selection of neonates for neuroprotective
therapies is very challenging; using one set of
criteria (5 min Apgar ⬍6, blood pH of 7.00 or
less, and need for intubation and ventilation in
the delivery room)36 applied in a retrospective
manner to a population, Nelson and Grether53
showed that most infants eventually diagnosed
with CP had nonasphyxial conditions that may
have contributed to adverse neurological outcome. These conditions include maternal or
neonatal infection,33,54 abnormal coagulopathy
secondary to factor V Leiden mutation55,56 or
anticardiolipin antibodies in blood of mothers.57
However, it remains unknown whether the same
criteria applied prospectively in the neonatal
period would identify a high percentage of all
infants in a population with hypoxic-ischemic
injury.
Although there are many studies which have
examined the relationship between prenatal and
perinatal events and neurodevelopmental outcome, the largest database on this topic is derived from the National Collaborative Perinatal
Project (NCPP) with enrollment of more than
50,000 mother-infant dyads between 1959 and
1966. A high mortality rate occurred among
term infants with severe asphyxia, so relatively
small numbers of children with low Apgar scores
were evaluated at 7 years.11 If these children had
survived, a stronger relationship between perinatal asphyxia and poor outcome may have been
found.58 Given the advances in Obstetric and
Neonatal care, the cluster of perinatal events
associated with neonatal neurological dysfunction noted in NCPP32 need to be re-examined in
a current data set. In view of these constraints,
the ongoing trials of modest hypothermia are
using a combination of criteria to establish a
diagnosis and identify study candidates. These
criteria include indicators of an acute event (fetal acidemia or resuscitation after a sentinel
event around the time of delivery), and evidence
Neuroprotection in Asphyxiated Term Infants
of an acute encephalopathy. Some trials are also
employing the aEEG to confirm the clinical impression of encephalopathy.
Characteristics of an Effective Therapy for
Neuroprotection
There are a number of important characteristics
for an intervention to be successful as a possible
brain oriented therapy. This includes targeting
specific mechanisms mediating the pathogenesis
of tissue injury, ease of initiation within a limited
interval of time, maintenance of the therapy for
the necessary interval of time to optimize the
neuroprotective effect, and absence of frequent
and/or serious adverse events associated with
the therapy. Each of these points will be briefly
addressed.
Targeting specific mechanisms. Although the
pathogenesis of peri-partum brain injury is extremely complex and not completely understood, the initiating event often involves hypoxia-ischemia. Hypoxemia alone probably has
relatively little adverse effects on the brain provided that perfusion pressure is maintained.
This reflects the typical homeostatic adjustments
in cerebral blood flow characteristic of mammalian species.59 The latter maintains bulk O2 delivery to the brain, and consequently brain O2
consumption. Similarly, ischemia without alteration of respiratory gases (ie, alterations in perfusion pressure and blood flow only) is a relatively uncommon event in the term infant and
most often occurs in the absence of an identifiable precipitating event or condition.60 Rather it
is the combination of hypoxia and ischemia that
initiates a complex cascade of events contributing to brain injury. Although the proximate
cause for hypoxia-ischemia is evident for some
infants (eg, impaired placental gas transport due
to an abruption, cord accident), the association of
brain injury with inflammatory conditions suggests
that triggering pathways to injury may be more
complicated than previously thought.54,61,62
Given these caveats, brain energy failure after
hypoxia-ischemia is associated with 2 phases of
pathologic events that culminate in brain injury.
These phases have been well described in newborn animals and are termed primary and secondary energy failure based on characteristics of
the cerebral energy state used to describe the
temporal sequence.63 The tie between hypoxia-
325
ischemia and brain injury is the initiation of
multiple mechanisms contributing to injury,
with varying links between mechanisms. Important pathways contributing to perinatal brain
injury include excessive exposure to excitotoxic
neurotransmitters,64 free radical damage,65 inflammation,66 and excessive apoptosis.67 Other
mechanisms such as defective osmoregulation
and inhibition of protein synthesis68 have been
addressed in adult but not perinatal animals.
Ideally prevention of hypoxia-ischemia is the
most effective strategy for this form of brain
injury, but is usually not feasible under real
world conditions. Neuroprotective strategies
thus need to focus on downstream events from
the putative hypoxia-ischemia. Neuroprotective
therapies can either be specific or nonspecific
with respect to a mechanism that prevents or
attenuates the extent of brain injury. An example of a specific neuroprotective therapy is MK801.69 This drug noncompetitively blocks the
N-methyl-D-aspartate receptors and effectively
inhibits the neurotoxicity associated with excessive release of excitatory neurotransmitters during hypoxia-ischemia. Another example is the
use of rhIL-1ra to protect against cerebral infarction after hypoxia-ischemia.70 The latter is an
interleukin-1 receptor antagonist and supports
the concept that inflammatory mediators play an
important role in the pathogenesis of hypoxicischemic brain injury. Although specific neuroprotective treatments are efficacious in the experimental setting of hypoxia-ischemia, it
remains unknown if one pathway is more predominant than others after hypoxia-ischemia in
human infants. Furthermore, characteristics of
the infant, such as genetic predisposition,
growth parameters, or preconditioning, are
likely to influence which mechanistic pathway(s)
has the greatest influence on outcome.
Until there is a better understanding of the
interplay among the multiple mechanisms of
injury for specific clinical conditions, a good
rationale could be made for the use of a nonspecific neuroprotective therapy. The latter
strategy would involve treatments that affect
multiple mechanistic pathways contributing to
brain injury. Modest brain hypothermia is the
prototypical example of a non-specific neuroprotective therapy. A relatively small reduction
in brain temperature (1-6°C) of neonatal animals is associated with better maintenance of the
326
Shankaran and Laptook
cerebral energy state during and immediately
after ischemia,71 attenuation of the release of
excitatory neurotransmitters.72 and decreased
caspase-3 activation and morphologic evidence
of apoptosis.73,74 Other neuroprotective effects
of cerebral hypothermia have been shown in
adult animals and include normalization of the
decrease in protein synthesis,68 reduction of free
radicals,75 and modulation of microglial activation and cytokine production.76 The net effect
of modest hypothermia on multiple pathways
is an attenuation of secondary energy failure77
and the neuroprotective benefits previously
cited.3-5,7,9 These considerations also raise the
possibility that combinations of therapies (nonspecific and/or specific treatments) may be a
reasonable approach for future clinical trials.
Ease/time of treatment initiation. An important aspect of neuroprotective therapies is the time
window available to initiate treatment. Although
the duration of the therapeutic window is not
precisely known for human infants, animal data
summarized above suggests that it is in the order
of hours. Thus, treatment needs to be initiated
in a short interval of time. Intravenous pharmacological therapy is attractive because of the rapidity and ease of medication administration. A
potential limitation to pharmacological therapy
is that therapeutic concentrations must be rapidly achieved throughout the brain tissue. The
blood-brain-barrier has always posed a potential
limitation to the effectiveness of drug therapy
for the central nervous system. Traditionally, development of new drug therapies has focused on
the drug-activity relationship, ie, the drug-receptor interaction, and there has been markedly less
attention to the structure-transport relationship,
ie, membrane permeation.78 Carriers will be
needed to insure transport across the blood
brain barrier unless compounds are lipid soluble
and of low molecular weight. An additional concern for the newborn is that maturational differences will prohibit ready extrapolation of experiences from adults to neonates.
In contrast, modest hypothermia represents a
therapy that can be implemented easily, rapidly,
and the extent of brain temperature reduction
can be assessed.6 In pilot animal studies performed for the National Institute of Child and
Human Development (NICHD) clinical trial of
whole body hypothermia for perinatal asphyxia,
the implementation of a cooling regimen and
relationship between systemic and brain temperature was evaluated.79 Three miniature swine
were instrumented and ventilated, and temperature probes were placed in the esophagus and
the brain (1 cm and 2 cm beneath the parietal
cortical surface and on the dura). Body cooling
was achieved by having the animals lay on a
cooling blanket interfaced with a commercially
available cooling system (Blanketrol II HyperHypothermia system, Cincinnati Sub-Zero Products, Cincinnati, OH). This system allows for
temperature control using an automatic control
mode (servo), and the esophageal temperature
was servo regulated between 38-39°C during
baseline conditions. During whole body cooling
esophageal temperature was servo controlled to
33.5°C, and the target temperature was reached
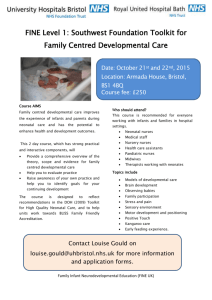
within 90 min of initiation of whole body cooling, and maintained for up to 6 hours. The table
shows the difference in temperature between
the esophagus and each brain region assessed.
The small difference in temperature between
the esophagus and the brain at a 2 cm depth
indicates that the esophageal temperature is an
excellent index of core brain temperature during normothermic and hypothermic conditions,
and that whole body hypothermia cools the entire brain. Furthermore, the servo control mechanism provided automatic adjustments in temperature of the cooling blanket to maintain
esophageal and thus brain temperature at the
set point.
The animal observations were used as the
methodological basis for a pilot study of either
normothermia or modest hypothermia in term
infants with encephalopathy at birth.79 The target esophageal temperature was 34.5°C and was
achieved within 30 minutes, followed by an overshoot of 1-1.5°C, with stabilization of the esophageal temperature at the set point by 90 min of
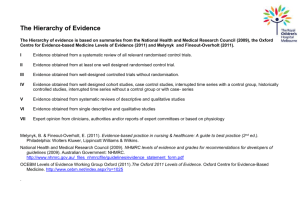
cooling (see Fig 1). Preliminary analysis of the
main trial (esophageal temperature set point of
33.5°C) indicates that achievement of the target
esophageal temperature also occurs within 90
min. The Blanketrol Hyper-Hypothermia (Cincinnati Sub-Zero Products) system is simple to
use, effectively lowers body and brain temperature, and requires no adjustments from the bedside provider.
Maintaining the neuroprotective intervention. The
duration that a neuroprotective intervention
needs to be continued for optimal efficacy re-
327
Neuroprotection in Asphyxiated Term Infants
Figure 1. (A) Temperatures of the esophagus and
(B) abdominal skin are plotted for the normothermic
group (open triangles) and the hypothermic group
(closed circles). Values are mean ⫾ SD. Normothermic infants were servo controlled at 36.5C using the
abdominal skin as the control site , and the hypothermic infants were servo controlled at 34.5C using the
esophageal temperature as the control site. The hypothermic group was rewarmed after 72 hours of
cooling.
mains uncertain. What appears to be certain is
that progression to secondary energy failure signifies irreversible development of brain injury.
In neonatal animals secondary energy failure
occurs between 24 to 48 hours after hypoxiaischemia.63 Furthermore, study of brain ischemia in fetal sheep has delineated the temporal
sequence of the accumulation of neurotransmitters and nitric oxide in the extracellular space,
EEG activity, and cortical impedance.80 After the
acute changes of ischemia have subsided, there
are prolonged elevations in excitatory neurotransmitters, indices of nitric oxide synthesis,
and decreases in cerebral impedance, suggesting that treatment may need to be continued for
up to 72 hours.
If pharmacological interventions are used to
achieve neuroprotection, the pharmacokinetics
to maintain therapeutic concentrations in the
brain tissue for some interval of time will need to
be understood, in addition to transport across
the blood-brain-barrier. Hypoxic-ischemic involvement of organs such as the kidney and liver
may affect the pharmacokinetics. Cerebral hypothermia is an appealing therapy that obviates
many of these issues. The use of esophageal
temperature to guide brain cooling provides a
convenient, minimally invasive, and reasonably
accurate index of core brain temperature (Table
1). Results from the NICHD Neonatal Network
pilot study of whole body cooling (Fig 1) showed
that esophageal temperature could be controlled to a desired target temperature (34.5°C
for the pilot) and maintained constant over 72
hours using the servo control mode of the Blanketrol Hyper-Hypothermia system (Cincinnati
Sub-Zero Products).79 There are some important caveats to these observations when monitoring cerebral hypothermia that are dependent
upon the mode of brain cooling. If brain hypothermia is achieved by cooling the body, the
brain is uniformly cooled with minimal temperature gradients from the core to the periphery,
episodes of hypoxia do not alter brain temperature, and systemic temperature is a good index
of brain temperature.6 In contrast, if brain hypothermia is achieved by selectively cooling the
head, there are prominent temperature gradients from the warmer core to the cooler periphery, hypoxia does alter brain temperature, and a
single systemic temperature site cannot provide
a valid index of brain temperature. Finally, if the
clinical course is complicated by brain ischemia,
systemic temperature will not be an accurate
index of brain temperature irrespective of the
mode of brain cooling.6,81
Safety of the neuroprotective intervention. The issue
of safety is pertinent to any neuroprotective intervention irrespective of the mechanism of action. The ideal treatment would be efficacious
with minimal adverse effects. Efficacy and safety
are usually not completely appreciated for new
treatments undergoing clinical trials, because
clinical experiences that form the basis for a
definitive clinical trial are often cohort studies
or small trials without the power to adequately
assess outcome. Thus, entry criteria for the evaluation of any new therapy in sick infants needs
to identify the group at highest risk for brain
Table 1. Temperature Difference Between the
Esophagus and Specific Brain Sites
Temperature Difference (°C)
Esophageal - Brain 2 cm
Esophageal - Brain 1 cm
Esophageal - Dura
0.1 ⫾ 0.3*
0.4 ⫾ 0.5
1.1 ⫾ 0.9
*P ⬍ .001 for esophageal-Brain 2 cm v esophageal - Brain 1
cm and esophageal - Dura.
328
Shankaran and Laptook
injury to justify potential therapy associated
risks. Therapies such as modest hypothermia
and high dose barbiturates are attractive from
this perspective since there is an existent knowledge base regarding potential adverse effects.
Unless a therapy is recognized to have great
hazards from initial experiences, a randomized
clinical trial represents the optimal way to evaluate efficacy relative to complications. In this
regard, randomized multicenter trials should be
monitored by a Data Safety Monitoring Committee with safety and outcome data evaluated at
multiple intervals. Methods such as that of
O’Brien and Fleming permit multiple looks at a
fixed sample size while maintaining overall type
1 error rate, and sacrificing little in terms of
power.
Role of neuroimaging in trials of neuroprotection. The
value of CT scanning as a good prognostic tool
to evaluate subsequent neurological sequelae is
limited.82 Sensitivity and interobserver agreement are better with MRI and computer tomography rather than with sonography for detection
of ischemia or infarction.83 MRI is now emerging as a more sensitive and early indicator of
brain injury in neonates than computer tomography, especially when combined with EEG.84
Abnormal signal density seen in the posterior
limb of the internal capsule had a 100% positive
predictive value for abnormal outcome at 1 year
of age.85
Diffusion weighted MRI shows areas of injury
in the basal ganglia and thalami within 6 hours
of injury.86 MRI imaging in the neonatal period
can now predict type of CP seen at follow up:
children with postero-lateral lentiform nucleus
and ventro-lateral thalamic injury developed dyskinetic CP; those with extensive thalamic injury,
central region and hippocampal lesions developed spastic CP, while deep grey nuclei and
cortico-subcortical lesions in the central region
were associated with mixed CP.87 Proton magnetic resonance spectroscopy (MRS) at 6 days of
age in acutely asphyxiated infants correlated well
with 30 month outcome. The basal nuclei and
intervascular boundary zone NAA/choline ratio
were highest in the children with normal outcome and lowest with those with an abnormal
outcome; while the lactate to choline ratio was
lowest in the normal children and highest in
abnormal children.88 Positron emission testing
scanning at 4-28 days of age has now been shown
to correlate with neurological outcome; the lowest glucose metabolic rate was seen in the CP
group.89 Thus, imaging of the brain during
and/or after neuroprotective interventions will
be an important component in the clinical assessment of brain injury. However, there are
practical concerns with present technology (logistics of off-site imaging facilities, moving critically ill neonates) that may limit the role of
neuroimaging in any trial of brain oriented therapies.
Primary outcome and sample size considerations. The
primary outcome of a neuroprotective trial
should be the combined endpoint of death or
moderate or severe disability at an early age:18
to 22 months is the earliest age at which major
disability can be detected. All evaluations should
be performed by certified and trained individuals masked to intervention status. Neuromotor
disability may be based on the neurologic examination and functional disability by the Gross
Motor Function (GMF) classification.90 Psychometric testing can be based on the Bayley Scales
of Infant Development (BSID II; MDI and PDI
normal values 100 ⫾ 15, mean ⫾ SD). Auditory
and visual outcome should be assessed by specialists masked to intervention status. All outcome variables should be defined a priori.
Moderate disability can be defined as Bayley
MDI between 1-2SD below mean and one or
more of the following: Level 2 on GMF, deafness
with no amplification or seizure disorder.
Severe disability can be defined as any of the
following: Bayley MDI ⬎2SD below mean (⬍70),
GMF level 3-5, deafness requiring hearing aids
(⬎60 db) or bilateral blindness (⬍20/200 acuity).
Sample size estimates should be powered to
include a 10% rate of loss to follow-up. A reasonable effect size for a favorable neuroprotective effect would be the ability to detect a reduction to 30% from a 50% event rate of death or
disability. With a two-tailed type 1 error of 0.05,
power of 80%, the sample size is 100 infants per
group or 200 total. Multicenter studies are
needed because the number of term infants at
risk for neurologic dysfunction will be too few in
any single institution. The number of infants
who suffer irreversible neurologic damage is a
subset of infants who are subject to asphyxia at
birth; hence large numbers of infants need to be
screened.
Neuroprotection in Asphyxiated Term Infants
Duration of follow-up. A critical issue in evaluating efficacy of neuroprotective therapies is the
age of follow-up for the outcome of interest. All
the current trials evaluating hypothermia as a
neuroprotective strategy have the primary outcome as death or disability at 18 months of age.
This age is the earliest age at which major disability can be detected. To understand whether
hypothermia or any other neuroprotective treatment is beneficial, it is necessary to evaluate
relationship of intervention to early childhood
outcome because interventions may influence
not only major neurological sequelae detected
at 18 months, but also potential sequelae of
brain injury in childhood-behavior, learning,
fine motor development and psychosocial and
psychiatric outcomes. For example, the relationship between the degree of cooling in neuroprotective trials and outcome may be discernible
only on subtle outcome evaluations beyond 18
months. The expense of tracking infants over
long time intervals and the attrition in follow-up
are critical issues in determining the duration of
follow-up for the primary outcome variable.
There is some experience with long-term outcome after hypoxic-ischemic encephalopathy
during early childhood. At 5 years of age, surviving infants with moderate or severe encephalopathy tend to have either a normal gross motor
exam or severe disability.31 In this study, fifty
percent of survivors were multiply handicapped
with spastic quadriplegia, persistent seizure disorder, microcephaly and language delays. Only
9 of 24 survivors had a McCarthy General Cognitive Index (GCI) that was normal. Lack of
head growth at 3 months and persistent seizure
disorder correlated with GCI and verbal, perceptual performance, quantitative, memory and motor subscores ⬍2SD below the mean. Cordes91
also has showed that serial head measurements
during the first few months in term infants with
HIE predicts later microcephaly.
There are limited data on school age outcomes of nondisabled survivors. Robertson et
al30 focused on findings among children who
survived moderate neonatal encephalopathy
with gross-motor ability intact. Children from 2
birth cohorts, 1 born 1974-1979 and the other
born 1982-1986 were followed to 8-10 years and
compared to matched control groups. The frequency of disabilities (8% following moderate
HIE and 100% following severe HIE) was un-
329
changed between the 2 time periods. There
were no survivors without a disability following
severe neonatal encephalopathy. The nondisabled survivors of moderate neonatal encephalopathy had a significantly lower percentage
achievement to age for motor tasks including
everyday motor (walking, running), complex
motor (hopping, balance) and fine motor tasks.
Academic achievement (reading, arithmetic)
greater than one level below expected grade
level of comparison children was seen to be
significantly greater among nondisabled survivors of moderate neonatal encephalopathy and
full scale, verbal and performance IQ was also
significantly lower in the nondisabled survivors
of moderate neonatal encephalopathy in both
birth cohorts.
Undertaking long-term outcome such as
school age follow-up is ideal in evaluating brain
oriented therapies. If loss to follow-up can be
minimized, important issues to be considered
are the use of evaluation tools that allow comparison of outcomes across studies. This will include assessments of neurologic status and classification of impairments.92 Imaging studies
should be obtained at the early childhood examination. Domains to be tested in the children
should include verbal and performance IQ, attention, executive function, and visual and perceptual motor skills. In addition, parental IQ
and family support should be assessed. Last, the
cost-effectiveness of the intervention should be
examined.
References
1. Hull J, Dodd KL: Falling incidence of hypoxic-ischemic
encephalopathy in term infants. Br J Obstet Gynaecol
99:386-391, 1992
2. Thornberg E, Thiringer K, Odeback A, et al: Birth asphyxia: Incidence, clinical course and outcome in a
Swedish population. Acta Paediatr 84:927-932, 1995
3. Gunn AJ, Gunn TR, de Haan HH, et al: Dramatic neuronal rescue with prolonged selective head cooling after
ischemia in fetal lambs. J Clin Invest 99:248-256, 1997
4. Gunn AJ, Gunn TR, Gunning MI, et al: Neuroprotection
with prolonged head cooling started before postschemic
seizures in fetal sheep. Pediatrics 102:1098-1106, 1998
5. Gunn AJ, Bennet L, Gunning MI, et al: Cerebral hypothermia is not neuroprotective when started after postischemic seizures in fetal sheep. Pediatr Res 46:274-280,
1999
6. Laptook AR, Shalak L, Corbett RJT: Differences in brain
temperature and cerebral blood flow during selective
330
7.
8.
9.
10.
11.
12.
13.
14.
15.
16.
17.
18.
19.
20.
21.
22.
23.
24.
25.
Shankaran and Laptook
head versus whole body cooling. Pediatrics 108:11031110, 2001
Wagner BP, Nedelcu J, Martin E: Delayed postischemic
hypothermia improves long term behavioral outcome
after cerebral hypoxia-ischemia in neonatal rats. Pediatr
Res 51:354-360, 2002
Laptook AR, Corbett RJT, Burns DK, et al: A limited
interval of delayed modest hypothermia for ischemic
brain resuscitation is not beneficial in neonatal swine.
Pediatr Res 46:383-389, 1999
Taylor DL, Mehmet H, Cady EB, et al: Improved neuroprotection with hypothermia delayed by 6 hours following cerebral hypoxia-ischemia in the 14 day old rat.
Pediatr Res 51:13-19, 2002
Hope PL, Costello AM, Cady EB, et al: Cerebral energy
metabolism studied with phosphorus NMR spectroscopy
in normal and birth asphyxiated infants. Lancet II:366369, 1984
Nelson KB, Ellenberg JH: Neonatal signs as predictors of
cerebral palsy. Pediatrics 164:225, 1979
Holden KR, Mellits ED, Freeman JM: Neonatal Seizures.
1. Correlation of prenatal and perinatal events with outcomes. Pediatrics 70:165-176, 1982
Adamson SJ, Allesandri LM, Badawi N, et al: Predictors
of neonatal encephalopathy in full term infants. BMJ
311:598-602, 1995
Nelson KB, Emery ES: Birth asphyxia and the neonatal
brain: What do we know and when do we know it? Clin
Perinatol 20:327-344, 1993
Freeman R: Intrapartum fetal monitoring—A disappointing story. N Engl J Med 322:6214-6216, 1990
Rosen MG, Dickinson JC: The paradox of electronic
fetal monitoring; More data may not enable us to predict
or prevent infant neurologic morbidity. Am J Obstet
Gynecol 168:745-751, 1993
Nelson KB, Dambrosia JM, Ting TY, et al: Uncertain
value of electronic fetal monitoring in predicting cerebral palsy. N Engl J Med 334:613-618, 1996
Spencer JA, Badawi N, Burton P, et al: The intrapartum
CTG prior to neonatal encephalopathy at term: A casecontrol study. Br J Obstet Gynecol 104:25-28, 1997
Goldaber KG, Gilstrap LC, Leveno KJ, et al: Pathologic
fetal acidemia. Obstet Gynecol 78:1103-1107, 1991
Low JA, Panagiotopoulos C, Derrick EJ: Newborn complications after intrapartum asphyxia with metabolic acidosis in the term fetus. Am J Obstet Gynecol 170:10811087, 1994
Goodwin TM, Belai I, Hernandez P, et al: Asphyxial
complications in the term newborn with severe umbilical
acidemia. Am J Obstet Gynecol 162:1506-1512, 1992
Winkler CL, Hauth JC, Tucker M, et al: Neonatal complications at term as related to the degree of umbilical
artery acidemia. Am J Obstetrics Gynecol 164:637-641,
1991
Belai Y, Goodwin TM, Durand M, et al: Umbilical arteriovenous PO2 and PC02 differences and neonatal morbidity in term infants with severe acidosis. Am J Obstet
Gynecol 7813-7819, 1998
King TA, Jackson GL, Josey AS, et al: The effect of
profound umbilical academia in term infants admitted
to a newborn nursery. J Pediatr 132:624-629, 1998
Mueller MD, Bruhwider H, Schupper GK, et al: Higher
26.
27.
28.
29.
30.
31.
32.
33.
34.
35.
36.
37.
38.
39.
40.
41.
42.
43.
rate of fetal acidemia after regional anesthesia for elective cesarean delivery. Obstet Gynecol 90:125-130, 1997
Herbst A, Wolner-Hanssen P, Ingemarsson I: Risk factors
for acidemia at birth. Obstet Gynecol 90:125-130, 1997
Meyer BA, Dickinson JE, Chambers C, et al: The effect of
fetal sepsis on umbilical cord blood gases. Am J Obstet
Gynecol 166:612-617, 1992
Sarnat HB, Sarnat MS: Neonatal encephalopathy following fetal distress. Arch Neurol 33:696-705, 1976
Low JA, Galbraith RS, Muir DW, et al: The relationship
between perinatal hypoxia and newborn encephalopathy. Am J Obstet Gynecol 152:256-260, 1985
Robertson CMT: Long-term follow up of term neonates
with perinatal asphyxia, in Stevenson DK, Sunshine P,
(eds): Fetal and Neonatal Brain Injury (ed 3) Oxford,
Oxford University Press, 2003, 829-858
Shankaran S, Woldt E, Koepke T, et al: Acute neonatal
morbidity and long-term central nervous system sequelae of perinatal asphyxis in term infants. Early Human Dev 25:135-148, 1991
Ellenberg JH, Nelson KB: Cluster of perinatal events
identifying infants at high risk for death or disability.
J Pediatr 113:546-552, 1988
Nelson KB, Leviton A: How much of neonatal encephalopathy is due to birth asphyxia? Am J Dis Child 145:
1325-1331, 1991
Enns GM: Inborn errors of metabolism with features of
hypoxic-ischemic encephalopathy, in Stevenson DK,
Sunshine P, (eds): Fetal and Neonatal Brain Injury (ed
3). Oxford, Oxford University Press, 2003, pp 392-408
Carter BS, McNabb F, Merenstein GB: Prospective validation of a scoring system for predicting neonatal morbidity after acute perinatal asphyxia. J Pediatr 132:619623, 1998
Perlman JM, Risser MS: Can asphyxiated infants at risk
for neonatal seizures be rapidly identified by current
high-risk markers? Pediatrics 97:456-462, 1998
Wayenberg JL, Dramaix M, Vermeylen D, et al: Neonatal
outcome after birth asphyxia: early indicators of prognosis. Prenat Neonat Med 3:482-489, 1998
Ekert P, Perlman M, Steinlin M, et al: Predicting the
outcome of post asphyxial hypoxic-ischemic encephalopathy within 4 hours of birth. J Pediatr 131:613-617,
1997
Holmes G, Rowe J, Hafford J, et al: Prognostic value of
the electroencephalogram in neonatal asphyxia. Electroencephalogr Clin Neurophysiol 53:60-72, 1982
Watanabe K, Miyazaki S, Hara K, et al: Behavioral state
cycles, background EEGs and prognosis of newborns
with perinatal hypoxia. Electroencephalogr Clin Neurophysiol 49:618-625, 1980
Allemand F, Caravalle B, Tozzi C, et al: Prognostic value
of the cerebral function monitor (cfm) and of the EEG
in term newborns with hypoxic-ischemic encephalopathy. Italian J Pediatr 22:61-66, 1996
Toet MC, van der Meij W, de Vries LS, et al: Comparison
between simultaneously recorded amplitude integrated
EEG cerebral function monitor (CFM) and standard
EEG in neonates. Pediatrics 109:771-779, 2002
Toet MC, Hellström-Westas L, Groenendaal F, et al:
Amplitude integrated EEG 3 and 6 hours after birth in
Neuroprotection in Asphyxiated Term Infants
44.
45.
46.
47.
48.
49.
50.
51.
52.
53.
54.
55.
56.
57.
58.
59.
60.
full term neonates with hypoxic-ischaemic encephalopathy. Arch Dis Child Fetal Neonatal Ed 80:F0-F5, 1999
al Naqeeb N, Edwards AD, Cowan FM, et al: Assessment
of neonatal encephalopathy by amplitude-integrated
electroencephalography. Pediatrics 103:1263-127, 1999
Hellström-Westas L, Rosen I, Svenningsen NW: Predictive value of early continuous amplitude integrated EEG
recordings on outcome after severe birth asphyxia in full
term infants. Arch Dis Child 72:F34-F38, 1995
Groenendaal F, de Vries LS: Selection of babies for
intervention after birth asphyxia. Sem Neonatol 5:17-32,
2000
Hellström-Westas L, de Vries LS, Rosen I: Hypoxia-ischemia and aEEG, in Hellström-Westas L, de Vries LS,
Rosen I (eds): An Atlas of Amplitude Integrated EEG in
the Newborn New York, NY, NY Parthenon Publishing,
2003, pp 67-94
Shalak LF, Laptook AR, Velaphi SC, et al: Amplitudeintegrated electroencephalography coupled with an
early neurologic examination enhances prediction of
term infants at risk for persistent encephalopathy. Pediatrics 111:351-357, 2003
Martı́n-Ancel A, Garcia-Alix A, Pascual-Salcedo D, et al:
Interleukin-6 in the cerebrospinal fluid after perinatal
asphyxia is related to early and late neurological manifestations. Pediatrics 100:789-794, 1997
Sävman K, Blennow M, Gustafson K, et al: Cytokine
response in cerebrospinal fluid after birth asphyxia. Pediatr Res 43:746-751, 1998
Oygür N, Sönmez O, Saka O, et al: Predictive value of
plasma and cerebrospinal fluid tumour necrosis factor-␣
and interleukin-IB concentrations on outcome of full
term infants with hypoxic-ischaemic encephalopathy.
Arch Dis Child Fetal Neonatal Ed 79:F190-F193, 1998
Huang CC, Wang ST, Chang YC, et al: Measurement of
the urinary lactate: creatinine ratio for the early identification of newborn infants at risk for hypoxic-ischemic
encephalopathy. N Engl J Med 341:328-335, 1999
Nelson KB, Grether KJ: Selection of neonates for neuroprotective therapies. Arch Pediatr Adolesc Med 153:
393-398, 1999
Grether JK, Nelson KB: Maternal infection and cerebral
palsy in infants of normal birth weight. JAMA 278:207211, 1997
Thorarensen O, Ryan S, Hunter J, et al: Factor V Leiden
mutation: An unrecognized cause of hemiplegic cerebral palsy, neonatal stroke, and placental thrombosis.
Ann Neurol 42:372-375, 1997
Debus O, Koch HG, Kurlemann G, et al: Factor V Leiden
and genetic defects of thrombophilia in childhood
porencephaly. Arch Dis Child Fetal Neonatal Ed 78:
F121-F124, 1998
Silver RK, MacGregor SN, Pasternak JF, et al: Fetal stroke
associated with elevated maternal anticardiolipin antibodies. Obstet Gynecol 80:497-499, 1992
Paneth N: Birth and the origins of cerebral palsy. N Engl
J Med 315:124-126, 1986
Jones MD, Traystman RJ, Simmons MA, et al: Effects of
changes in arterial O2 content on cerebral blood flow in
the lamb. Am J Physiol 240:H209-215, 1981
Gunther G, Junker R, Strater R, et al: for the Childhood
Stoke Study Group: Symptomatic ischemic stroke in full-
61.
62.
63.
64.
65.
66.
67.
68.
69.
70.
71.
72.
73.
74.
75.
76.
77.
331
term neonates: Role of acquired and genetic prothrombotic risk factors. Stroke 31:2437-2441, 2000
Nelson KB, Dambrosia JM, Grether JK, et al: Neonatal
cytokines and coagulation factors in children with cerebral palsy. Ann Neurol 44:665-675, 1999
Shalak LF, Laptook AR, Jafri HS, et al: Clinical chorioamnionitis, elevated cytokines, and brain injury in term
infants. Pediatrics 110:673-680, 2002
Lorek A, Takei Y, Cady EB, et al: Delayed (“secondary”)
cerebral energy failure after acute hypoxia-ischemia in
the newborn piglet: continuous 48 hour studies by phosphorous magnetic resonance spectroscopy. Pediatr Res
36:699-706, 1994
Johnston MV: Excitotoxicity in neonatal hypoxia. Ment
Retard Dev Disabil Res Rev 7:229-234, 2001
Palmer C, Roberts RL, Bero C: Deferoxamine post-treatment reduces ischemic brain injury in neonatal rats.
Stroke 25:1039-1045, 1994
Liu XH, Kwon D, Schielke GP, et al: Mice deficient in
interleukin-1 converting enzyme are resistant to neonatal hypoxic-ischemic brain damage. J Cereb Blood Flow
Metab 19:1099-1108, 1999
Cheng Y, Deshmukh D, D’Costa A, et al: Caspase inhibitor affords neuroprotection with delayed administration in a rat model of neonatal hypoxic-ischemic brain
injury. J Clin Invest 101:1992-1999, 1998
Bergstedt K, Hu BR, Wieloch T: Post-ischemic changes
in protein synthesis in the rat brain: Effects of hypothermia. Exp Brain Res 95:91-99, 1993
McDonald JW, Silverstein FS, Johnston MV: MK-801 protects the neonatal brain from hypoxic-ischemic damage.
Eur J Pharmacol 140:359-361, 1987
Martin D, Chinookoswong N, Miller G: The interleukin-1 receptor antagonist (rhIL-1ra) protects against cerebral infarction in a rat model of hypoxia-ischemia. Exp
Neurology 130:362-367, 1994
Laptook AR, Corbett RJT, Sterett R, et al: Quantitative
relationship between brain temperature and energy utilization rate measured in vivo using 31P and 1H magnetic
resonance spectroscopy. Pediatr Res 38:919-925, 1995
Thoresen M, Satas S, Puka-Sundvall M, et al: Post-hypoxic hypothermia reduces cerebrocortical release of
NO and excitotoxins. NeuroReport 8:3359-3362, 1997
Edwards AD, Yue X, Squier MV, et al: Specific inhibition
of apoptosis after cerebral hypoxia-ischemia by moderate post-insult hypothermia. Biochem Biophys Res
Comm 217:1193-1199, 1995
Fukuda H, Tomimatsu T, Watanabe N, et al: Post-ischemic hypothermia blocks caspase-3 activation in the newborn rat brain after hypoxia-ischemia. Brain Res 910:
187-191, 2001
Globus MYT, Busto R, Lin B, et al: Detection of free
radical activity during transient global ischemia and recirculation: Effects of intraischemic brain temperature
modulation. J Neurochem 65:1250-1256, 1995
Goss JR, Styren SD, Miller PD, et al: Hypothermia attenuates the normal increase in interleukin 1 RNA and
nerve growth factor following traumatic brain injury in
the rat. J Neurotrauma 12:159-167, 1995
Thoresen M, Penrice J, Lorek A, Cady EB, Wylezinska M,
Kirkbride V, Cooper CE, Brown AD, Edwards AD, Wyatt
JS, Reynolds EOR: Mild hypothermia after severe tran-
332
78.
79.
80.
81.
82.
83.
84.
85.
Shankaran and Laptook
sient hypoxia-ischemia ameliorates delayed cerebral energy failure in the newborn piglet. Pediatr Res 37:667670, 1995
Pardridge WM: Drug delivery to the brain. J Cereb Blood
Flow Metab 17:713-731, 1997
Shankaran S, Laptook A, Wright L, et al: Whole-body
hypothermia for neonatal encephalopathy: Animal observations as a basis for a randomized, controlled pilot
study in term infants. Pediatrics 110:377-385, 2002
Tan WKM, Matthew CE, During MJ, et al: Accumulation
of cytotoxins during the development of seizures and
edema after hypoxic-ischemic injury in late gestation
fetal sheep. Pediatr Res 39:791-797, 1996
Laptook AR, Corbett RT, Sterett R, et al: Modest hypothermia provides partial neuroprotection for ischemic
neonatal brain. Pediatr Res 35:436-442, 1994
Shankaran S, Kottamasu SR, Kuhns L: Brain sonography, computed tomography, and single-photon emission
computed tomography in term neonates with perinatal
asphyxia. Clin Perinatol 20:379-394, 1993
Blankenberg FG, Norbash AM, Lane B, et al: Neonatal
intracranial ischemia and hemorrhage: Diagnosis with
US, CT, and MR Imaging. Radiology 199:253-259, 1996
Biagioni E, Mercuri E, Rutherford M, et al: Combined
use of electroencephalogram and magnetic resonance
imaging in full-term neonates with acute encephalopathy. Pediatrics 107:461-468, 2001
Rutherford MA, Pennock JM, Counsell SJ, et al: Abnormal magnetic resonance signal in the internal capsule
predicts poor neurodevelopmental outcome in infants
86.
87.
88.
89.
90.
91.
92.
with hypoxic-ischemic encephalopathy. Pediatrics 102:
323-328, 1998
Soul JS, Robertson RL, Tzika AA, et al: Time course of
changes in diffusion-weighted magnetic resonance imaging in a case of neonatal encephalopathy with defined
onset and duration of hypoxic-ischemic insult. Pediatrics
108:1211-114, 2001
Krägeloh-Mann I, Helber A, Mader I, et al: Bilateral
lesions of thalamus and basal ganglia: origin and outcome. Dev Med Child Neurol 44:477-484, 2002
Miller SP, Newton N, Ferriero DM, et al: Predictors of
30-month outcome after perinatal depression: Role of
proton MRS and socioeconomic factors. Pediatr Res 52:
71-77, 2002
Thorngren-Jerneck K, Ohlsson T, Sandell A, et al: Cerebral glucose metabolism measured by positron emission
tomography in term newborn infants with hypoxic-ischemic encephalopathy. Pediatr Res 49:495-501, 2001
Palisano R, Rosenbaum P, Walter S, et al: Development
and reliability of a system to classify gross motor function
in children with cerebral palsy. Dev Med Child Neurol
39:214-223, 1998
Cordes I, Roland EH, Lupton BA, et al: Early prediction
of the development of microcephaly after hypoxic-ischemic encephalopathy in the full-term newborn. Pediatrics 93:703-707, 1994
Beckung E, Hagberg G: Correlation between ICIDH
handicap code and gross motor function classification
system in children with cerebral palsy. Dev Med Child
Neurol 42:669-673, 2000