Medical Information form

Medical Information form
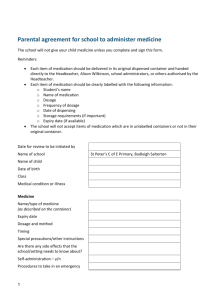
Please provide the following information to facilitate administration of medication(s) while your child is traveling to Canada. Please be thorough in your explanations and return the form at the
Parent Information Meeting on Thursday, March 27, 2008.
Student Name_____________________________________________________________
Parent name(s) ____________________________________________________________
Parent phone # (day) _______________________ (evening) _________________________
(cell)________________________ (other)
1) Medication name____________________________________________________
Time(s) of day taken_________________________________________________
Dosage___________________________________________________________
Any known side effects? Comments? Special needs?
2) Medication name____________________________________________________
Time(s) of day taken_________________________________________________
Dosage___________________________________________________________
Any known side effects? Comments? Special needs?
3) Medication name____________________________________________________
Time(s) of day taken_________________________________________________
Dosage___________________________________________________________
Any known side effects? Comments? Special needs?
4) Medication name____________________________________________________
Time(s) of day taken_________________________________________________
Dosage___________________________________________________________
Any known side effects? Comments? Special needs?
*** You may list additional medications on the reverse side, if necessary.
As a reminder, chaperones must receive all prescription medications before boarding the bus.
Please place each medication in a separate, clear plastic zip lock storage bag. Label each bag with your child’s name.