THE EVOLVING IMPACT OF G PROTEIN-COUPLED RECEPTOR KINASES IN CARDIAC HEALTH
advertisement

Physiol Rev 95: 377– 404, 2015 doi:10.1152/physrev.00015.2014 THE EVOLVING IMPACT OF G PROTEIN-COUPLED RECEPTOR KINASES IN CARDIAC HEALTH AND DISEASE Priscila Y. Sato, J. Kurt Chuprun, Mathew Schwartz, and Walter J. Koch Center for Translational Medicine and Department of Pharmacology, Temple University School of Medicine, Philadelphia, Pennsylvania; and Advanced Institutes of Convergence Technology, Suwon, South Korea Sato PY, Chuprun JK, Schwartz M, Koch WJ. The Evolving Impact of G ProteinCoupled Receptor Kinases in Cardiac Health and Disease. Physiol Rev 95: 377– 404, 2015; doi:10.1152/physrev.00015.2014.—G protein-coupled receptors (GPCRs) are important regulators of various cellular functions via activation of intracellular signaling events. Active GPCR signaling is shut down by GPCR kinases (GRKs) and subsequent -arrestin-mediated mechanisms including phosphorylation, internalization, and either receptor degradation or resensitization. The seven-member GRK family varies in their structural composition, cellular localization, function, and mechanism of action (see sect. II). Here, we focus our attention on GRKs in particular canonical and novel roles of the GRKs found in the cardiovascular system (see sects. III and IV). Paramount to overall cardiac function is GPCR-mediated signaling provided by the adrenergic system. Overstimulation of the adrenergic system has been highly implicated in various etiologies of cardiovascular disease including hypertension and heart failure. GRKs acting downstream of heightened adrenergic signaling appear to be key players in cardiac homeostasis and disease progression, and herein we review the current data on GRKs related to cardiac disease and discuss their potential in the development of novel therapeutic strategies in cardiac diseases including heart failure. L I. II. III. IV. V. VI. INTRODUCTION G PROTEIN-COUPLED RECEPTOR... G PROTEIN-COUPLED RECEPTOR... G PROTEIN-COUPLED RECEPTOR... OTHER GRKs AND THE... CONCLUSIONS 377 379 387 391 394 396 I. INTRODUCTION The body maintains its “physiological homeostasis” by constantly sending signals to organs, which receive and translate circulating stimuli into appropriate cellular responses. The ability of cells to communicate with each other is paramount for the maintenance of this homeostasis. This communication is achieved through molecules, also known as agonists, which bind to receptors activating downstream signal transduction pathways. One of the major agonist-receptor interactions is that of G protein-coupled receptors (GPCRs) (155). Although there is not a solid consensus on classification, this superfamily of receptors may be considered to encompass protein members from six different classes: class A (rhodopsin-like), class B (secretin-receptor like), class C (metabotropic-glutamate/pheromone), class D (fungal mating pheromone), class E (cAMP), and frizzled-smoothened (8, 38, 77, 78, 130). Although the exact size of this superfamily is un- known, human genome sequence analysis has predicted that nearly 800 human genes are GPCRs (25). Commonly known GPCRs include: -adrenergic receptors (-ARs), ␣-adrenergic receptors (␣-ARs), rhodopsin, endothelin receptors, adenosine receptors, and others (77). These receptors are integral membrane proteins characterized by seven membrane-spanning domains, which upon agonist binding change their conformation triggering heterotrimeric G proteins to bind to it in the intracellular space and subsequently activating downstream signal transduction pathways (45, 205, 206, 214) (see FIGURE 1). Agonist binding to GPCRs promote conformational changes (206) which allow for the dissociation of heterotrimeric G proteins into ␣ and ␥ subunits, stimulating activation of downstream proteins such as protein kinase A, Src, MEK5, phosphatidylinositol 3-kinase (PI3K), GPCR kinase (GRK), etc. While activation of signaling pathways by these receptors is extremely important, so is deactivation. When the balance of activation and deactivation is impaired, imperative cellular mechanisms become faulty, and if not corrected in a timely manner, this signaling can become irreversibly detrimental to the body, leading to diseased states. Deactivation of GPCR-elicited signaling is mainly accomplished by GRKs, and this is termed desensitization. Termination of signaling via GPCRs is done through a two-step mechanism: first, the GRK phosphorylates the active receptor (and only this form of the receptor), leading to confor- 0031-9333/15 Copyright © 2015 the American Physiological Society 377 SATO ET AL. Resting (GDP-bound) state G-protein coupled receptor Agonist-binding and Gα-Gβγ association GDP Gα Gβγ Agonist Receptor recycling GDP Gα RGS P P P P Receptor endocytosis GDP Gα Gβγ Gβγ P RGS binding and GTP hydrolysis Nucleotide exchange GRK Proteosomal degradation Effector Effector GTP Gα GRK β-arrestin P P P Gβγ Gα-Gβγ dissociation, GRK2 and β-arrestin association GTP GTP P GTP Gα Gβγ GDP GT Signaling FIGURE 1. G protein-coupled receptor activation and reactivation. At rest, G␣␥ is bound to GDP and both receptor and G␣␥ are not associated. Upon agonist binding, G␣␥ associates with the receptor followed by GDP-GTP nucleotide exchange. G␣ and G␥ dissociate from the receptor with its respective effector proteins leading to downstream signaling. At the active receptor, GRKs bind and phosphorylate the receptor leading to receptor conformational changes and subsequent -arrestin binding. -Arrestin-bound receptors are then primed for clathrin-mediated endocytosis and sorted for proteosomal degradation or receptor recycling. Concurrently, RGS binds to G␣ leading to GTP hydrolysis and promoting the receptor to its initial resting state. mational changes that promote binding of -arrestin; and second, phosphorylated and -arrestin bound GPCRs are no longer able to bind to and activate G proteins (132, 228, 274). FIGURE 1 depicts a schematic of GPCR activation, signaling, and desensitization. Briefly, agonist binding to the receptor causes nucleotide exchange, G␣-G␥ dissociation, and downstream signaling through effector activation. The G␣-G␥ dissociation mobilizes GRKs to phosphorylate the activated receptor, a process which may vary depending on the GRK isoforms (see sect. IIC). Serine (Ser) and threonine (Thr) phosphorylation by GRKs at the COOH terminus of the receptor promotes -arrestin mobilization and binding to the receptor. This may further lead to clathrin-induced endocytosis and reactivation or degradation of the receptor. Although receptor endocytosis reactivation/recycling is an extremely important and complex mechanism involving many other proteins, it is beyond the scope of this review and better detailed by Moore et al. (163). Lastly, activation of GTPases causes G protein trimer reformation and repriming of the receptor for another round of stimulation. In this review, we focus on the mul- 378 tifaceted functions of GRKs including their evolving nonGPCR or noncanonical activity that appears to be critical for cardiovascular homeostasis and disease. The first description of phosphorylation-mediated deactivation of GPCRs was provided in the 1970s where the photoreceptor rhodopsin, a prototypical GPCR, was rapidly deactivated by phosphorylation by “opsin or rhodopsin kinase” (also known as GRK1) (28, 133, 270). Later, the same deactivation mechanism was proposed in many other GPCRs (reviewed in Ref. 35) including 2ARs (21). Several studies have demonstrated that agonist-specific desensitization of the 2-AR was associated with receptor phosphorylation (19, 229, 243). GRK2 was then identified (initially named the -AR kinase, -ARK1) and shown to be able to phosphorylate -ARs as well as rhodopsin in a light-dependent manner (19, 21). It was only when GRK2 was identified and characterized to possess properties similar to GRK1 that the hypothesis was put forth of a possible family of new proteins: the GRK family (16, 19). Physiol Rev • VOL 95 • APRIL 2015 • www.prv.org G PROTEIN-COUPLED RECEPTOR KINASES II. G PROTEIN-COUPLED RECEPTOR KINASES Visual subfamily 1 A. GRK Family Members The GRK family is composed of seven members. This family of kinases is quite small considering that they are responsible for deactivating potentially more than 800 GPCR gene products as only a small percent of these receptors are not regulated by phosphorylation (78). Although identification of phosphorylation-induced desensitization of GPCRs by rhodopsin kinase (GRK1) (270) and GRK2 (or -ARK1) (18, 21) opened the doors to this novel deactivation mechanism, it was only after cloning of GRK2 in 1989 that the idea of a new eukaryotic serine/threonine (Ser/Thr) protein kinase family fully emerged. Promptly thereafter, new members of this family were identified and included: GRK3 (20), GRK4 (6), GRK5 (134, 192), GRK6 (17), and GRK7 (101, 269). Based on sequence similarity and gene structure analysis, vertebrate GRKs are further divided into three subcategories: visual or rhodopsin-kinases subfamily (comprising of GRK1 and GRK7), -AR kinases subfamily (comprising of GRK2 and GRK3), and the GRK4 subfamily (comprising of GRK4, GRK5, and GRK6) (see FIGURE 2). The GRK family of proteins possesses shared structural and functional hallmarks. These proteins are mainly composed of three regions: a short 25-residue proximal NH2-terminal region unique to the GRK family of kinases, a regulator of G protein signaling (RGS) homology domain (RH), which is interrupted by a Ser/Thr kinase domain (KD). This ⬃500 –520 amino acid residue KD belongs to the AGC kinase family and is shared by all GRKs (reviewed in Refs. 95, 112). The entire NH2 terminus is highly conserved among GRKs though the NH2-terminal region is unique to the GRK family of kinases and implicated in GPCR binding (reviewed in Refs. 95, 112). The COOH terminus is the most diverse region among GRK subfamilies. GRK1 and GRK7 have short COOH-terminal prenylation sequences (101, 113). GRK2 and GRK3 contain pleckstrin homology (PH) domains implicated in binding anionic phospholipids and G␥ subunits (34, 60, 128, 187). GRK2 has been recently implicated to localize to mitochondria (43, 83). GRK2 does not have a classical mitochondrial localization sequence, so it is not clear what is the required minimal sequence necessary for this novel localization. GRK4 and GRK6 have palmitoylation sites (194, 241) as well as lipidbinding capabilities (118). GRK5 membrane targeting relies on a phospholipid binding domain (residues 552–562) (196). Alternative splicing has been identified for GRK4 (4 splice variants) (194, 216) and GRK6 (4 splice variants) (75, 161, 193, 257); however, not all splice variants appear to be expressed across species. More recently, a nuclear localization sequence (NLS) has been identified within GRK5 (amino acids 388 –395) (120), which happens to be a common feature in all GRK4 subfamily members (119). In addition, a nuclear export signal (NES, amino acids 259 –265) has also been identified 42 184 514 532 563 K219 GRK1 1 40 531 513 553 185 K220 GRK7 βARK subfamily 1 36 184 513 553 661 689 513 553 661 688 K220 GRK2 1 36 184 K220 GRK3 GRK4 subfamily 1 38 181 508 525 578 K216K217 GRK4 1 38 180 259 265 388 395 507 525 590 K215 GRK5 1 38 180 507 525 576 K215K216 GRK6 N-terminal region PH domain RH domain Nuclear localization signal C-terminus Nuclear export signal Kinase domain FIGURE 2. GRK topology and subfamily distribution. All GRKs are comprised of a NH2-terminal region (green), followed by an RH domain (pink) interrupted by a kinase domain (yellow) and a COOH terminus (orange). Visual or rhodopsin-kinases subfamily comprises of GRK1 (also known as rhodopsin kinase) and GRK7, with the unique capability of prenylation in the COOH terminus. The ARK subfamily comprises of GRK2 and GRK3, having a characteristic PH domain. The GRK4 subfamily is comprised of GRK4, GRK5, and GRK6. GRK5 has a unique nuclear localization signal (in blue) and nuclear export signal (in dark green). Numbers in black correspond to amino acids at start or end of each region. GRK4 and GRK6 residue numbers correspond to GRK4␣ and GRK6A variants, respectively. Numbers in red correspond to residues responsible for catalytic activity. (119). FIGURE 2 depicts the tri-domain schematic of all members of the GRK family that include the above-described features. Catalytic activity is dependent on specific lysine residues and shown for each isoform. B. GRK Tissue Localization Most GRKs are ubiquitously expressed; however, there is selective tissue distribution. GRK1 and GRK7, members of Physiol Rev • VOL 95 • APRIL 2015 • www.prv.org 379 SATO ET AL. the rhodopsin-kinase subfamily, are generally restricted to the retina where they primarily target rhodopsin and cone opsin, respectively. Within the retina, these two isoforms are particularly restricted to rod and cone photoreceptors, although both are also present in pinealocytes (41, 231, 283, 284). GRK4 is highly expressed in the testes (194), although it has also been shown to be expressed in proximal tubule cells in kidneys (73, 258), in the brain (217), and in the uterus myometrium (29). In particular, two GRK4 variants (GRK4␣ and GRK4␥) have been reported to signal through D1 and D3 dopamine receptors within the kidney (73, 258). Essentially all the remaining isoforms are ubiquitously expressed with varying degrees of expression depending on type of tissue. GRK2 primarily targets several GPCRs including -ARs and angiotensin II type 1 receptors, and it is expressed in most tissues. GRK3 targets olfactory receptors, thrombin receptors, kappa-opioid CRF1 (57, 219), and ␣1- and ␣2–ARs (12, 246). It is found in most tissues, but most prominently in the olfactory epithelium. GRK5 can phosphorylate -ARs, adenosine receptors, and M2 muscarinic receptors, and it is expressed in most tissues (14). TABLE 1 shows tissue distribution of various GRK isoforms (reviewed in Ref. 112). Pertinent to this review is the expression of cardiac GRKs. In the human heart there is evidence for expression of GRK2, GRK3, GRK5, and GRK6 (67). The most prominent cardiac GRK isoforms are 2 and 5, although 3 and 6 have also been reported at low levels (1, 67, 162). Moreover, it is important to note that a particular GRK does not have to be the most prominently expressed GRK in a tissue to be crucial for a specific GPCR signaling regulation as its cellular localization and activity are key measures determining GPCR-GRK interactions. More recently, GRK3 and GRK4 have been described to be present in the thyroid nodules and to be upregulated in hyperfunc- Table 1. GRK isoform tissue distribution GRK Tissue Localization Reference Nos. 1 2 Retina⬎⬎pineal Leukocytes⬎front cortex of brain⬎⬎heart⬎lung⬎kidney, thyroid nodules Brain⬎spleen⬎heart, lung, kidney, thyroid nodules Testis⬎⬎⬎⬎brain, thyroid nodules Heart, placenta, lung⬎skeletal muscle⬎brain, liver, pancreas⬎kidney, thyroid nodules Brain, skeletal muscle⬎pancreas⬎heart, lung, kidney, placenta⬎liver, thyroid nodules Retina, particularly cones 146, 171 16, 65, 135, 262 3 4 5 6 7 380 20, 58, 135, 209, 262 6, 262 134, 262 17, 98, 262 101, 269 tioning thyroids, which may also indirectly impact cardiac function (262). C. Canonical Subcellular Targeting of GRK Isoforms Agonist-mediated activation of GPCRs is obviously critical for cellular responses; however, sustained GPCR stimulation is deleterious in part because of receptor desensitization and eventually downregulation. If novo or de novo activation of receptors does not occur, this downregulation of receptors may not only lead to loss of responsiveness to agonists but also cellular response disarray. It is the primary job of GRKs to reverse the harmful effects of chronic GPCR stimulation. To accomplish this goal, GRKs are canonically thought to be present mainly in the cellular cytoplasm or close to the plasma membrane. Certain GRK isoforms have specific sequence trademarks that allow them to preferentially target specific subcellular compartments. In general, membrane targeting of all GRKs towards activated GPCRs involves residues and domains within the COOH terminus of these kinases (see TABLE 2). GRK1 and GRK7 are localized directly to the plasma membrane after GPCR activation as both isoforms possess a short COOH-terminal prenylation sequence (101, 113), and the attached lipid molecules act as lipid anchors facilitating attachment to cell membranes. This cellular localization is advantageous for visual GRKs as they perform their function of “probing” for active rhodopsins or cone opsins. As such, visual GRKs perform a two-dimensional search instead of a three-dimensional diffusion, which is essential for their ultra-rapid signal termination. This means that because GRK1 and GRK7 attachment to the membrane is facilitated by lipid anchoring, when GPCRs become active, these specific kinases have the advantage of searching for active receptors in the x- and y-position only since they are already closely associated with the membrane. On the contrary, all other GRKs do not have this facilitated mode of attachment, having to perform an x, y, and z search for activated receptors. The -ARK family of kinases (GRK2 and GRK3) are membrane targeted from the cytosol through binding to the membrane-anchored G␥ subunits of G proteins following their dissociation after GPCR activation (34, 187). Indeed, GRK2 and GRK3 were originally found to be localized in the cytoplasm and then recruited to the membrane as a response to agonist-occupied receptors (19, 21, 242). This binding occurs within the COOH terminus and includes the PH domain (34, 189). Because G␥ subunits are generated by activated receptors, free G␥ recruits these GRK isoforms to the locale of active GPCRs, thereby greatly enhancing GPCR phosphorylation only when needed ensuring the fidelity of the desensitization process of only agonistoccupied receptors. Nevertheless, it is important to note Physiol Rev • VOL 95 • APRIL 2015 • www.prv.org G PROTEIN-COUPLED RECEPTOR KINASES Table 2. GRK subcellular targeting at baseline conditions GRK Tissue Localization Reference Nos. 1 2 Cytoplasm very close to plasma membrane (rod outer segments) Cytoplasm (free or associated with actin, actinin, microtubules)⬎plasma membrane ⬎⬎⬎mitochondria Cytoplasm⬎plasma membrane Splice variants below: ␣: Cytoplasm⬎ plasma membrane ⬎⬎⬎nucleus : Cytoplasm⬎ plasma membrane ⬎⬎⬎nucleus ␥: Cytoplasm⬎ plasma membrane ⬎⬎⬎nucleus ␦: Cytoplasm ⬎ plasma membrane ⬎⬎⬎nucleus Cytoplasm ⬎⬎⬎nucleus Mainly in the cytoplasm, splice variants below: A: Cytoplasm and close to plasma membrane⬎⬎⬎nucleus B: Cytoplasm and close to plasma membrane⬎⬎⬎nucleus C: Cytoplasm and close to plasma membrane⬎⬎⬎nucleus D: Exclusively in the nucleus Cytoplasm very close to plasma membrane (cone outer segments) 39, 224 19, 21, 43, 83, 168, 242, 281 3 4 5 6 7 that the fidelity of the desensitization process is aided by the preference of GRKs for the agonist-occupied conformation of the receptor as a substrate, as agonist occupancy can increase GPCR substrate affinity manyfold. Thus, like GRK1 and GRK7, the -ARK kinases attach to the membrane via a prenyl group; however, these kinases “pirate” the lipid anchors from G␥ and do not have them directly attached to their C-tail. The G␥ binding domain within the COOH-terminal PH domain of GRK2 (FIGURE 2) was originally determined biochemically (128). Following the structural information of GRK2 at the atomic level, the key residues for G␥ binding were confirmed (143). Importantly, peptides from this region can block the membrane localization of GRK2 and prevent -AR and GPCR desensitization (128). The shortest effective GRK2-G␥ blocking peptide is a 28-mer peptide. However, most studies over the last 20 years have used the 194-amino acid residue peptide of the entire COOH terminus of GRK2, -ARKct (128, 129), which has been shown to be effective both in vitro and in vivo at inhibiting GRK2 activity (discussed in detail below). Lastly, subcellular targeting of the GRK4 subfamily involves protein hallmarks and modifications also present in the COOH termini. GRK4 and GRK6 carry both palmitoylation sites as well as lipid-binding positively charged elements which promote a biased membrane localization (147, 194, 240, 241). Though lacking the palmitoylation site, the COOH terminus of GRK5 is capable of binding phospholipids, thus distinctly promoting plasma membrane targeting (251). These features likely enhance lipid bilayer affinity and kinase activity. Interestingly, GRK6A splice variant contains elements that both promote and inhibit membrane localization. While it contains the features men- 19, 21, 242, 281 119 119 119 119 119, 281 119, 119, 119, 119, 41 120, 281 257 257 257 257 tioned above, it also contains acidic residues that inhibit membrane localization (118, 257). A nonpalmitoylated form of GRK6A is detected in the cytoplasm and nucleus, although nuclear function still remains unclear (118). Surprisingly, GRK6B and GRK6C, which do not contain the palmitoylation sites, are still capable of localizing to the plasma membrane in cultured cells (257). Interestingly, membrane localization is rescued when the string of acidic residues located in the COOH terminus of GRK6A is mutated to neutral or basic residues in nonpalmitoylated GRK6A. This suggests that palmitoylation is not the dominant mechanism in which GRK4 subfamily of proteins achieve their preferential membrane localization. In addition, a fourth isoform for GRK6 (GRK6D) has been proposed to lack the catalytic domain and exclusively localize to the nucleus, although its function is yet to be determined (257). In vitro, different GRK isoforms may phosphorylate different GPCRs, and differential subcellular targeting and tissue expression levels might contribute to explaining the functional specificity observed in vivo (see TABLE 1). For instance, GRK2 is capable of phosphorylating rhodopsin in a light-dependent manner (18), yet GRK1 is the isoform involved in rhodopsin deactivation in vivo as GRK2 does not perform this function in GRK1 knockout mice (39). GRK2 and GRK3 are both expressed in the brain and HEK cells. In HEK cells, both isoforms behave similarly, yet in the brain, GRK3 is more membrane-associated that GRK2 (4, 33). Although enormous effort has been expended to understand GRK receptor specificity, the mechanism for receptor preference still remains unclear. Receptor phosphorylation “bar coding” has been suggested as one of the ways specificity might be determined (166), yet this concept may not entirely account for GRK selectivity. In this study, phos- Physiol Rev • VOL 95 • APRIL 2015 • www.prv.org 381 SATO ET AL. phorylation patterns of the receptor by GRKs lead to diverse -arrestin-related activities. Yet, it did not explain why a specific GRK was more prone to phosphorylate a receptor over another. GRK receptor specificity has been analyzed in hybrid transgenic mouse hearts. For example, GRK2, GRK3, and GRK5 overexpressing mice were bred with cardiac-specific transgenic mice overexpressing constitutively activated ␣1B-ARs. The results revealed that different GRKs had varying effects on this receptor. While GRK3 desensitized ␣1B-ARs very well, GRK2 had no effect, and the effects of GRK5 were mixed (68). In another study using just GRK2 and GRK5 cardiac overexpressing transgenic mice, it was found that both of these cardiac GRKs desensitize -ARs quite well, while GRK2 could also attenuate signaling through angiotensin II receptors, and GRK5 had no effect on these receptors (212). GRK5 and GRK2 also differently effected cardiac adenosine responses, respectively desensitizing or having no effect (212). Clearly, GRKs have receptor selectivity in vivo; however, the mechanism of receptor preference still remains unknown. Different expression levels of various GRK isoforms in a cell-specific manner may be one of the ways in which GRKs accomplish different tasks in various tissues, emphasizing the importance of spatial-temporal expression. Nevertheless, relative levels of expression in a particular tissue do not necessarily explain receptor-kinase specificity. Yet, how bar coding, cell-specific expression, or structural characteristics play a role in receptor specificity still requires further investigation. D. Mechanism of Action of GRKs The molecular basis in which GRKs first recognize active receptors still remains a matter of speculation. The most plausible hypothesis is termed “fly casting,” in which the disordered NH2 terminus of GRKs forms an initial lowaffinity interaction with the active receptor (55, 226). In the case of GRK1 and GRK7 which have a prenylation sequence thought to involve lipid anchoring to membranes, this would mean that the search is in two dimensions, increasing its chance of finding active-receptors and fulfilling its ultra-fast response requirement. The other subfamilies are thought to involve a three-dimensional search, although proximity to the membranes would also permit for these kinases to be readily available to deactivate the receptor in a timely manner. Crystal structures of specific GRKs have proven essential in understanding possible mechanisms of action and activation processes. These concepts have been well summarized and recently reviewed in References 95 and 104. The bestdescribed function of GRKs is the ability to phosphorylate active GPCRs. With the exception of GRK4␣, which has been shown to be constitutively active and capable of phosphorylating unstimulated GPCRs (160, 203), the activity of 382 GRKs appear to depend on the functional state of the target. In fact, docking to the active-receptor seems to directly activate GRKs (42, 172). Phosphorylation of the active receptor can in itself decrease G protein coupling (274), but most importantly, it allows for -arrestin to bind and block the cytoplasmic surface of receptors, thus preventing interaction with effector enzymes that are necessary to initiate downstream signaling (132). A recent structure of GRK6 in a “closed conformation” revealed an ordered NH2 terminus engaged in extensive interactions with both the small lobe and the C-tail of the kinase domain (26). These interactions are physically impossible when GRK6 is in a more open conformation (144). More interesting is the fact that the contact points of these residues in the NH2 terminus and the kinase domain are highly conserved in all GRKs and that site-directed mutagenesis revealed them to be essential for phosphorylation of active GPCRs and soluble substrates (26, 103, 105, 174, 238). In particular, mutations in hydrophobic residues in the NH2-terminal helix of the kinase abolished receptor but not peptide phosphorylation, suggesting the necessity of these residues for GPCR-GRK interactions (26). Although it seems evident how GRKs achieve an active conformation, one can only infer the mechanism in which an active receptor would stabilize and potentiate GRK activity. Recently, a structure of -arrestin complexed to a GPCR phosphopeptide provided particular evidence of a receptor interacting interface to -arrestin (227). Structural understanding of GRK complexed to the receptor would greatly aid in unveiling precisely how this interaction occurs. Although no such structural evidence currently exists, it is known that after a signaling event, the whole process of desensitization starts by phosphorylation of the activated receptor by GRKs. In particular, GRKs phosphorylate at one or more Ser/Thr residues located on the intracellular domains of the receptor, particularly sites located in the COOH terminus and in the intracellular loop between TM5 and TM6 of the receptor (127). Docking of GRKs to active receptors has been proposed to require the NH2 terminus of GRKs (26, 103, 173) as well as other regions outside the kinase domain (10, 64). In addition, in order for GRKs to phosphorylate active GPCRs efficiently, they require the presence of a cytoplasmic pocket (not present in the receptor’s inactive state) as well as the presence of negatively charged lipids (46, 204, 236). The size and physical properties of this cytoplasmic pocket in GPCRs are expected to be highly conserved while the sequence and size of the cytoplasmic loops of the receptors may greatly differ. Thus the conservation of this complimentary cytoplasmic pocket within various GPCRs potentially allows GRKs to phosphorylate a broad array of GPCR substrates. The rationale behind this hypothesis lies in the fact that this pocket in the activated receptor would fit in conformation and charge to that of GRKs in their active Physiol Rev • VOL 95 • APRIL 2015 • www.prv.org G PROTEIN-COUPLED RECEPTOR KINASES conformation. Once docked, the kinase would adopt a closed conformation and lead to phosphorylation of substrates in close proximity (104). The RH domain within the NH2 terminus (FIGURE 2) of GRKs has also been implicated in GPCR phosphorylation. Canonical RGS proteins are GTPase activating proteins (GAP), attenuating G protein-mediated signaling by promoting GTPase activity of GTP-G␣ (reviewed in Ref. 102). GRK2 and GRK3 can bind to G␣q through its RH domain (36). However, RH domains of GRKs have low or no GAP activity, and their ability to halt signaling is primarily due to directly binding and sequestering activated G␣q (36) or direct hindrance of GPCRs (63, 64). In addition, GRK-RH domain-mediated signaling can also occur independently of the receptor-G␣q process. GRK2 is capable of scavenging G␣q/11 inhibiting insulin-induced glucose transport (254). Likewise, it can inhibit endothelin-1-mediated glucose transport by interfering with G␣q/11(242). Recently, GRK2 has been shown to specifically regulate insulin receptor signaling in the heart by phosphorylating IRS-1 and blocking glucose transporter membrane translocation (50), which demonstrates a physiological role for GRK2 acting towards a non-GPCR substrate. E. Regulation of GRKs Canonically, there is the necessity for GRKs to be regulated at the moment it phosphorylates activated receptors. Phosphorylated active receptors allow for the binding of -arrestins, which triggers the formation of clathrin-coated pits and progression through endocytic pathways (see FIGURE 1). These internalized compartments may contain receptors, GRK2, -arrestin, as well as other proteins characteristic of endocytic vesicles (reviewed in Ref. 163). Once internalized, these vesicles are sorted for degradation (desensitization) or recycling (resensitization). The presence of GRKs in these internalized active-receptor vesicles may physically prevent the kinase from performing its function on other activated GPCRs. Additionally, prior to vesicle formation and internalization, the binding of -arrestin to the active-receptor-GRK complex leads to further recruitment of other proteins. One of these recruited proteins is Src, which has been reported to phosphorylate GRK2, diminishing its activity (177). Recently, it has been demonstrated that -arrestin association to the phosphorylated receptor occurs in a biphasic mode. First, there is a “loose” hanging interaction between the C-tail of the receptor and the NH2-terminal domain of arrestin. Analogous to a fishing line, the receptor samples for potential interactions at high rate. Second, there is an insertion of the finger loop into the receptor core leading to longitudinal arrangement of arrestin, also known as fully engaged “tight” interaction (228). This initial “fishing” of the receptor is only possible after the receptor has been phosphorylated by GRKs. Subsequent signaling, also known as GPCR biased signaling, occurs after -arrestin is recruited to the phosphorylated receptor, a topic which is further expanded in section IIF. Although circulating agonists, such as catecholamines, can induce activation of GRKs mediated by GPCRs, multiple molecular mechanisms have been proposed to regulate GRKs in the cellular cytoplasm. While some regulatory mechanisms may be common to all GRKs, the fine tuning of kinase activity may be different for each GRK subtype. GRK1 has been shown to be capable of regulating its activity by autophosphorylation at Ser21, Ser488, and Thr489 (31, 173). In addition, while having no effect on GRK2, the calcium-binding protein recoverin is able to inhibit GRK1. As calcium levels change in response to changes in light, recoverin regulates GRK1 (40, 280). In HEK cells, PKA directly binds to and phosphorylates GRK2 at Ser685, enhancing G␥ binding and promoting membrane translocation (54). PKC has been shown to modulate GRK5 and GRK2. PKC is able to phosphorylate GRK5 and inhibit its activity severalfold due to both decreased affinity and activity for the active receptor (195). PKC-mediated GRK5 phosphorylation most likely occurs at Ser572, and either Ser566 or Ser568, although PKC can also phosphorylate autoregulatory sites Ser484 and/or Thr485 (195). On the other hand, PKC phosphorylation enhances GRK2 activity two- to threefold, possibly by increasing the ability of GRK2 to bind membranes and by disinhibiting tonic calmodulin regulation (48, 131, 276). GRK5 has also been shown to be modulated by calmodulin through a calmodulin-binding domain on GRK5 (197). GRK2 is a short-lived protein (half-life of ⬃1 h in HEK, COS-7, Jurkat, and C6 glioma cells) that is polyubiquitinated and actively degraded by the proteasome proteolytic pathway with increasing degradation in response to activation of 2-ARs (177, 180). Interestingly, in HL60 cells, the half-life of GRK2 was estimated to be ⬃20 h (148). With such a relative short half-life, transcriptional regulation might be an important factor for GRK regulation, although little is known about molecular mechanisms directly involved in modulating GRK mRNA levels. Initially, the GRK2 promoter was considered to be a general “housekeeping” gene (181). Studies of the GRK2 promoter region revealed several notable features, which included no evidence for TATA box, absence of CCAAT boxes in the proximal region upstream of the predicted start site, and the first 300 bases immediately upstream of the ATG are extremely GC rich (87%) (181). In addition, there are predicted secondary structures in the 5’ region of the mRNA, which may serve as posttranscriptional regulators of expression (181). Nevertheless, evidence does exist on potential modulators of GRK2 mRNA content. In the heart, circulating catecholamines and -AR activity correlate with GRK2 mRNA expression (111). Mitogenic T-cell stimulation by exposing mononuclear leukocytes to PHA led to increased GRK2 mRNA levels, while no change was observed in Physiol Rev • VOL 95 • APRIL 2015 • www.prv.org 383 SATO ET AL. mRNA expression of GRK5 and GRK6 (59). More intriguing are the analysis of the human GRK2 gene promoter in aortic smooth muscle cells, where agents that led to physiological vasoconstriction or hypertrophy increased GRK2 promoter activity, and on the contrary, proinflammatory cytokines such as interleukin-1, tumor necrosis factor-␣, or interferon-␥ decreased the activity of the GRK2 promoter (202). As mentioned above, active GPCR-GRK complex recruits -arrestins. -Arrestins can also interact with the cytosolic tyrosine kinase, c-Src, recruiting it to the complex. c-Src has been shown to phosphorylate GRK2 on tyrosine residues, marking it for degradation (177). In addition, in vitro studies have shown that c-Src modulates ␣1B-AR activity through GRK2 and GRK3 (5) even though in vivo experiments show that GRK2 has no effect towards ␣1B-ARs (68). Moreover, GRK2 can also be phosphorylated by p38 (141) and ERK1 (188) mitogen-activated protein (MAP) kinases at Ser670. This phosphorylation results in diminished activity (less phosphorylation of the active receptor) (188) and increased degradation (71). The phosphorylation of Ser670 of GRK2 by MAP kinases has recently been shown to cause the localization of this GRK2 to mitochondria (43), which will be discussed in more detail below. Specifically relevant to cardiovascular regulation, mechanical stretch has also been implicated in activating GRKs. In neonatal rat ventricular myocytes, mechanical stretch led to activation of GRK2 through angiotensin II type I receptor, G␣q, and PKC (153). Inflatable balloon stretch in explanted hearts activated GRK5 and GRK6 but not GRK2 (201). In addition, as detailed above, GRK2 and GRK3 contain within their COOH terminus a PH domain that is involved in G␥ binding. Free G␥ binds to these GRKs within this region at multiple sites (34) with high affinity and are required for GPCR phosphorylation (189). Moreover, a regulatory G␥-binding site has also been described at the NH2 terminus of GRK2 (70). Phospholipids have also been reported to modulate the activity of GRKs (34) through the PH domain of GRK2 and GRK3 or through amino acids 547–560 of GRK5 (34, 169, 185, 196). Another regulation at the PH domain level of GRK2 and GRK3 is the ability to bind to phosphatidylinositol 4,5-bisphosphate (PIP2) and other acidic phospholipids. PIP2 binds to the NH2 terminus of the PH domain and is able to increase by threefold GRK2 phosphorylation of membrane receptors (60, 61). Recently, another mode of GRK2-specific regulation has been described as this kinase is capable of being S-nitrosylated, and the dynamic modification at Cys340 when nitric oxide (NO) bioavailability is high causes inhibition of GRK2 activity towards GPCRs (271). GRK2 has been found to interact with endothelial NO synthase (eNOS), and these two molecules reciprocally inhibit one another with eNOS-NO bioavailability altering the in vivo activity 384 of GRK2 (106). Importantly, in studies using a GRK2 knock-in mouse where Cys340 was mutated to a Ser and incapable of being S-nitrosylated, GRK2 activity was higher. This led to increased myocyte cell death after ischemic injury, and these mice were resistant to NO-mediated cardioprotection (106). More recently, studies in heterozygous GRK2 knockout (KO) mice revealed that these mice are more resistant to vascular remodeling, mechanical alterations, and hypertension induced by angiotensin II, partially through the preservation of NO bioavailability since these mice have less GRK2 to inhibit eNOS (9). Therefore, the unique interaction between GRK2 and the eNOS-NO system is a powerful and dynamic mechanism for regulating this GRK isoform, especially in the cardiovascular system. Of particular importance, GRKs have also been implicated in binding and sometimes phosphorylating other nonGPCR substrates. The first description of a non-GPCR substrate for GRKs was tubulin (37, 96, 186), and both GRK2 and GRK5 are capable of phosphorylating tubulin. Interestingly, phosphorylation of tubulin by GRK2 is enhanced in the presence of G␥ and phospholipids (both of which promote GRK localization to the membrane) as well as in the presence of active GPCRs. It is known that active GPCRs can enhance GRK phosphorylation of peptides up to 100-fold (42, 172). Thus one may infer that any potential substrate in close proximity to GRKs might become phosphorylated. This led to the suggestion that phosphorylation of non-GPCR substrates might be related to opportunity and location, being at the right place at the right time. In support of this hypothesis is the “high gain” phosphorylation in the retina (22, 23), phosphorylation of IRS-1 by GRK2 in response to insulin (50) and GRK2 phosphorylation of p38 (183). On the other hand, GRKs have been hypothesized to possess functions beyond its kinase capabilities. GRKs have been proposed to be modulators of cellular functions in a phosphorylation-independent manner due to their ability to interact with a variety of signaling and trafficking proteins, such as actin (79), actinin (80), tubulin (37), G␣ (36), G␥ (187), clathrin (225), PI3K (164), GIT (190), caveolin (36, 88), lipids, etc. GRKs have been placed in the center of regulatory processes involving cell migration (179), metabolism (50, 52, 254), and apoptosis (43). Further investigation is needed to address these GRK-mediated intermolecular interactions and how they link to various cellular processes. Overall, these noncanonical activities of GRKs may play key roles in physiological signaling including in the heart as detailed below. F. GRKs Directing GPCR-Biased Signaling GPCR signaling is rapidly attenuated by GRK phosphorylation of receptors and subsequent binding of the protein -arrestin (191, 237). -Arrestin binding to the activated Physiol Rev • VOL 95 • APRIL 2015 • www.prv.org G PROTEIN-COUPLED RECEPTOR KINASES receptor acts as a clathrin adaptor ultimately triggering the receptor for internalization (91). However, prior to receptor downregulation, activated GPCRs could be “functionally selective” or “biased” towards G protein or -arrestinmediated signaling. It has been shown that the 2-AR cytoplasmic end helices VI and VII adopt two major conformational states depending on its ligand. Receptor agonists primarily affect G protein specific active state of helix VI, whereas -arrestin biased ligands predominantly affect helix VII (140). In addition, the “pattern” of which a receptor is phosphorylated may dictate a “bar code” for -arrestin function. For example, GRK2 phosphorylation of the 2-AR results in waning of signaling and/or receptor internalization, whereas GRK6-phosphorylation of 2-ARs induces recruitment of -arrestin that leads to extracellular signalregulated kinase 1/2 (ERK1/2) signaling (166). Distinct GRK2 and GRK6 phosphorylation sites have been identified on the 2-AR (166). Moreover, work in other receptors has also shown the requirement of GRK2 (and GRK3)mediated receptor phosphorylation for GPCR internalization, and GRK5 and GRK6-mediated receptor phosphorylation for -arrestin-mediated ERK1/2 signaling (121, 123, 126, 207, 222, 285). In support of this GRK-mediated GPCR-biased signaling are the studies using carvedilol, a -AR antagonist that has been shown to be a weak -arrestin-biased agonist that can activate ERK after an apparent action of GRK6 (277). Interestingly, in myocytes, -arrestin “biased” signaling has also been shown to involve AT1Rs, in particular stretchmediated activation of AT1Rs signals through -arrestin “biased” pathways (201). -Arrestin has also been implicated in mediating transactivation of the epidermal growth factor receptor (EGFR) downstream of 1-AR signaling (167, 252). More intriguing is the fact that this -arrestindependent transactivation of EGFR is cardioprotective, independent of G protein activation, and requires the actions GRK5 and GRK6 (167). Interestingly, this novel pathway shows a trend towards increase in activity when GRK2 is absent, which supports the overall hypotheses that biased, -arrestin-dependent signaling is indeed directed by the actions of specific GRKs notion of GRK dependence of -arrestin function (167). In fact, it appears that biased GPCR signaling is determined by which GRK phosphorylates a given receptor (166). Thus GRK phosphorylation of GPCRs is a significant cellular event as it cannot only desensitize the active receptor but also dictate downstream signaling, functionally selecting for G protein or enabling -arrestin-mediated pathways. G. Mouse Models of Altered GRK Levels Undoubtedly mouse models have proven to be an essential tool in understanding in vivo GRK functions. Various mouse models have aided in understanding these multifaceted kinases and their regulation. The first GRK mouse model was presented in Science 1995 by Koch et al. (129). Here, cardiac-specific overexpression of GRK2 in vivo led to reduced functional coupling of -ARs, dampened adenylyl cyclase activity, and attenuated isoproterenol-stimulated myocardial contractility. In the same paper, the authors showed that expression of the -ARKct, the peptide inhibitor of GRK2, led to enhanced contractility in the presence or absence of isoproterenol (129). Many other mouse models followed this initial report as listed in TABLE 3. Of note, it is important to highlight that the only GRK global KO that is embryonically lethal is that of GRK2 (117). This is important to note as particularly significant since GRK2 is the predominant isoform expressed during embryogenesis (220). In fact, GRK2 transcripts are detected at 7.5 days post coitum in multipotent cells in early mesoderm and neural crest (220). Interestingly, in mice, while global GRK2 knockout (KO) is embryonically lethal, cardiacspecific ablation of GRK2 is not (158). In fact, normal heart structure, cardiac function, and gene expression were observed in cardiac-specific GRK2 KOs when Nkx2.5-Cre was used. These mice did exhibit enhanced inotropic sensitivity to isoproterenol, impaired lusitropic tachyphylaxis, and aggravated catecholamine toxicity during chronic -AR stimulation (158). This differs significantly from the situation when GRK2 is eliminated from cardiac myocytes after birth as discussed below (199). Of note, it is important to mention recent studies crossing heterozygous GRK5 and GRK6 knockout mice previously described (84, 85) to generate double GRK5 and GRK6 knockout mice which are embryonically lethal (32). Among genetic in vivo models of GRKs, involving manipulation of GRKs, GRK2 is the best studied isoform, with many mouse models revealing the different structural elements of this kinase (see TABLE 3). The majority of GRKbased genetically engineered mouse models have been targeted to cardiovascular tissues and have paved the way that proves that GRKs, especially GRK2 and GRK5, play critical roles in normal and pathophysiological cardiac regulation and function. The remaining portion of this review will focus on discussions concerning key biologically, physiologically, and translationally significant aspects of cardiovascular GRK function that have been largely gained from mouse models. Importantly, these mouse studies have also been largely complemented by human studies where applicable as well as studies in larger animal species. The understanding of GRK function and regulation provided by these mouse models and other studies provides evidence that GRKs and their targeted inhibition represent a potential new and powerful drug class that may yield new treatments for cardiovascular disorders. Physiol Rev • VOL 95 • APRIL 2015 • www.prv.org 385 SATO ET AL. Table 3. Mouse models of GRKs GRK Isoform Chromosome in Humans 1 13 2 3 11 22 Chromosome in Mouse 8 19 5 4 4 5 5 10 19 6 5 7 3 13 Year of Publication Genotype Phenotype 1999 GRK1 knockout Loss of light-dependent phosphorylation of rhodopsin. Single photon responses became larger and long-lasting. 39 2010 GRK1 overexpression Photoreceptor damage when exposed to bright light 272 1996 GRK2 knockout Embryonic lethality-hypoplasia of ventricular myocardium. Heterozygous mice are supersensitive to -AR stimulation. 117 2006 GRK2-flox knockout (cardiac) Viable mouse, enhanced ionotropy to isoproterenol though develop accelerated catecholamine toxicity to chronic treatment; lusitropic tachyphylaxis. 158 1995 GRK2 overexpression (cardiac) Decreased -AR signaling, attenuated ventricular contractility in the presence of isoproterenol. 129 2002 GRK2 overexpression (vascular smooth muscle restricted) -AR signaling attenuation, vasodilation in response to isoproterenol was attenuated, resting mean blood arterial blood pressure elevation; hypertrophy. 69 1995 ARKct (495–689) (cardiac) Enhanced contractility with or without isoproterenol stimulation 129 2003 ARKnt (50–145) (cardiac) Cardiac hypertrophy, enhanced -AR density, and signaling. 125 2013 GRK2-C340S Loss of nitrosylation-mediated cardioprotection postischemic injury. 106 1997 GRK3 knockout Supersensitivity to olfactory stimuli. 182 1998 GRK3 overexpression (cardiac) Normal -AR biochemical signaling and hemodynamic function. Decreased MAP kinase activity in response to thrombin. 110 2008 GRK3ct (cardiac) Hypertension, ␣1-receptor hyper-responsiveness. 261 GRK4 knockout Not characterized ⫹ 2002 GRK4␥-A142V Hypertension, altered dopamine signaling 73, 268 1996 GRK5 overexpression (cardiac) -Adrenergic receptor desensitization, unchanged ANG II receptor stimulation. 212 1999 GRK5 knockout Exon 6 and 7 flanked by LoxP. Muscarinic supersensitivity and impaired receptor desensitization. 85 2011 GRK5 knockout Exon 3 partially deleted and replaced with gal. Diminished LPS-induced neutrophil infiltration in the lung with no differences in liver and spleen. Decreased cytokine/chemokine levels. 176 2012 GRK5-flox knockout (cardiac) Cardioprotection posttransaortic constriction. 85, 89 2008 GRK5-Q41 (cardiac) No protective effects against increased LV mass and chamber size induced by isoproterenol. 137 2008 GRK5-L41 (cardiac) GRK5-L41 decreases 1-AR signaling by enhancing desensitization. 137 2008 GRK5 overexpression ⌬NLS (cardiac) Normal pathology after transaortic constriction. 157 2013 GRK5 and GRK6 double knockout Embryonically lethal. 32 2003 GRK6 knockout Impaired desensitization of postsynaptic D2-like dopamine receptors and dopaminergic supersensitivity to psychostimulants. Alterations in immune response and inflammation. 76, 84, 124 * *GRK7 is present in cones; therefore, there is no GRK7 equivalent in mouse as these animals are color blind. ⫹ Knockout animal deposited at Jackson Laboratories by Dr. Lefkowitz, yet there is no published work related to this mouse model. 386 Reference Nos. Physiol Rev • VOL 95 • APRIL 2015 • www.prv.org G PROTEIN-COUPLED RECEPTOR KINASES III. G PROTEIN-COUPLED RECEPTOR KINASE 2 AND THE CARDIOVASCULAR SYSTEM A. GRK2 and Heart Failure Heart failure is the end point of many cardiac diseases which include but are not restricted to myocardial infarction, hypertension, coronary artery disease, cardiomyopathies, congenital heart diseases, and others. To prevent heart failure, it is vital to understand the molecular events that interfere with -AR signaling homeostasis. One of the hallmarks of heart failure is increased activation of the sympathetic nervous system, leading to an increase in circulating catecholamines (reviewed in Ref. 151). In the heart, that translates into increased activation of the -ARs. This augmentation in stimulus is thought to be initially a compensatory mechanism, to reestablish cardiac performance, increasing heart rate and contractility. Unfortunately, if this increase in signal transduction remains unabated, it can lead to the deleterious effects seen in heart failure. Data have shown that these pathological events are triggered by enhanced GRK2 activity in both the heart and the sympathetic nervous system (151, 213). The myocardium uses positive chronotropic and ionotropic effects mediated by 1-ARs and 2-ARs through Gs coupling to accomplish the demand elicited by increased agonists. In the nonfailing heart, 75% of -ARs are 1, with distribution patterns fairly similar among all cardiac chambers (reviewed in Ref. 14). Interestingly, chronic stimulation of -ARs has been reported to produce opposing outcomes; stimulation of 1 and 2 would lead to deleterious and cardioprotective effects, respectively (86). Although initially thought to be only present in adipose tissue, functional 3-ARs are also upregulated in the failing myocardium (44, 62). Thus upregulation of active -ARs increases the necessity for GRKs to turn off this increase in -AR signal transduction. Indeed, chronic catecholamine exposure in vivo can lead to upregulated GRK2 (111). Continued activation of 1-ARs and 2-ARs on myocytes following cardiac stress/injury leads to their desensitization via enhanced GRK2 activity and chronically this leads to receptor downregulation. Importantly, a hallmark characteristic of the failing heart is the loss of -AR-mediated inotropic reserve manifested by both a loss (⬃50%) of -AR receptor density but also overdesensitization of remaining receptors, attributed to increased GRK activity (151, 213). Importantly, human studies have provided compelling evidence that during heart failure there is both increased catecholamine circulation as well as increased myocardial levels of GRKs (reviewed in Ref. 178). While in an aging human there are no changes in GRK activities (136), alterations in cardiac GRKs are evident in the development of human heart failure (136, 184, 253). GRK activity was reported to be elevated in end-stage heart failure patients (136). Increased myocardial and lymphocyte levels of GRK2 have been reported in human heart failure (100, 108). Myocardial biopsy samples and peripheral blood lymphocytes from 23 human transplant patients also revealed an increase in both GRK2 and GRK5, although there was no correlation between myocardial and lymphocyte levels. The authors on this study found that in myocardial tissues, the 1/2 ratio was 57/42%, which differs from normal 80/20% ratio, and they also found significant increases in both GRK5 and GRK2 (2). In peripheral blood lymphocytes, the authors observed a substantial increase in GRK2 levels and a 1/2 ratio of 3/96% (2). Human patients with ischemic and dilated cardiomyopathies have elevated GRK2 mRNA levels (3-fold) as well as increased activity (2-fold) (253). GRK2 levels were elevated in all chambers in human hearts of left ventricular overload disorders as well as in dilated cardiomyopathies (67). More recently, mRNA and protein levels of GRKs in left ventricular myocardium were analyzed from 31 patients with advanced heart failure undergoing transplantation. Compared with control nonfailing left ventricular samples, advanced heart failure patients possessed augmented levels of GRK2 and GRK5, but not GRK3 (3). Animal models recapitulating human heart failure have yielded substantial and important mechanisms involving GRKs and how the increase in levels can correlate to the unfavorable prognostic cardiac pathology. These models have been extensively discussed in References 14, 95, and 178. Of note are the studies in rats subjected to surgical coronary artery occlusion. Hypertrophic failing hearts showed increased GRK2 protein and activity while no major change was observed in hypertrophic nonfailing hearts (250). Another study in hypertrophic cardiomyopathic mouse hearts showed increased GRK2 protein expression and activity compared with nontransgenic littermate controls (NLC) (81). In rats subjected to left coronary artery ligation, myocardial mRNA and protein levels of GRK2 and GRK5 were elevated in failing hearts (259). In spontaneously hypertensive heart failure rats, GRK2 increased at the intercalated disk in 6-, 12-, and 24-mo-old animals, while no change was observed in total protein expression (281). In mice, pressure overload following transverse aortic constriction also led to an increase in cytosolic and membrane GRK (47). The most abundant circulating catecholamines are epinephrine, norepinephrine, and dopamine. Circulating epinephrine and norepinephrine primarily derive from two major sources in the body. Sympathetic nerve endings are capable of releasing their own stored norepinephrine directly onto the cardiac muscle. Alternatively, upon acetylcholine stimulation of nicotinic cholinergic receptors at the adrenal medulla, chromaffin cells release previously synthesized and stored epinephrine (mainly) and norepinephrine (reviewed Physiol Rev • VOL 95 • APRIL 2015 • www.prv.org 387 SATO ET AL. in Ref. 151). This is pertinent to heart failure as sympathetic nervous system hyperactivity chronically stimulates -ARs leading to increased GRK levels and worsens prognosis. Adrenal levels of GRK2 have been shown to be upregulated in chronic heart failure, leading to augmented catecholamine release due to downregulation of ␣2-ARs in chromaffin cells (149). Moreover, in rats, modulation of adrenal catecholamine release has been manipulated by overexpression of GRK2 or expression of -ARKct (152). More important are the studies in mice specifically harboring deleted GRK2 in chromaffin cells. At 4 wk postmyocardial infarction, adrenal-targeted GRK2 KO animals showed decreased circulating catecholamines and consequently reduced sympathetic activity. This was associated with enhanced cardiac function and improved -adrenergic reserve compared with control animals (150). Overall, the link between adrenal GRK2 and ␣2-AR-mediated negative feedback on catecholamine release appears important and to have great implication in adverse cardiac remodeling and progression of heart failure. Due to the strong correlation between GRK2 levels and heart failure, GRK2 inhibition has been proposed as a potential treatment for cardiac injury. Studies in a mouse model expressing the -ARKct as a peptide inhibitor of GRK2 has added significant evidence supporting this notion. Cardiac-targeted -ARKct transgenic expression in mice led to a phenotype of significantly enhanced cardiac function and increased sensitivity to acute -AR agonist exposure (129). Reciprocally, cardiac-targeted transgenic mice with enhanced levels of GRK2, at levels found in failing human myocardium, leads to a phenotype of significantly aberrant -AR signaling and a loss of inotropic reserve (129). These mice with cardiac -ARKct expression have also been used to rescue several models of heart failure including dilated cardiomyopathy (210) and hypertrophic cardiomyopathy (82, 97). The Muscle Lim Protein (MLP) KO mouse, which is a model of dilated cardiomyopathy, was the first heart failure mouse model rescued by -ARKct expression as GRK2 inhibition in myocytes from birth resulted in a MLP KO mouse that never developed pathology (210). Calsequestrin (CSQ) is a sarcoplasmic reticulum calcium-binding protein. Mice overexpressing this protein have a severe hypertrophic cardiomyopathy phenotype with shortened survival (97). Surprisingly, mice expressing the -ARKct and overexpressing CSQ have significantly enhanced survival that was synergistically potentiated by -AR blocker treatment (86). This was the first example that GRK2 inhibition could be complementary and even more beneficial than the -blockade, which is a standard of care for human heart failure. The inhibition of GRK2 by -ARKct expression is anticipated to be mixed as it will also block other G␥-dependent signaling processes so to ultimately prove that GRK2 inhibition is the therapeutic target of -ARKct in heart failure. 388 Studies have been carried out using the GRK2 KO mice. As stated, global homozygous GRK2 mice are lethal (117). However, heterozygous KO mice are viable and present with enhanced cardiac function essentially identical to -ARKct transgenic mice (211). Interestingly, these KO mice with 50% less GRK2 expressed in their hearts could be further enhanced functionally with cardiac -ARKct expression (211). GRK2 has also been genetically ablated only in cardiomyocytes at or after birth, and these animals are protected from heart failure development after myocardial infarction showing that GRK2 activity is indeed pathological in the heart following cardiac injury (199). In fact, induction of cardiomyocyte GRK2 gene ablation after postmyocardial infarction in mice significantly improved global cardiac function and reversed adverse ventricular remodeling (199). Overall, these studies in mice show that the primary target of -ARKct expression is GRK2 inhibition, although there appears to be slight intricate mechanisms that are unique to -ARKct expression versus GRK2 KO. One of these is the regulation of the L-type calcium channel that is enhanced with loss of both GRK2 and -ARKct expression (200, 263). -ARKct expression disinhibits the L-type current through G␥ binding (263), while the loss of GRK2 enhances L-type currents independent of G␥ (200). Other mechanistic differences may exist, but these models clearly show that limiting GRK2 activity in the heart after injury prevents and even reverses heart failure. Studies beyond the mouse have solidified GRK2 inhibition via the -ARKct as a viable therapeutic strategy for heart failure (reviewed in Ref. 260). First, adenoviral-mediated intracoronary-mediated myocardial delivery of the ARKct to rabbit models of cardiac dysfunction and heart failure has led to improved cardiac function (221, 248, 273). In fact, when -ARKct was expressed before a myocardial infarction, the prevention of -AR desensitization and downregulation was shown to prevent heart failure development (273). Recently, preclinical studies using adeno-associated virus-serotype-6 (AAV6) to express -ARKct have shown reversal of heart failure in both rats (208) and pigs (198). These data have been submitted to the United States Food and Drug Administration, and a phase I clinical trial utilizing -ARKct gene therapy for GRK2 inhibition is currently underway with a prospective start date in 2016. Additional evidence in support of the potential that GRK2 inhibition has in treating heart failure patients comes from recent studies revealing that paroxetine, a drug that targets serotonin reuptake centrally and that is currently used to treat depression and central nervous system-related disorders, is capable of inhibiting GRK2 as an off-target (249). Paroxetine has been shown to increase myocyte contractility through GRK2 inhibition, and further studies will investigate whether it can improve cardiac function in heart failure models (249). Interestingly, paroxetine is known to Physiol Rev • VOL 95 • APRIL 2015 • www.prv.org G PROTEIN-COUPLED RECEPTOR KINASES have developmental cardiovascular side effects if given to pregnant mothers (154), and this is consistent with GRK2 KO mice (117). Although paroxetine may not be an ideal candidate for heart failure therapy, currently it is a prototype molecule that can lead medicinal chemists to develop the first selective small molecule pharmacological GRK2 inhibitor. Of note, another compound gallein, which is not a candidate for a viable human drug, has been shown recently to reverse the CSQ transgenic mouse model of heart failure (122). Gallein actually targets G␥ binding and so is analogous to -ARKct expression. Although other targets of G␥ binding were found, the primary mechanisms for heart failure reversal with gallein was G␥-GRK2 inhibition (122). Overall, evidence strongly supports the fact that inhibition of GRK2 in treating heart failure patients can be beneficial though -ARKct gene therapy or emerging small molecules, and this will probably become a clinical reality in the near future. B. GRK2 and Acute Cardiac Injury In humans, neurohormonal activation such as adrenergic overdrive has been observed in patients acutely after cardiac stress/injury including after a myocardial infarction (230). In addition, increased levels of GRK2 have also been reported in other human studies of disease states (reviewed in Refs. 14, 27). In animal models of cardiac injury, GRK2 upregulation is one of the first cardiac molecular changes seen (159, 273). Of note is the observation that increased levels of GRK2 correlates with clinical severity and left ventricular stroke volume (3). In a 2-yr follow up study in humans with acute coronary syndrome, GRK2 levels increased during ST-segment elevation in myocardial infarction and correlated with decreased ejection fraction and end-systolic volume (218). In mice, upregulation of GRK2 was observed as early as 7 days after transverse aortic restriction (47), and increased levels of GRK2 appear to precede the prognosis of overt heart failure (7, 109). Therefore, it is clear that GRK2 upregulation in myocardium occurs acutely after myocardial injury with significant involvement in chronic progression of disease. Importantly, studies have recently shown that altered GRK2 levels and activity also have profound and significant effects in the heart following acute cardiac injury (30, 72). First, when cardiac-targeted GRK2 overexpressing transgenic mice are subjected to ischemia/reperfusion (I/R) injury, they present with significantly increased injury (i.e., cardiac infarction size), and this was due to increased myocyte cell death due to apoptosis in the ischemic region (30). Interestingly, -ARKct transgenic mice displayed significant cardioprotection after I/R injury (30). This protection against acute ischemic injury due to GRK2 inhibition with -ARKct was confirmed in cardiac-specific GRK2 KO mice as both mice with loss of cardiomyocyte GRK2 at birth or induced loss of GRK2 in adulthood had significant cardioprotection after I/R injury (72). The mechanisms responsible for the prodeath activity of GRK2 and cardioprotection of lower GRK2 activity and expression are not entirely clear, although in the transgenic study, inhibition of eNOS-NO system via GRK2 was observed while -ARKct increased cardiac NO levels after I/R and improved survival signaling (30). This is especially interesting due to the recent discovery of a dynamic interrelationship between GRK2 and eNOS in the myocyte (106). In the cardioprotected GRK2 KO mice, an inhibition of cytochrome c release from mitochondria was observed as well as decreased myocyte apoptosis due to lower caspase-2 and -9 activities (72). Thus it appears that acute GRK2 inhibition is a target for novel therapeutic intervention as ischemic cardioprotection without the necessity for preconditioning of the myocardium. Paroxetine, as a GRK2 inhibitor, although not ideal for the chronic treatment of heart failure, may be a candidate for acute single-dose administration around the time of reperfusion of postmyocardial infarction patients and is being considered for such preclinical testing due to potential cardioprotective properties. The cause of increased apoptosis after acute ischemia with enhanced GRK2 activity is not entirely understood, but the above studies in GRK2 KO mice are consistent with mitochondrial-dependent cell death pathways being involved. This is especially interesting since studies by our lab (43) and others (83, 168) have shown GRK2 to be localized to mitochondria, which is a novel area of cellular localization for this GRK. This is of particular significance to I/R injury as the mitochondrion is the major source of energy to cells. However, there is still no consensus in functional role for mitochondrial GRK2. Of note, mitochondria from mice overexpressing GRK2 possess premature opening of the membrane permeability transition pore compared with nontransgenic littermate mice (43). Studies in HEK cells have argued that GRK2 overexpression is involved in increasing ATP content and I/R in quadriceps femoris muscle of Cre-deleted GRK2 mice leads to decreased ATP content compared with floxed control mice (83). On the other hand, our lab has shown that GRK2 localization to the mitochondria is detrimental to the cardiac outcome post-I/R. GRK2 has been shown to interact with Hsp90 (148) and to be phosphorylated by ERK at Ser670 (188). In cardiac cells, translocation of GRK2 to the mitochondria is mediated by ERK phosphorylation of GRK2 and Hsp90 binding (43). With the use of geldanamycin or N-acetylcysteine (Hsp90 inhibitor and antioxidant, respectively), post-I/R injury translocation of GRK2 to the mitochondria was attenuated (43). Also, the use of COOH-terminal mutations of GRK2 where Ser670 was replaced with alanine revealed a loss of mitochondrial localization following oxidative stress and, importantly, less apoptosis indicating that GRK2 targeting to the mitochondrial is a prerequisite for its pro-death activities (43). FIGURE 3A shows the proposed mechanism for GRK2 translocation to the mitochondria. FIGURE 3B Physiol Rev • VOL 95 • APRIL 2015 • www.prv.org 389 SATO ET AL. A B Ischemia/Reperfusion (Oxidative stress) GPCR ROS GRK2 ROS NAC ROS BARKCT P ERK GRK2 Hsp90 Geldamycin Mitochondria FIGURE 3. Mitochondrial GRK2 translocation in oxidative stress. A: cellular stressful events (such as ischemia/reperfusion) lead to the generation of reactive oxygen species (ROS) and subsequent activation of extracellular signal-regulated kinases (ERK), which in turn phosphorylate G protein-coupled receptor kinase 2 (GRK2) at residue 670. Phosphorylated GRK2 then interacts with heat shock protein 90 (Hsp90) mediating translocation to the mitochondria. ARKct is a peptide inhibitor of GRK2. Treatment with the antioxidant N-acetylcysteine inhibits ROS generation. Geldamycin (GA) is an inhibitor of Hsp90. B: immunogold electron microscopy of cardiac tissue from nontransgenic littermate control (NLC) on top and GRK2-overexpressing (GRK2Tg) animals on bottom. Gold particle labeling shows GRK2 present at baseline in mitochondria of both genotypes though overexpression of GRK2 seems to also translate to increase amount of GRK2 in the mitochondria. Original experiment first described in Chen et al. (43). Scale bars are 1 m. It is clear that basally GRK2 is already residing within the mitochondria (B), independent of mechanisms shown in A. Therefore, GRK2 may play a role in normal mitochondrial homeostasis. It is not yet clear what this can be, but data suggest mitochondrial GRK2 may regulate ATP levels (83). shows immunogold electron micrographs from cardiac tissue of GRK2-overexpressing mice (GRK2Tg; bottom) and a nontransgenic littermate control mouse (NLC; top). This clearly shows the localization of GRK2 to the mitochondria and that overexpression of GRK2 leads to increased mitochondria GRK2 even at baseline. The functional impact of this localization is not yet clear but under active investigation. C. GRK2 and Hypertension Increase in blood pressure can be mediated through increase in catecholamines (norepinephrine or epinephrine), which act primarily on ␣-ARs (␣1 and ␣2), potentially altering peripheral resistance. Other hypertensive neurohormones such as angiotensin II and endothelin-1 can also induce chronic GPCR activation that can lead to increased peripheral resistance. Alterations in peripheral resistance can ulti- 390 mately lead to an attenuation of vasodilation, subsequently increasing cardiac afterload. Hypertension dramatically increases the risk for ischemic heart disease, which can in turn lead to stroke as well as cardiac and renal failure. Although the kidney and heart are at the core of blood pressure control, the contractile state of the vasculature is of major importance, due to the fact that blood flow is inversely proportional to the radius of the vessel to the fourth power (reviewed in Ref. 99). Interestingly, GRK2 levels are increased in young patients with hypertension compared with both normotensively young and old patients (92). In agreement are the studies in hypertensive patients showing increased peripheral blood lymphocyte GRK2 levels (116). Overall, increased GRK2 levels are correlated with increased blood pressure (94). In hypertensive rat models, there is increased GRK2 in both lymphocytes and vascular smooth muscle (93). Importantly, vascular-targeted increase of GRK2 via transgenesis is sufficient to increase Physiol Rev • VOL 95 • APRIL 2015 • www.prv.org G PROTEIN-COUPLED RECEPTOR KINASES mean arterial blood pressure by ⬃20% compared with control NLC mice (69). The increased levels of GRK2 in vascular smooth muscle were also accompanied by thickening of the vessels and cardiac hypertrophy (69). This was attributed to the enhanced desensitization of GPCRs that relax blood vessels such as 2-ARs (69). Of course, the mechanism for how GRK2 may induce hypertension is not fully understood. Data with -blockers would suggest it may not be entirely due to uncoupling of -ARs, and it is important to keep in mind that the noncanonical actions of GRK2 such as MAP kinase regulation may be in play here. GRK2-dependent changes in blood pressure and vascular homeostasis may also occur within endothelial cells where GRK2 is expressed. Consistent with results in cardiomyocytes (30, 106), lowering GRK2 levels in vascular endothelial cells increases NO bioavailability, which can lead to enhanced vasorelaxation, and this can protect against hypertension in mice (9, 245). Beneficial effects of lowering GRK2 in endothelial cells also include improved insulin signaling as recently shown in spontaneously hypertensive rats (279) and in a mouse model of type 2 diabetes (244). These data coupled with vascular smooth muscle targeting support GRK2 inhibition, not only in heart failure, but for hypertension as well. However, it must be noted that GRK2 has also been shown to be important in regulating endothelial inflammation and oxidative stress (51, 239). For example, lower GRK2 exclusively in murine endothelial cells was recently shown to be associated with increased reactive oxygen species (51). This is intriguing since lower GRK2 in endothelial cells in mice with global loss of GRK2 (heterozygous GRK2 KO mice) are protective against oxidative stress (9). Thus more research is needed to reconcile these findings. Race is also a factor that contributes to the development of hypertension (138, 223). GRK2 levels were measured in a cohort of 133 African-American patients. Quantification of GRK2 levels in lymphocytes of hypertensive patients (systolic pressure above 130 mmHg) showed a 2-fold increase in protein expression and a greater than 40% increase in GRK2 activity (53). In addition, the same study found a direct correlation of GRK2 (but not GRK5) between plasma norepinephrine levels and systolic blood pressure in black adults. Overall, elevated levels of GRK2 in lymphocytes and vascular smooth muscle have been implicated in both human hypertension and animal models of the disease. This increase in GRK2 levels and activity seem to be very pertinent especially when hypertension takes the overt turn to heart failure (99). Many have suggested using levels of GRK2 in lymphocytes as a biomarker in heart failure at least to monitor response to treatment (108). It may also be a risk predictor of heart failure development. IV. G PROTEIN-COUPLED RECEPTOR KINASE 5 AND CARDIAC DISEASE A. GRK5 and Its Role in Pathological Cardiac Hypertrophy and Heart Failure In addition to GRK2, GRK5 is found at high levels in the heart (2, 67). In fact, of all the tissues expressing GRK5 in the body, its highest levels are found in myocardium (134; also see TABLE 1). Interestingly, in myocardial tissue of transplanted hearts, GRK5 was shown to be the most commonly expressed GRK (2). Recently, many studies in human subjects have suggested GRK5 as a key player in the development of cardiac hypertrophy and heart failure. GRK5 levels were increased by 68% in the left ventricle of hearts with dilated cardiomyopathy and by 48% in volumeoverload patients (67). In the failing myocardium, GRK5 protein was upregulated, and an increase in GRK5 protein and mRNA was observed in patients treated with -agonists compared with those under -blocker treatment. In this study, -blockade led to GRK5 mRNA levels that were comparable to nonfailing hearts, although protein content only showed a decreased trend compared with failing hearts (3). Finally, in human studies comprised of ischemic, dilated, and nonischemic/nondilated cardiomyopathies, expression levels of GRK5 inversely correlated with left ventricular end-systolic and diastolic diameters (162). On the basis of these human studies, it has been proposed that GRK5 is a potential therapeutic target for the treatment of heart failure (reviewed in Ref. 107). Like GRK2, the canonical function of GRK5 is to terminate GPCR signaling. Indeed, cardiac-targeted GRK5 overexpressing transgenic mice have severely attenuated -AR signaling and myocardial in vivo responsiveness, demonstrating that, like GRK2, this kinase can act as a -AR kinase in vivo (212). Cardiac-targeted overexpression of GRK2 or GRK5 in mice has been shown to result in different regulation of GPCR signaling. For instance, adenosine receptors are targeted by the overexpression of GRK5 but not GRK2, while angiotensin II receptors are targeted by the overexpression of GRK2 and not GRK5 (212). Of importance to cardiac function, recent studies have revealed functions for GRK5 beyond its canonical role of regulating GPCRs. GRK5 can bind to calmodulin with an affinity 40 times higher than GRK2 (215). The binding to calmodulin prevents membrane-mediated signaling, although phosphorylation of soluble substrates is unchanged (49, 79). This binding of calmodulin has been shown to be essential for the non-GPCR activity of GRK5 in the heart as this causes the nuclear accumulation of GRK5 (90). GRK5 has also been shown to bind to DNA and to have an active nuclear localization signal (NLS) corresponding to amino acids 388 –395 in the catalytic domain (see FIGURE 2). Altering the NLS to keep GRK5 out of the nucleus does not appear to significantly affect GPCR kinase activity (120). More Physiol Rev • VOL 95 • APRIL 2015 • www.prv.org 391 SATO ET AL. recently, GRK5 has been shown to possess a nuclear export signal (NES) corresponding to amino acids 259 –265 (see FIGURE 2) (119). Of note, the NLS within the catalytic domain appears to be a common feature of GRK4 subfamily members (119). Following cardiac hypertrophic stimulation, which causes calcium-calmodulin activation, GRK5 translocates to the nucleus where it has noncanonical activity as a class II histone deactylase (HDAC) kinase and induces gene transcription through the derepression of MEF2 (157, 282). This has been shown in transgenic GRK5 overexpressing mice to lead to exaggerated cardiac hypertrophy and accelerated heart failure (157). Importantly, transgenic mice overexpressing a GRK5 with its NLS mutated have normal responses to hypertrophic stimulation showing that it is this novel activity of GRK5 responsible for the pathology (157, 282). To confirm the importance of GRK5 to cardiac pathology when there is abnormal hypertrophic stress, GRK5 KO mice (both global and cardiac-specific) have significantly less hypertrophy and improved function after ventricular pressure overload (89). These data demonstrate the first known pathophysiological role for a noncanonical activity of a GRK, and a schematic of this mechanism of GRK5 in pathological cardiac hypertrophy is shown in FIGURE 4A. Additionally, studies in myocytes of spontaneously hypertensive heart failure rats show GRK5 protein localization to the nucleus (FIGURE 4B), further supporting the notion of GRK5 redistribution in cardiac diseased states. Genome-wide RNA interference in Drosophila identified G protein-coupled receptor kinase (Gprk)2, which in other organisms is homologous to GRK5, to be a conserved regulator of NF⟩ (255). Further studies have also confirmed GRK5 as a mediator of NF⟩ signaling in mammals, with potential implications in cardiac hypertrophy and other cardiovascular pathologies, although the mechanism of action is still not fully understood (114, 170, 232). NF⟩ is a highly regulated dimeric transcription factor present as heterodimers (p50:p65) or homodimers (p50:p50 or p65:p65) (87). Extracellular stimulus induces the activation of I⟩ kinase (IKK)-mediated phosphorylation and degradation of NF⟩ repressor, I⟩␣, causing NF⟩ to be free to shuttle to the nucleus (13, 66). However, this recent view has been challenged by the findings that NF⟩:I⟩␣ complexes are able to continuously shuttle between cytoplasm and nucleus by nuclear transporters (24, 87). With that in mind, studies in HEK and BAEC cells overexpressing GRK5 showed nuclear accumulation of I⟩␣, which was linked to inhibition of NF⟩ signaling. The mechanism suggested in this study was due to a physical interaction between GRK5-RH domain (residues 50 –176) and I⟩␣ NH2 terminus rather than phosphorylative events (232). In addition, in support of this mechanism, intracardiac injection of a NH2-terminal peptide of GRK5 (residues 1–176 containing the RH domain) reduced left ventricular hyper- 392 trophy by inhibiting NF⟩-mediated hypertrophic gene expression (233). A schematic view of this mechanism is shown in FIGURE 5A. Nevertheless, in neonatal myocytes exposed to the hypertrophic agonist, phorbol 12-myristate 13-acetate (PMA), there were increased levels of GRK5, p50, and p65. Expression of dominant negative I⟩␣, usage of N-acetylcysteine, or silencing of p65 showed decreased levels of GRK5. Activation of NF⟩ led to binding of p50 and p65 to the GRK5 promoter and subsequent increase in GRK5 expression after hypertrophic stimuli (115). Conversely to the mechanism proposed in FIGURE 5A, overexpression of GRK5 increased levels of p50 and p65, and silencing of GRK5 led to decreased levels of p50 and p65 and loss of NF⟩ DNA binding activity (114). A schematic of the latter mechanism is shown in FIGURE 5B. Moreover, in other studies, GRK5 has also been implicated in mediating NF⟩ activation in macrophages, and these cells are important in injured myocardium (175, 176). Overexpression of GRK5 in Raw 264.7 macrophages enhanced TNF-␣-mediated NF⟩ activity, and knockdown of GRK5 led to diminished NF⟩ activity, in agreement with the mechanism in FIGURE 5B. Moreover, in macrophages, GRK2 and GRK5 interacted with I⟩␣ NH2 terminus (in agreement with FIGURE 5A), and GRK5 (but not GRK2) phosphorylated I⟩␣ at the same residues as I⟩␣ kinase does (Ser32 and Ser36) (175). Due to the role of NF⟩ signaling in inflammation, studies have also looked at how GRK5 levels modulate inflammation. In a sepsis model, GRK5 KO mice showed less inflammation than its control, with diminished expression of NF⟩-driven genes and decreased phosphorylation of I⟩␣ (170, 176). In agreement, lipopolysaccharide (LPS)-induced I⟩␣ phosphorylation was significantly reduced in macrophages from GRK5 KO mice. LPS-induced p65 translocation to the nucleus and NF⟩ DNA binding was significantly diminished in the GRK5 KO mice (176). B. GRK5 Polymorphism and Its Role in Cardiac Disease Genetic polymorphisms have been suggested to be involved in inter-individual differences in response to -AR activation and its outcome to disease. GRK5 nonsynonymous polymorphisms have been reported in humans while there is none in GRK2 (137). In particular, many studies have looked into GRK5 residue 41 glutamine to leucine polymorphism due to its high prevalence in the population from African genetic background. GRK5-L41 has been reported to represent a gain-of-function polymorphism by enhancing 2-ARs uncoupling during persistent agonist exposure (266). This polymorphism has been suggested to present a greater risk for loss of bronchodilatory function during -AR agonist stimulation in asthma patients (266). Studies in transgenic mice bearing cardiac GRK5-L41 showed an Physiol Rev • VOL 95 • APRIL 2015 • www.prv.org G PROTEIN-COUPLED RECEPTOR KINASES A Epinephrine/Angiotensin II Endothelin-1 GPCR GPCR GRK5 Gq Gq GRK5 Calmodulin GRK5 Calmodulin Exit nucleus GRK5 14-3-3 P P HDAC5 IP3 receptor Calmodulin HDAC5 Hypertrophic genes MEF2 DNA Nucleus B a b c d e f g h enhanced uncoupling of isoproterenol-stimulated -adrenergic signaling compared with GRK5-Q41 or nontransgenic littermate mice (137). Interestingly, GRK5-L41 and GRK5-Q41 show similar nuclear localization and ability to stimulate HDAC nuclear export (282) (see FIGURE 4). In this study, diminished -AR-signaling was viewed to be beneficial as it was interpreted as mimicking -blockade. In fact, African-American GRK5-L41 heart failure patients showed prolonged survival or prolonged time for cardiac transplantation (137). In addition, in a cohort of 2,673 FIGURE 4. Agonist-mediated GRK5 translocation to the nucleus. A: catecholamine or angiotensin II-mediated receptor activation leads to calmodulin activation through Gq. Calmodulin binds to the NH2 terminus of GRK5 dislodging from the plasma membrane and promoting nuclear localization. Nuclear GRK5 interaction to calmodulin is then stabilized by IP3-regulated calcium release. Nuclear GRK5 can act as an HDAC5 kinase, de-repressing MEF2 and inducing hypertrophic gene transcription. On the other hand, endothelin-1 receptor activation leads to its desensitization via GRK5 which cannot interact with calmodulin thus preventing nuclear translocation. B: cardiomyocytes from control rats (left column) and spontaneously hypertensive heart failure rats (SHHF) (right column). Myocytes are shown at different ages which correspond to: 2 (first row), 6 (second row), 12 (third row), and 24 mo old (fourth row). Confocal images labeling for GRK5 reveal a redistribution of GRK5 to the nucleus in SHHF rats. Scale bar equals 50 m. [Image from studies of Yi et al. (281), with permission from John Wiley and Sons, Inc.] acute coronary syndrome patients, improved outcome was observed in African-American patients harboring GRK5L41 (56). Moreover, analysis of human patients carrying GRK5-L41 was found to be protective in treated hypertensive patients with coronary artery disease, although no influence in blood pressure response to antihypertensives was seen (142). Yet, another study, looking at patients with left ventricular apical ballooning syndrome showed an increased prevalence of GRK5-L41 polymorphism (235), although no link to prognosis was drawn in this study. Over- Physiol Rev • VOL 95 • APRIL 2015 • www.prv.org 393 SATO ET AL. A B GPCR GPCR GRK5 GRK5 GRK5 IκBα GRK5 NFκB IκBα NFκB GRK5 GRK5 NFκB NFκB NFκB NFκB IκBα IκBα NFκB IκBα NFκB NFκB IκBα NFκB-driven genes and GRK5 NFκB-driven genes DNA DNA FIGURE 5. Potential mechanisms of interaction involving GRK5 and NF⟩ pathway. A: NF⟩-I⟩␣ complex can shuttle between cytoplasm and nucleus. Alternatively, I⟩␣ can be phosphorylated by I⟩␣-kinase leading to its degradation. Free NF⟩ can then enter the nucleus and activate transcription. GRK5 RH domain can bind to I⟩␣ COOH terminus. Upregulation of GRK5 leads to the increase of nuclear I⟩␣, which can in turn inhibit NF⟩ and NF⟩-driven transcription. B: alternatively, upregulation of GRK5 has been proposed to upregulate NF⟩ proteins (p50 and p65). This upregulation in NF⟩ would lead to its translocation to the nucleus and activation of gene transcription. In addition, NF⟩ can also activate the transcription of GRK5. all, it is important to point out that while nuclear events may be an important factor observed in these polymorphisms, canonical GPCR phosphorylation and desensitization as well as noncanonical induction of -arrestin-biased signaling due to altered GRK5 activity may be a contributing factor to what has been observed with this GRK5 polymorphism. More recently, intronic short tandem repeat (STR) (CAn) polymorphisms of GRK5 have been linked to type 2 diabetes mellitus (T2DM) (278). A cohort of 1,164 patients was classified in four groups (normal fasting glucose, impaired fasting glucose, impaired glucose tolerance, and T2DM), and five intronic CAn alleles in GRK5 were identified. CA16 was identified as the only GRK5 STR to be associated with abnormal blood glucose (278), yet the mechanism in which this would alter transcription is still unknown. Overall, GRK5 polymorphisms represent a potential mechanism in which genetic variability could associate with cardiac disease susceptibility and risk factor. Nevertheless, further investigation needs to address mechanism of action, polymorphisms that are silent versus nonsilent, and which cardiac conditions GRK5 polymorphisms would mostly influence, as there are also reports of GRK5 polymorphisms not associating to certain diseases (74, 247). 394 V. OTHER GRKs AND THE CARDIOVASCULAR SYSTEM A. GRK3 and the Heart GRK3 has been shown to be expressed in the human heart although to a much lesser extent than GRK2 and GRK5 (2, 67, 162). Clinical studies have shown that decreased heart performance inversely correlates with levels of GRK3 (162). Other studies, however, have reported no change in GRK3 levels in heart failure patients (3). Nevertheless, discrepancies such as these may be explained, at least in part, by varying heart failure etiologies, such as the augmented levels of GRK3 in volume overload patients and unchanged levels of GRK3 in dilated cardiomyopathy hearts (67). Studies in mice have been particularly helpful in unveiling the potential functional role of cardiac GRK3 (see TABLE 3). GRK3 KO mice developed normally, albeit displaying impairment in odorant-induced desensitization of cAMP responses (182). Cardiac-restricted expression of GRK3 peptide inhibitor (GRK3ct, analogous to the -ARKct of GRK2) in mice led to hypertension derived from increased cardiac output, hyperkinetic myocardium, and increased ␣1-AR responsiveness (261). No alterations in cardiac mass or left ventricular dimensions were observed in GRK3ct Physiol Rev • VOL 95 • APRIL 2015 • www.prv.org G PROTEIN-COUPLED RECEPTOR KINASES mice at baseline. Nevertheless, after chronic ventricular pressure-overload, preserved cardiac function was observed only in GRK3ct transgenic mice compared with NLC control mice (264). This preservation in function after pressure overload was observed even though there was similar induction of hypertrophic gene expression as seen in control mice (264). Based on this, during development of heart failure, it can be inferred that GRK3 may play a role in receptor responsiveness without modulating hypertrophic responses (as in the case of GRK5). In addition, mice overexpressing GRK3 in the heart have no hypertrophy (68) and possessed normal -AR-signaling both biochemically and functionally, although altered thrombin-mediated signaling was observed (110). In hybrid mice studies, GRK3 overexpression has been highly implicated in diminishing ␣1-adrenergic receptor signaling (68). While studies in mice have provided clues as to potential cardiac responses driven by GRK3, further studies still need to elucidate the role of GRK3 in human heart failure. B. GRK4 and GRK6 in Hypertension To a much lesser extent, GRK4 and GRK6 have also been implicated in cardiac dysfunction. Since the levels of GRK4 and GRK6 in the human heart are rather low (67), it has been hypothesized that most of the cardiac impact by these two isoforms is through an indirect mechanism, possibly through altered blood pressure. GRK4 is the main GRK isoform in the testes, although it is also expressed in the kidneys and brain, and at minor levels in other organs (see TABLE 1) (194, 256). GRK4 has been reported to possess four alternative splice variants (194). Furthermore, GRK4 single nucleotide polymorphisms have been previously reported and include R65L, A142V, and A486V. GRK4A486V has been associated with hypertension in Italian patients (15), in Chinese patients (267), and in an Australian cohort of patients (234). Although in these three studies no association between hypertension and GRK4-R65L or GRK4-A142V variant was seen, increasing copies of GRK4-R65L and GRK4-A142V were associated with reduced atenolol-induced diastolic blood pressure lowering (256). In fact, mice harboring the GRK4-A142V variant had increased arterial blood pressure compared with control animals (73). GRK4-A142V mice have defective coupling between D1 dopamine receptors and GRK4 in the renal proximal tubule; thus the kidneys are unable to properly excrete sodium, leading to hypertension (73). In addition to the above-mentioned human studies, no single site GRK4 polymorphism showed significant association with hypertension in a population from Ghana (275). Yet, in another study, GRK4-A486V has also been implicated with hypertension, as has R65L, but only when in conjunction with other polymorphisms (156). To clarify discrepancies, meta-analysis of all five human studies was recently conducted and subgroup analysis by ethnicity revealed that GRK4-A486V inversely correlated with hypertension among East Asians, while it positively correlates among Europeans. In addition, in Europeans GRK4-R65L also correlated with hypertension (139). Overall, GRK4 polymorphisms may have an impact in the heart by promoting hypertensive phenotypes; however, inconsistent results in human studies have yet to provide solid evidence in this matter. GRK6 has four alternative splice variants (75, 161, 193, 257), and its association with hypertension has been studied to a much lesser extent. GRK6 mRNA has been reported to be barely detectable in human hearts (67). Due to its close relationship with GRK5 and due to its minor expression in the heart, efforts have attempted to determine whether hypertension-mediated heart failure induces changes in GRK6 expression. In a rat model of spontaneous hypertensive heart failure (SHHF), GRK6 expression was increased in 12- and 24-mo-old animals compared with age-matched controls with an increased cytoplasmic-to-membrane ratio as seen by confocal imaging (281). Increased localization to the membrane and kinase activity are proposed to occur because of palmitoylation of GRK6 (241). GRK6-A contains three cysteines in the COOH terminus known to serve as substrates for palmitoylation. GRK6-B (slice variant-B) lacks those palmitoylation sites but has a site for protein kinase phosphorylation, while GRK6-C has none of the these two motifs, and GRK6-D lacks catalytic activity (161, 193). While GRK6 A-C differ in their COOH terminus, which is involved in membrane targeting and receptor interaction, in COS-6 cells GRK6-D is exclusively localized to the nucleus (257). Importantly, three of the GRK6 variants identified in mouse are likely to exist in humans and rats (257). The link between GRK6 levels, GRK6 variants, and hypertension-mediated heart failure still needs further investigation. Immune response and inflammation are important cellular mechanisms that may also impact the heart. Important to note are the studies reporting the involvement of GRK6 in lymphocyte chemotaxis and inflammation (76, 124). Lymphocytes from GRK6 KO mice possess impaired chemotactic ability to respond to CXCL12, which is more pronounced in T cells than B cells (76). This effect is specific to GRK6 as other GRK isoforms were not able to rescue the impaired migratory behavior. Polymorphonuclear neutrophils (PMN) are involved in defense against infection, and leukotriene (LT) B4 is one of the most potent chemoattractants of PMN. Studies in GRK6 KO mice revealed increased PMN response towards LTB4 and stromal cell-derived factor 1 (SDF-1) (124). Loss of GRK6 in mice reduces and enhances chemotaxis in lymphocytes and PMN, respectively, suggesting a cell-specific role of GRK6. Acute inflammation response was also increased in GRK6 KO mice (124), and GRK6 deficiency in mice has been implicated with autoimmune disease related to impaired apoptotic cell clearance (165). Nevertheless, GRK6-mediated immune re- Physiol Rev • VOL 95 • APRIL 2015 • www.prv.org 395 SATO ET AL. sponse and inflammation impact on the heart still remain to be fully elucidated. VI. CONCLUSIONS GPCR signaling is a dynamic process that can quickly adapt to meet cellular demands. This signaling highly depends on proteins that regulate its activity. Two protein families that are intricately linked in the regulation of the activated receptors are the GRKs and -arrestins. GRKs have a wide array of physiological impact, and alterations in GRKs have been linked to many noncardiac pathologies such as bipolar disease (11), Alzheimer’s disease (168), rheumatoid arthritis (145), multiple sclerosis (265), Parkinson’s disease (33), and others. This review focused on GRKs, and in particular, the role of cardiac GRKs in maintaining myocardial function in diseased and nondiseased conditions. GRK2 and GRK5 are the main cardiac isoforms. While both isoforms have been shown to mediate canonical GPCR receptor signaling, unique non-receptor-dependent regulatory roles have been recently uncovered. For example, GRK2 has been reported to be involved in mitochondrial homeostasis and GRK5 in nuclear transduction signaling. The noncanonical localization of these GRKs opens new possibilities and exciting potential, as it provides a new avenue in which GRKs could mechanistically exert function in the myocardium. -Blockers are one of the most widely used drugs in the treatment of hypertension and congestive heart failure. Like -blockers, the GRKs are also involved in terminating -AR signaling. Changes in GRK levels or inactivation of GRKs may reduce or enhance -AR-mediated signaling, subsequently altering downstream signaling pathways. Human studies suggest that GRK2 and GRK5 are increased in expression and activity in various cardiac diseases. Inhibition of GRK2, as seen by the expression of the -ARKct as well as the targeted KO of GRK2 in myocytes, has been shown to improve cardiac function in several animal models of cardiomyopathy. It is well established that alterations in GRK levels lead to changes in signaling pathways, which may regulate apoptosis, inflammation, hypertrophy, and/or transcription. While canonical signaling of GRKs in the heart exacerbates progression to heart failure, novel, noncanonical molecular mechanisms of action for GRK2 and GRK5 in the mitochondria and nucleus, respectively, hold promise for future drug development to limit the pathology evoked by upregulation of these kinases after cardiac stress/ injury. With the elucidation of novel GPCR biased signaling mediated via -arrestins have led to more importance for GRK-mediated phosphorylation as GRKs enable this type of signaling. In fact, which GRK can phosphorylate a given receptor appears to control -arrestin independent signaling. In addition, new evidence on the role of nonabundantly expressed cardiac GRK isoforms (GRK3, GRK4, and 396 GRK6) is intriguing. These isoforms, though expressed at low levels at baseline, may be important and relevant in diseased states. Finally, it is worth emphasizing that the GRKs are expressed at different levels in various tissues, and the challenge remains to understand the role that GRKs play in various cardiac conditions. The overall correlation between GRK levels to different cardiac disease etiologies still remains to be determined, and further investigation will no doubt continue to uncover important translational aspects that GRKs present in the cardiovascular system. ACKNOWLEDGMENTS Present address of M. Schwartz: Advanced Institutes of Convergence Technology, Suwon, South Korea. Address for reprint requests and other correspondence: W. J. Koch, W. W. Smith Chair in Cardiovascular Medicine, Professor and Chair, Dept. of Pharmacology, Director, Center for Translational Medicine, Temple University School of Medicine, 3500 N. Broad St., 940 MERB, Philadelphia, PA 19140 (e-mail: Walter.koch@temple.edu). GRANTS W. J. Koch is the W. W. Smith Chair in Cardiovascular Medicine and is funded by National Heart, Lung, and Blood Institute Grants R37 HL061690, R01 HL085503, P01 HL091799, P01 HL75443 (Project 2), and P01 HL108806 (Project 3). P. Y. Sato is supported by a postdoctoral fellowship from the Great Rivers Affiliate of the American Heart Association. DISCLOSURES No conflicts of interest, financial or otherwise, are declared by the authors. REFERENCES 1. Aguero J, Almenar L, D’Ocon P, Oliver E, Monto F, Moro J, Castello A, Rueda J, Martinez-Dolz L, Sanchez-Lazaro I, Montero JA. Correlation between beta-adrenoceptors and G-protein-coupled receptor kinases in pretransplantation heart failure. Transplant Proc 40: 3014 –3016, 2008. 2. Aguero J, Almenar L, D’Ocon P, Oliver E, Monto F, Rueda J, Vicente D, Martinez-Dolz L, Salvador A. Myocardial and peripheral lymphocytic transcriptomic dissociation of beta-adrenoceptors and G protein-coupled receptor kinases in heart transplantation. J Heart Lung Transplant 28: 1166 –1171, 2009. 3. Aguero J, Almenar L, Monto F, Oliver E, Sanchez-Lazaro I, Vicente D, Martinez-Dolz L, D’Ocon P, Rueda J, Salvador A. Myocardial G protein receptor-coupled kinase expression correlates with functional parameters and clinical severity in advanced heart failure. J Card Fail 18: 53– 61, 2012. 4. Ahmed MR, Bychkov E, Gurevich VV, Benovic JL, Gurevich EV. Altered expression and subcellular distribution of GRK subtypes in the dopamine-depleted rat basal ganglia is not normalized by L-DOPA treatment. J Neurochem 104: 1622–1636, 2008. 5. Alcantara-Hernandez R, Casas-Gonzalez P, Garcia-Sainz JA. Roles of c-Src in alpha1Badrenoceptor phosphorylation and desensitization. Auton Autacoid Pharmacol 28: 29 – 39, 2008. Physiol Rev • VOL 95 • APRIL 2015 • www.prv.org G PROTEIN-COUPLED RECEPTOR KINASES 6. Ambrose C, James M, Barnes G, Lin C, Bates G, Altherr M, Duyao M, Groot N, Church D, Wasmuth JJ. A novel G protein-coupled receptor kinase gene cloned from 4p163. Hum Mol Genet 1: 697–703, 1992. 7. Anderson KM, Eckhart AD, Willette RN, Koch WJ. The myocardial beta-adrenergic system in spontaneously hypertensive heart failure (SHHF) rats. Hypertension 33: 402– 407, 1999. 8. Attwood TK, Findlay JB. Fingerprinting G-protein-coupled receptors. Protein Eng 7: 195–203, 1994. 9. Avendano MS, Lucas E, Jurado-Pueyo M, Martinez-Revelles S, Vila-Bedmar R, Mayor F Jr, Salaices M, Briones AM, Murga C. Increased nitric oxide bioavailability in adult GRK2 hemizygous mice protects against angiotensin II-induced hypertension. Hypertension 63: 369 –375, 2014. 10. Baameur F, Morgan DH, Yao H, Tran TM, Hammitt RA, Sabui S, McMurray JS, Lichtarge O, Clark RB. Role for the regulator of G-protein signaling homology domain of G protein-coupled receptor kinases 5 and 6 in beta 2-adrenergic receptor and rhodopsin phosphorylation. Mol Pharmacol 77: 405– 415, 2010. 11. Barrett TB, Emberton JE, Nievergelt CM, Liang SG, Hauger RL, Eskin E, Schork NJ, Kelsoe JR. Further evidence for association of GRK3 to bipolar disorder suggests a second disease mutation. Psychiatr Genet 17: 315–322, 2007. 12. Bawa T, Altememi GF, Eikenburg DC, Standifer KM. Desensitization of alpha 2Aadrenoceptor signalling by modest levels of adrenaline is facilitated by beta 2-adrenoceptor-dependent GRK3 up-regulation. Br J Pharmacol 138: 921–931, 2003. 13. Beinke S, Ley SC. Functions of NF-kappaB1 and NF-kappaB2 in immune cell biology. Biochem J 382: 393– 409, 2004. 14. Belmonte SL, Blaxall BC. G protein coupled receptor kinases as therapeutic targets in cardiovascular disease. Circ Res 109: 309 –319, 2011. 15. Bengra C, Mifflin TE, Khripin Y, Manunta P, Williams SM, Jose PA, Felder RA. Genotyping of essential hypertension single-nucleotide polymorphisms by a homogeneous PCR method with universal energy transfer primers. Clin Chem 48: 2131–2140, 2002. 16. Benovic JL, DeBlasi A, Stone WC, Caron MG, Lefkowitz RJ. Beta-adrenergic receptor kinase: primary structure delineates a multigene family. Science 246: 235–240, 1989. 17. Benovic JL, Gomez J. Molecular cloning and expression of GRK6. A new member of the G protein-coupled receptor kinase family. J Biol Chem 268: 19521–19527, 1993. 18. Benovic JL, Mayor F Jr, Somers RL, Caron MG, Lefkowitz RJ. Light-dependent phosphorylation of rhodopsin by beta-adrenergic receptor kinase. Nature 321: 869 – 872, 1986. 19. Benovic JL, Mayor F Jr, Staniszewski C, Lefkowitz RJ, Caron MG. Purification and characterization of the beta-adrenergic receptor kinase. J Biol Chem 262: 9026 –9032, 1987. 20. Benovic JL, Onorato JJ, Arriza JL, Stone WC, Lohse M, Jenkins NA, Gilbert DJ, Copeland NG, Caron MG, Lefkowitz RJ. Cloning, expression, and chromosomal localization of beta-adrenergic receptor kinase 2. A new member of the receptor kinase family. J Biol Chem 266: 14939 –14946, 1991. 21. Benovic JL, Strasser RH, Caron MG, Lefkowitz RJ. Beta-adrenergic receptor kinase: identification of a novel protein kinase that phosphorylates the agonist-occupied form of the receptor. Proc Natl Acad Sci USA 83: 2797–2801, 1986. 26. Boguth CA, Singh P, Huang CC, Tesmer JJ. Molecular basis for activation of G proteincoupled receptor kinases. EMBO J 29: 3249 –3259, 2010. 27. Bojic T, Sudar E, Mikhailidis D, Alavantic D, Isenovic E. The role of G protein coupled receptor kinases in neurocardiovascular pathophysiology. Arch Med Sci 8: 970 –977, 2012. 28. Bownds D, Dawes J, Miller J, Stahlman M. Phosphorylation of frog photoreceptor membranes induced by light. Nat New Biol 237: 125–127, 1972. 29. Brenninkmeijer CB, Price SA, Lopez Bernal A, Phaneuf S. Expression of G-proteincoupled receptor kinases in pregnant term and non-pregnant human myometrium. J Endocrinol 162: 401– 408, 1999. 30. Brinks H, Boucher M, Gao E, Chuprun JK, Pesant S, Raake PW, Huang ZM, Wang X, Qiu G, Gumpert A, Harris DM, Eckhart AD, Most P, Koch WJ. Level of G proteincoupled receptor kinase-2 determines myocardial ischemia/reperfusion injury via pro- and anti-apoptotic mechanisms. Circ Res 107: 1140 –1149, 2010. 31. Buczylko J, Gutmann C, Palczewski K. Regulation of rhodopsin kinase by autophosphorylation. Proc Natl Acad Sci USA 88: 2568 –2572, 1991. 32. Burkhalter MD, Fralish GB, Premont RT, Caron MG, Philipp M. Grk5l controls heart development by limiting mTOR signaling during symmetry breaking. Cell Rep 4: 625– 632, 2013. 33. Bychkov ER, Gurevich VV, Joyce JN, Benovic JL, Gurevich EV. Arrestins and two receptor kinases are upregulated in Parkinson’s disease with dementia. Neurobiol Aging 29: 379 –396, 2008. 34. Carman CV, Barak LS, Chen C, Liu-Chen LY, Onorato JJ, Kennedy SP, Caron MG, Benovic JL. Mutational analysis of Gbetagamma and phospholipid interaction with G protein-coupled receptor kinase 2. J Biol Chem 275: 10443–10452, 2000. 35. Carman CV, Benovic JL. G-protein-coupled receptors: turn-ons and turn-offs. Curr Opin Neurobiol 8: 335–344, 1998. 36. Carman CV, Parent JL, Day PW, Pronin AN, Sternweis PM, Wedegaertner PB, Gilman AG, Benovic JL, Kozasa T. Selective regulation of Galpha(q/11) by an RGS domain in the G protein-coupled receptor kinase, GRK2. J Biol Chem 274: 34483–34492, 1999. 37. Carman CV, Som T, Kim CM, Benovic JL. Binding and phosphorylation of tubulin by G protein-coupled receptor kinases. J Biol Chem 273: 20308 –20316, 1998. 38. Chalmers DT, Behan DP. The use of constitutively active GPCRs in drug discovery and functional genomics. Nat Rev Drug Discov 1: 599 – 608, 2002. 39. Chen CK, Burns ME, Spencer M, Niemi GA, Chen J, Hurley JB, Baylor DA, Simon MI. Abnormal photoresponses and light-induced apoptosis in rods lacking rhodopsin kinase. Proc Natl Acad Sci USA 96: 3718 –3722, 1999. 40. Chen CK, Inglese J, Lefkowitz RJ, Hurley JB. Ca2⫹-dependent interaction of recoverin with rhodopsin kinase. J Biol Chem 270: 18060 –18066, 1995. 41. Chen CK, Zhang K, Church-Kopish J, Huang W, Zhang H, Chen YJ, Frederick JM, Baehr W. Characterization of human GRK7 as a potential cone opsin kinase. Mol Vis 7: 305–313, 2001. 42. Chen CY, Dion SB, Kim CM, Benovic JL. Beta-adrenergic receptor kinase. Agonistdependent receptor binding promotes kinase activation. J Biol Chem 268: 7825–7831, 1993. 22. Binder BM, Biernbaum MS, Bownds MD. Light activation of one rhodopsin molecule causes the phosphorylation of hundreds of others. A reaction observed in electropermeabilized frog rod outer segments exposed to dim illumination. J Biol Chem 265: 15333–15340, 1990. 43. Chen M, Sato PY, Chuprun JK, Peroutka RJ, Otis NJ, Ibetti J, Pan S, Sheu SS, Gao E, Koch WJ. Prodeath signaling of G protein-coupled receptor kinase 2 in cardiac myocytes after ischemic stress occurs via extracellular signal-regulated kinase-dependent heat shock protein 90-mediated mitochondrial targeting. Circ Res 112: 1121–1134, 2013. 23. Binder BM, O’Connor TM, Bownds MD, Arshavsky VY. Phosphorylation of nonbleached rhodopsin in intact retinas and living frogs. J Biol Chem 271: 19826 –19830, 1996. 44. Cheng HJ, Zhang ZS, Onishi K, Ukai T, Sane DC, Cheng CP. Upregulation of functional beta(3)-adrenergic receptor in the failing canine myocardium. Circ Res 89: 599 – 606, 2001. 24. Birbach A, Gold P, Binder BR, Hofer E, de Martin R, Schmid JA. Signaling molecules of the NF-kappa B pathway shuttle constitutively between cytoplasm and nucleus. J Biol Chem 277: 10842–10851, 2002. 45. Cherezov V, Rosenbaum DM, Hanson MA, Rasmussen SG, Thian FS, Kobilka TS, Choi HJ, Kuhn P, Weis WI, Kobilka BK, Stevens RC. High-resolution crystal structure of an engineered human beta2-adrenergic G protein-coupled receptor. Science 318: 1258 – 1265, 2007. 25. Bjarnadottir TK, Gloriam DE, Hellstrand SH, Kristiansson H, Fredriksson R, Schioth HB. Comprehensive repertoire and phylogenetic analysis of the G protein-coupled receptors in human and mouse. Genomics 88: 263–273, 2006. 46. Choe HW, Kim YJ, Park JH, Morizumi T, Pai EF, Krauss N, Hofmann KP, Scheerer P, Ernst OP. Crystal structure of metarhodopsin II. Nature 471: 651– 655, 2011. Physiol Rev • VOL 95 • APRIL 2015 • www.prv.org 397 SATO ET AL. 47. Choi DJ, Koch WJ, Hunter JJ, Rockman HA. Mechanism of beta-adrenergic receptor desensitization in cardiac hypertrophy is increased beta-adrenergic receptor kinase. J Biol Chem 272: 17223–17229, 1997. 48. Chuang TT, LeVine H 3rd, De Blasi A. Phosphorylation and activation of beta-adrenergic receptor kinase by protein kinase C. J Biol Chem 270: 18660 –18665, 1995. 49. Chuang TT, Paolucci L, De Blasi A. Inhibition of G protein-coupled receptor kinase subtypes by Ca2⫹/calmodulin. J Biol Chem 271: 28691–28696, 1996. 50. Ciccarelli M, Chuprun JK, Rengo G, Gao E, Wei Z, Peroutka RJ, Gold JI, Gumpert A, Chen M, Otis NJ, Dorn GW 2nd, Trimarco B, Iaccarino G, Koch WJ. G proteincoupled receptor kinase 2 activity impairs cardiac glucose uptake and promotes insulin resistance after myocardial ischemia. Circulation 123: 1953–1962, 2011. 51. Ciccarelli M, Sorriento D, Franco A, Fusco A, Del Giudice C, Annunziata R, Cipolletta E, Monti MG, Dorn GW 2nd, Trimarco B, Iaccarino G. Endothelial G protein-coupled receptor kinase 2 regulates vascular homeostasis through the control of free radical oxygen species. Arterioscler Thromb Vasc Biol 33: 2415–2424, 2013. 52. Cipolletta E, Campanile A, Santulli G, Sanzari E, Leosco D, Campiglia P, Trimarco B, Iaccarino G. The G protein coupled receptor kinase 2 plays an essential role in beta-adrenergic receptor-induced insulin resistance. Cardiovasc Res 84: 407– 415, 2009. 53. Cohn HI, Xi Y, Pesant S, Harris DM, Hyslop T, Falkner B, Eckhart AD. G proteincoupled receptor kinase 2 expression and activity are associated with blood pressure in black Americans. Hypertension 54: 71–76, 2009. 54. Cong M, Perry SJ, Lin FT, Fraser ID, Hu LA, Chen W, Pitcher JA, Scott JD, Lefkowitz RJ. Regulation of membrane targeting of the G protein-coupled receptor kinase 2 by protein kinase A and its anchoring protein AKAP79. J Biol Chem 276: 15192–15199, 2001. 55. Cortese MS, Uversky VN, Dunker AK. Intrinsic disorder in scaffold proteins: getting more from less. Prog Biophys Mol Biol 98: 85–106, 2008. 56. Cresci S, Dorn GW, 2nd Jones PG, Beitelshees AL, Li AY, Lenzini PA, Province MA, Spertus JA, Lanfear DE. Adrenergic-pathway gene variants influence beta-blockerrelated outcomes after acute coronary syndrome in a race-specific manner. J Am Coll Cardiol 60: 898 –907, 2012. 57. Dautzenberg FM, Wille S, Braun S, Hauger RL. GRK3 regulation during CRF- and urocortin-induced CRF1 receptor desensitization. Biochem Biophys Res Commun 298: 303–308, 2002. 58. Dawson TM, Arriza JL, Jaworsky DE, Borisy FF, Attramadal H, Lefkowitz RJ, Ronnett GV. Beta-adrenergic receptor kinase-2 and beta-arrestin-2 as mediators of odorantinduced desensitization. Science 259: 825– 829, 1993. 59. De Blasi A, Parruti G, Sallese M. Regulation of G protein-coupled receptor kinase subtypes in activated T lymphocytes. Selective increase of beta-adrenergic receptor kinase 1 and 2. J Clin Invest 95: 203–210, 1995. 60. DebBurman SK, Ptasienski J, Benovic JL, Hosey MM. G protein-coupled receptor kinase GRK2 is a phospholipid-dependent enzyme that can be conditionally activated by G protein betagamma subunits. J Biol Chem 271: 22552–22562, 1996. 61. DebBurman SK, Ptasienski J, Boetticher E, Lomasney JW, Benovic JL, Hosey MM. Lipid-mediated regulation of G protein-coupled receptor kinases 2 and 3. J Biol Chem 270: 5742–5747, 1995. 62. Dessy C, Balligand JL. Beta3-adrenergic receptors in cardiac and vascular tissues emerging concepts and therapeutic perspectives. Adv Pharmacol 59: 135–163, 2010. 63. Dhami GK, Anborgh PH, Dale LB, Sterne-Marr R, Ferguson SS. Phosphorylationindependent regulation of metabotropic glutamate receptor signaling by G proteincoupled receptor kinase 2. J Biol Chem 277: 25266 –25272, 2002. 64. Dhami GK, Dale LB, Anborgh PH, O’Connor-Halligan KE, Sterne-Marr R, Ferguson SS. G Protein-coupled receptor kinase 2 regulator of G protein signaling homology domain binds to both metabotropic glutamate receptor 1a and Galphaq to attenuate signaling. J Biol Chem 279: 16614 –16620, 2004. 65. Dohlman HG, Thorner J, Caron MG, Lefkowitz RJ. Model systems for the study of seven-transmembrane-segment receptors. Annu Rev Biochem 60: 653– 688, 1991. 66. Dolcet X, Llobet D, Encinas M, Pallares J, Cabero A, Schoenenberger JA, Comella JX, Matias-Guiu X. Proteasome inhibitors induce death but activate NF-kappaB on en- 398 dometrial carcinoma cell lines and primary culture explants. J Biol Chem 281: 22118 – 22130, 2006. 67. Dzimiri N, Muiya P, Andres E, Al-Halees Z. Differential functional expression of human myocardial G protein receptor kinases in left ventricular cardiac diseases. Eur J Pharmacol 489: 167–177, 2004. 68. Eckhart AD, Duncan SJ, Penn RB, Benovic JL, Lefkowitz RJ, Koch WJ. Hybrid transgenic mice reveal in vivo specificity of G protein-coupled receptor kinases in the heart. Circ Res 86: 43–50, 2000. 69. Eckhart AD, Ozaki T, Tevaearai H, Rockman HA, Koch WJ. Vascular-targeted overexpression of G protein-coupled receptor kinase-2 in transgenic mice attenuates beta-adrenergic receptor signaling and increases resting blood pressure. Mol Pharmacol 61: 749 –758, 2002. 70. Eichmann T, Lorenz K, Hoffmann M, Brockmann J, Krasel C, Lohse MJ, Quitterer U. The amino-terminal domain of G-protein-coupled receptor kinase 2 is a regulatory Gbeta gamma binding site. J Biol Chem 278: 8052– 8057, 2003. 71. Elorza A, Penela P, Sarnago S, Mayor F Jr. MAPK-dependent degradation of G proteincoupled receptor kinase 2. J Biol Chem 278: 29164 –29173, 2003. 72. Fan Q, Chen M, Zuo L, Shang X, Huang MZ, Ciccarelli M, Raake P, Brinks H, Chuprun KJ, Dorn GW 2nd, Koch WJ, Gao E. Myocardial ablation of G protein-coupled receptor kinase 2 (GRK2) decreases ischemia/reperfusion injury through an anti-intrinsic apoptotic pathway. PLoS One 8: e66234, 2013. 73. Felder RA, Sanada H, Xu J, Yu PY, Wang Z, Watanabe H, Asico LD, Wang W, Zheng S, Yamaguchi I, Williams SM, Gainer J, Brown NJ, Hazen-Martin D, Wong LJ, Robillard JE, Carey RM, Eisner GM, Jose PA. G protein-coupled receptor kinase 4 gene variants in human essential hypertension. Proc Natl Acad Sci USA 99: 3872–3877, 2002. 74. Figtree GA, Bagnall RD, Abdulla I, Buchholz S, Galougahi KK, Yan W, Tan T, Neil C, Horowitz JD, Semsarian C, Ward MR. No association of G-protein-coupled receptor kinase 5 or beta-adrenergic receptor polymorphisms with Takotsubo cardiomyopathy in a large Australian cohort. Eur J Heart Fail 15: 730 –733, 2014. 75. Firsov D, Elalouf JM. Molecular cloning of two rat GRK6 splice variants. Am J Physiol Cell Physiol 273: C953–C961, 1997. 76. Fong AM, Premont RT, Richardson RM, Yu YR, Lefkowitz RJ, Patel DD. Defective lymphocyte chemotaxis in beta-arrestin2- and GRK6-deficient mice. Proc Natl Acad Sci USA 99: 7478 –7483, 2002. 77. Foord SM, Bonner TI, Neubig RR, Rosser EM, Pin JP, Davenport AP, Spedding M, Harmar AJ. International Union of Pharmacology. XLVI. G protein-coupled receptor list. Pharmacol Rev 57: 279 –288, 2005. 78. Fredriksson R, Lagerstrom MC, Lundin LG, Schioth HB. The G-protein-coupled receptors in the human genome form five main families. Phylogenetic analysis, paralogon groups, and fingerprints. Mol Pharmacol 63: 1256 –1272, 2003. 79. Freeman JL, De La Cruz EM, Pollard TD, Lefkowitz RJ, Pitcher JA. Regulation of G protein-coupled receptor kinase 5 (GRK5) by actin. J Biol Chem 273: 20653–20657, 1998. 80. Freeman JL, Pitcher JA, Li X, Bennett V, Lefkowitz RJ. ␣-Actinin is a potent regulator of G protein-coupled receptor kinase activity and substrate specificity in vitro. FEBS Lett 473: 280 –284, 2000. 81. Freeman K, Colon-Rivera C, Olsson MC, Moore RL, Weinberger HD, Grupp IL, Vikstrom KL, Iaccarino G, Koch WJ, Leinwand LA. Progression from hypertrophic to dilated cardiomyopathy in mice that express a mutant myosin transgene. Am J Physiol Heart Circ Physiol 280: H151–H159, 2001. 82. Freeman K, Lerman I, Kranias EG, Bohlmeyer T, Bristow MR, Lefkowitz RJ, Iaccarino G, Koch WJ, Leinwand LA. Alterations in cardiac adrenergic signaling and calcium cycling differentially affect the progression of cardiomyopathy. J Clin Invest 107: 967– 974, 2001. 83. Fusco A, Santulli G, Sorriento D, Cipolletta E, Garbi C, Dorn GW 2nd, Trimarco B, Feliciello A, Iaccarino G. Mitochondrial localization unveils a novel role for GRK2 in organelle biogenesis. Cell Signal 24: 468 – 475, 2012. 84. Gainetdinov RR, Bohn LM, Sotnikova TD, Cyr M, Laakso A, Macrae AD, Torres GE, Kim KM, Lefkowitz RJ, Caron MG, Premont RT. Dopaminergic supersensitivity in G protein-coupled receptor kinase 6-deficient mice. Neuron 38: 291–303, 2003. Physiol Rev • VOL 95 • APRIL 2015 • www.prv.org G PROTEIN-COUPLED RECEPTOR KINASES 85. Gainetdinov RR, Bohn LM, Walker JK, Laporte SA, Macrae AD, Caron MG, Lefkowitz RJ, Premont RT. Muscarinic supersensitivity and impaired receptor desensitization in G protein-coupled receptor kinase 5-deficient mice. Neuron 24: 1029 –1036, 1999. 86. Gauthier C, Tavernier G, Charpentier F, Langin D, Le Marec H. Functional beta3adrenoceptor in the human heart. J Clin Invest 98: 556 –562, 1996. 87. Ghosh S, Karin M. Missing pieces in the NF-kappaB puzzle. Cell 109 Suppl: S81–96, 2002. 88. Gildea JJ, Israel JA, Johnson AK, Zhang J, Jose PA, Felder RA. Caveolin-1 and dopamine-mediated internalization of NaKATPase in human renal proximal tubule cells. Hypertension 54: 1070 –1076, 2009. 89. Gold JI, Gao E, Shang X, Premont RT, Koch WJ. Determining the absolute requirement of G protein-coupled receptor kinase 5 for pathological cardiac hypertrophy: short communication. Circ Res 111: 1048 –1053, 2012. 90. Gold JI, Martini JS, Hullmann J, Gao E, Chuprun JK, Lee L, Tilley DG, Rabinowitz JE, Bossuyt J, Bers DM, Koch WJ. Nuclear translocation of cardiac G protein-coupled receptor kinase 5 downstream of select Gq-activating hypertrophic ligands is a calmodulin-dependent process. PLoS One 8: e57324, 2012. 91. Goodman OB Jr, Krupnick JG, Santini F, Gurevich VV, Penn RB, Gagnon AW, Keen JH, Benovic JL. Beta-arrestin acts as a clathrin adaptor in endocytosis of the beta2-adrenergic receptor. Nature 383: 447– 450, 1996. 92. Gros R, Benovic JL, Tan CM, Feldman RD. G-protein-coupled receptor kinase activity is increased in hypertension. J Clin Invest 99: 2087–2093, 1997. 93. Gros R, Chorazyczewski J, Meek MD, Benovic JL, Ferguson SS, Feldman RD. G-protein-coupled receptor kinase activity in hypertension: increased vascular and lymphocyte G-protein receptor kinase-2 protein expression. Hypertension 35: 38 – 42, 2000. 94. Gros R, Tan CM, Chorazyczewski J, Kelvin DJ, Benovic JL, Feldman RD. G-proteincoupled receptor kinase expression in hypertension. Clin Pharmacol Ther 65: 545–551, 1999. 95. Gurevich EV, Tesmer JJ, Mushegian A, Gurevich VV. G protein-coupled receptor kinases: more than just kinases and not only for GPCRs. Pharmacol Ther 133: 40 – 69, 2012. 96. Haga K, Ogawa H, Haga T, Murofushi H. GTP-binding-protein-coupled receptor kinase 2 (GRK2) binds and phosphorylates tubulin. Eur J Biochem 255: 363–368, 1998. 97. Harding VB, Jones LR, Lefkowitz RJ, Koch WJ, Rockman HA. Cardiac beta ARK1 inhibition prolongs survival and augments beta blocker therapy in a mouse model of severe heart failure. Proc Natl Acad Sci USA 98: 5809 –5814, 2001. 98. Haribabu B, Snyderman R. Identification of additional members of human G-proteincoupled receptor kinase multigene family. Proc Natl Acad Sci USA 90: 9398 –9402, 1993. 99. Harris DM, Cohn HI, Pesant S, Eckhart AD. GPCR signalling in hypertension: role of GRKs. Clin Sci 115: 79 – 89, 2008. 106. Huang ZM, Gao E, Fonseca FV, Hayashi H, Shang X, Hoffman NE, Chuprun JK, Tian X, Tilley DG, Madesh M, Lefer DJ, Stamler JS, Koch WJ. Convergence of G proteincoupled receptor and S-nitrosylation signaling determines the outcome to cardiac ischemic injury. Sci Signal 6: ra95, 2013. 107. Huang ZM, Gold JI, Koch WJ. G protein-coupled receptor kinases in normal and failing myocardium. Front Biosci 16: 3047–3060, 2011. 108. Iaccarino G, Barbato E, Cipolletta E, De Amicis V, Margulies KB, Leosco D, Trimarco B, Koch WJ. Elevated myocardial and lymphocyte GRK2 expression and activity in human heart failure. Eur Heart J 26: 1752–1758, 2005. 109. Iaccarino G, Keys JR, Rapacciuolo A, Shotwell KF, Lefkowitz RJ, Rockman HA, Koch WJ. Regulation of myocardial betaARK1 expression in catecholamine-induced cardiac hypertrophy in transgenic mice overexpressing alpha1B-adrenergic receptors. J Am Coll Cardiol 38: 534 –540, 2001. 110. Iaccarino G, Rockman HA, Shotwell KF, Tomhave ED, Koch WJ. Myocardial overexpression of GRK3 in transgenic mice: evidence for in vivo selectivity of GRKs. Am J Physiol Heart Circ Physiol 275: H1298 –H1306, 1998. 111. Iaccarino G, Tomhave ED, Lefkowitz RJ, Koch WJ. Reciprocal in vivo regulation of myocardial G protein-coupled receptor kinase expression by beta-adrenergic receptor stimulation and blockade. Circulation 98: 1783–1789, 1998. 112. Inglese J, Freedman NJ, Koch WJ, Lefkowitz RJ. Structure and mechanism of the G protein-coupled receptor kinases. J Biol Chem 268: 23735–23738, 1993. 113. Inglese J, Koch WJ, Caron MG, Lefkowitz RJ. Isoprenylation in regulation of signal transduction by G-protein-coupled receptor kinases. Nature 359: 147–150, 1992. 114. Islam KN, Bae JW, Gao E, Koch WJ. Regulation of nuclear factor kappaB (NF-kappaB) in the nucleus of cardiomyocytes by G protein-coupled receptor kinase 5 (GRK5). J Biol Chem 288: 35683–35689, 2013. 115. Islam KN, Koch WJ. Involvement of nuclear factor kappaB (NF-kappaB) signaling pathway in regulation of cardiac G protein-coupled receptor kinase 5 (GRK5) expression. J Biol Chem 287: 12771–12778, 2012. 116. Izzo R, Cipolletta E, Ciccarelli M, Campanile A, Santulli G, Palumbo G, Vasta A, Formisano S, Trimarco B, Iaccarino G. Enhanced GRK2 expression and desensitization of betaAR vasodilatation in hypertensive patients. Clin Transl Sci 1: 215–220, 2008. 117. Jaber M, Koch WJ, Rockman H, Smith B, Bond RA, Sulik KK, Ross J Jr, Lefkowitz RJ, Caron MG, Giros B. Essential role of beta-adrenergic receptor kinase 1 in cardiac development and function. Proc Natl Acad Sci USA 93: 12974 –12979, 1996. 118. Jiang X, Benovic JL, Wedegaertner PB. Plasma membrane and nuclear localization of G protein coupled receptor kinase 6A. Mol Biol Cell 18: 2960 –2969, 2007. 119. Johnson LR, Robinson JD, Lester KN, Pitcher JA. Distinct structural features of G protein-coupled receptor kinase 5 (GRK5) regulate its nuclear localization and DNAbinding ability. PLoS One 8: e62508, 2013. 120. Johnson LR, Scott MG, Pitcher JA. G protein-coupled receptor kinase 5 contains a DNA-binding nuclear localization sequence. Mol Cell Biol 24: 10169 –10179, 2004. 100. Hata JA, Williams ML, Schroder JN, Lima B, Keys JR, Blaxall BC, Petrofski JA, Jakoi A, Milano CA, Koch WJ. Lymphocyte levels of GRK2 (betaARK1) mirror changes in the LVAD-supported failing human heart: lower GRK2 associated with improved betaadrenergic signaling after mechanical unloading. J Card Fail 12: 360 –368, 2006. 121. Jones BW, Song GJ, Greuber EK, Hinkle PM. Phosphorylation of the endogenous thyrotropin-releasing hormone receptor in pituitary GH3 cells and pituitary tissue revealed by phosphosite-specific antibodies. J Biol Chem 282: 12893–12906, 2007. 101. Hisatomi O, Matsuda S, Satoh T, Kotaka S, Imanishi Y, Tokunaga F. A novel subtype of G-protein-coupled receptor kinase, GRK7, in teleost cone photoreceptors. FEBS Lett 424: 159 –164, 1998. 122. Kamal FA, Mickelsen DM, Wegman KM, Travers JG, Moalem J, Hammes SR, Smrcka AV, Blaxall BC. Simultaneous adrenal and cardiac GPCR-Gbeta gamma inhibition halts heart failure progression. J Am Coll Cardiol 2014. 102. Hollinger S, Hepler JR. Cellular regulation of RGS proteins: modulators and integrators of G protein signaling. Pharmacol Rev 54: 527–559, 2002. 123. Kara E, Crepieux P, Gauthier C, Martinat N, Piketty V, Guillou F, Reiter E. A phosphorylation cluster of five serine and threonine residues in the C-terminus of the follicle-stimulating hormone receptor is important for desensitization but not for beta-arrestin-mediated ERK activation. Mol Endocrinol 20: 3014 –3026, 2006. 103. Huang CC, Orban T, Jastrzebska B, Palczewski K, Tesmer JJ. Activation of G proteincoupled receptor kinase 1 involves interactions between its N-terminal region and its kinase domain. Biochemistry 50: 1940 –1949, 2011. 104. Huang CC, Tesmer JJ. Recognition in the face of diversity: interactions of heterotrimeric G proteins and G protein-coupled receptor (GPCR) kinases with activated GPCRs. J Biol Chem 286: 7715–7721, 2011. 105. Huang CC, Yoshino-Koh K, Tesmer JJ. A surface of the kinase domain critical for the allosteric activation of G protein-coupled receptor kinases. J Biol Chem 284: 17206 – 17215, 2009. 124. Kavelaars A, Vroon A, Raatgever RP, Fong AM, Premont RT, Patel DD, Lefkowitz RJ, Heijnen CJ. Increased acute inflammation, leukotriene B4-induced chemotaxis, and signaling in mice deficient for G protein-coupled receptor kinase 6. J Immunol 171: 6128 – 6134, 2003. 125. Keys JR, Greene EA, Cooper CJ, Naga Prasad SV, Rockman HA, Koch WJ. Cardiac hypertrophy and altered beta-adrenergic signaling in transgenic mice that express the amino terminus of beta-ARK1. Am J Physiol Heart Circ Physiol 285: H2201–H2211, 2003. Physiol Rev • VOL 95 • APRIL 2015 • www.prv.org 399 SATO ET AL. 126. Kim J, Ahn S, Ren XR, Whalen EJ, Reiter E, Wei H, Lefkowitz RJ. Functional antagonism of different G protein-coupled receptor kinases for beta-arrestin-mediated angiotensin II receptor signaling. Proc Natl Acad Sci USA 102: 1442–1447, 2005. 146. Lorenz W, Inglese J, Palczewski K, Onorato JJ, Caron MG, Lefkowitz RJ. The receptor kinase family: primary structure of rhodopsin kinase reveals similarities to the betaadrenergic receptor kinase. Proc Natl Acad Sci USA 88: 8715– 8719, 1991. 127. Kobilka BK. G-protein coupled receptors Springer-Verlag. http://www.springerreference. com/index/chapterdbid/137855 (March 21, 2014). 147. Loudon RP, Benovic JL. Altered activity of palmitoylation-deficient and isoprenylated forms of the G protein-coupled receptor kinase GRK6. J Biol Chem 272: 27422– 27427, 1997. 128. Koch WJ, Inglese J, Stone WC, Lefkowitz RJ. The binding site for the beta gamma subunits of heterotrimeric G proteins on the beta-adrenergic receptor kinase. J Biol Chem 268: 8256 – 8260, 1993. 148. Luo J, Benovic JL. G protein-coupled receptor kinase interaction with Hsp90 mediates kinase maturation. J Biol Chem 278: 50908 –50914, 2003. 129. Koch WJ, Rockman HA, Samama P, Hamilton RA, Bond RA, Milano CA, Lefkowitz RJ. Cardiac function in mice overexpressing the beta-adrenergic receptor kinase or a beta ARK inhibitor. Science 268: 1350 –1353, 1995. 149. Lymperopoulos A, Rengo G, Funakoshi H, Eckhart AD, Koch WJ. Adrenal GRK2 upregulation mediates sympathetic overdrive in heart failure. Nat Med 13: 315–323, 2007. 130. Kolakowski LF Jr. GCRDb: a G-protein-coupled receptor database. Receptors Channels 2: 1–7, 1994. 131. Krasel C, Dammeier S, Winstel R, Brockmann J, Mischak H, Lohse MJ. Phosphorylation of GRK2 by protein kinase C abolishes its inhibition by calmodulin. J Biol Chem 276: 1911–1915, 2001. 132. Krupnick JG, Gurevich VV, Benovic JL. Mechanism of quenching of phototransduction. Binding competition between arrestin and transducin for phosphorhodopsin. J Biol Chem 272: 18125–18131, 1997. 133. Kuhn H, Dreyer WJ. Light dependent phosphorylation of rhodopsin by ATP. FEBS Lett 20: 1– 6, 1972. 134. Kunapuli P, Benovic JL. Cloning and expression of GRK5: a member of the G proteincoupled receptor kinase family. Proc Natl Acad Sci USA 90: 5588 –5592, 1993. 135. Kwatra MM, Schwinn DA, Schreurs J, Blank JL, Kim CM, Benovic JL, Krause JE, Caron MG, Lefkowitz RJ. The substance P receptor, which couples to Gq/11, is a substrate of beta-adrenergic receptor kinase 1 and 2. J Biol Chem 268: 9161–9164, 1993. 150. Lymperopoulos A, Rengo G, Gao E, Ebert SN, Dorn GW 2nd, Koch WJ. Reduction of sympathetic activity via adrenal-targeted GRK2 gene deletion attenuates heart failure progression and improves cardiac function after myocardial infarction. J Biol Chem 285: 16378 –16386, 2010. 151. Lymperopoulos A, Rengo G, Koch WJ. Adrenergic nervous system in heart failure: pathophysiology and therapy. Circ Res 113: 739 –753, 2013. 152. Lymperopoulos A, Rengo G, Zincarelli C, Soltys S, Koch WJ. Modulation of adrenal catecholamine secretion by in vivo gene transfer and manipulation of G proteincoupled receptor kinase-2 activity. Mol Ther 16: 302–307, 2008. 153. Malhotra R, D’Souza KM, Staron ML, Birukov KG, Bodi I, Akhter SA. G alpha(q)mediated activation of GRK2 by mechanical stretch in cardiac myocytes: the role of protein kinase C. J Biol Chem 285: 13748 –13760, 2010. 154. Mangin D, Healy D, Mintzes B. Paroxetine is associated with malformation during pregnancy. BMJ 343: d5060, 2011. 155. Marinissen MJ, Gutkind JS. G-protein-coupled receptors and signaling networks: emerging paradigms. Trends Pharmacol Sci 22: 368 –376, 2001. 136. Leineweber K, Klapproth S, Beilfuss A, Silber RE, Heusch G, Philipp T, Brodde OE. Unchanged G-protein-coupled receptor kinase activity in the aging human heart. J Am Coll Cardiol 42: 1487–1492, 2003. 156. Martinez Cantarin MP, Ertel A, Deloach S, Fortina P, Scott K, Burns TL, Falkner B. Variants in genes involved in functional pathways associated with hypertension in African Americans. Clin Transl Sci 3: 279 –286, 2010. 137. Liggett SB, Cresci S, Kelly RJ, Syed FM, Matkovich SJ, Hahn HS, Diwan A, Martini JS, Sparks L, Parekh RR, Spertus JA, Koch WJ, Kardia SL, Dorn GW 2nd. A GRK5 polymorphism that inhibits beta-adrenergic receptor signaling is protective in heart failure. Nat Med 14: 510 –517, 2008. 157. Martini JS, Raake P, Vinge LE, DeGeorge BR Jr, Chuprun JK, Harris DM, Gao E, Eckhart AD, Pitcher JA, Koch WJ. Uncovering G protein-coupled receptor kinase-5 as a histone deacetylase kinase in the nucleus of cardiomyocytes. Proc Natl Acad Sci USA 105: 12457–12462, 2008. 138. Light KC, Sherwood A. Race, borderline hypertension, and hemodynamic responses to behavioral stress before and after beta-adrenergic blockade. Health Psychol 8: 577–595, 1989. 158. Matkovich SJ, Diwan A, Klanke JL, Hammer DJ, Marreez Y, Odley AM, Brunskill EW, Koch WJ, Schwartz RJ, Dorn GW 2nd. Cardiac-specific ablation of G-protein receptor kinase 2 redefines its roles in heart development and beta-adrenergic signaling. Circ Res 99: 996 –1003, 2006. 139. Liu C, Xi B. Pooled analyses of the associations of polymorphisms in the GRK4 and EMILIN1 genes with hypertension risk. Int J Med Sci 9: 274 –279, 2012. 140. Liu JJ, Horst R, Katritch V, Stevens RC, Wuthrich K. Biased signaling pathways in beta2-adrenergic receptor characterized by 19F-NMR. Science 335: 1106 –1110, 2012. 141. Liu Z, Jiang Y, Li Y, Wang J, Fan L, Scott MJ, Xiao G, Li S, Billiar TR, Wilson MA, Fan J. TLR4 Signaling augments monocyte chemotaxis by regulating G protein-coupled receptor kinase 2 translocation. J Immunol 191: 857– 864, 2013. 142. Lobmeyer MT, Wang L, Zineh I, Turner ST, Gums JG, Chapman AB, Cooper-DeHoff RM, Beitelshees AL, Bailey KR, Boerwinkle E, Pepine CJ, Johnson JA. Polymorphisms in genes coding for GRK2 and GRK5 and response differences in antihypertensivetreated patients. Pharmacogenet Genomics 21: 42– 49, 2011. 143. Lodowski DT, Pitcher JA, Capel WD, Lefkowitz RJ, Tesmer JJ. Keeping G proteins at bay: a complex between G protein-coupled receptor kinase 2 and Gbetagamma. Science 300: 1256 –1262, 2003. 144. Lodowski DT, Tesmer VM, Benovic JL, Tesmer JJ. The structure of G protein-coupled receptor kinase (GRK)-6 defines a second lineage of GRKs. J Biol Chem 281: 16785– 16793, 2006. 145. Lombardi MS, Kavelaars A, Schedlowski M, Bijlsma JW, Okihara KL, Van de Pol M, Ochsmann S, Pawlak C, Schmidt RE, Heijnen CJ. Decreased expression and activity of G-protein-coupled receptor kinases in peripheral blood mononuclear cells of patients with rheumatoid arthritis. FASEB J 13: 715–725, 1999. 400 159. Maurice JP, Shah AS, Kypson AP, Hata JA, White DC, Glower DD, Koch WJ. Molecular beta-adrenergic signaling abnormalities in failing rabbit hearts after infarction. Am J Physiol Heart Circ Physiol 276: H1853–H1860, 1999. 160. Menard L, Ferguson SS, Barak LS, Bertrand L, Premont RT, Colapietro AM, Lefkowitz RJ, Caron MG. Members of the G protein-coupled receptor kinase family that phosphorylate the beta2-adrenergic receptor facilitate sequestration. Biochemistry 35: 4155– 4160, 1996. 161. Moepps B, Vatter P, Frodl R, Waechter F, Dixkens C, Hameister H, Gierschik P. Alternative splicing produces transcripts encoding four variants of mouse G-proteincoupled receptor kinase 6. Genomics 60: 199 –209, 1999. 162. Monto F, Oliver E, Vicente D, Rueda J, Aguero J, Almenar L, Ivorra MD, Barettino D, D’Ocon P. Different expression of adrenoceptors and GRKs in the human myocardium depends on heart failure etiology and correlates to clinical variables. Am J Physiol Heart Circ Physiol 303: H368 –H376, 2012. 163. Moore CA, Milano SK, Benovic JL. Regulation of receptor trafficking by GRKs and arrestins. Annu Rev Physiol 69: 451– 482, 2007. 164. Naga Prasad SV, Barak LS, Rapacciuolo A, Caron MG, Rockman HA. Agonist-dependent recruitment of phosphoinositide 3-kinase to the membrane by beta-adrenergic receptor kinase 1. A role in receptor sequestration. J Biol Chem 276: 18953–18959, 2001. 165. Nakaya M, Tajima M, Kosako H, Nakaya T, Hashimoto A, Watari K, Nishihara H, Ohba M, Komiya S, Tani N, Nishida M, Taniguchi H, Sato Y, Matsumoto M, Tsuda M, Physiol Rev • VOL 95 • APRIL 2015 • www.prv.org G PROTEIN-COUPLED RECEPTOR KINASES Kuroda M, Inoue K, Kurose H. GRK6 deficiency in mice causes autoimmune disease due to impaired apoptotic cell clearance. Nat Commun 4: 1532, 2012. 166. Nobles KN, Xiao K, Ahn S, Shukla AK, Lam CM, Rajagopal S, Strachan RT, Huang TY, Bressler EA, Hara MR, Shenoy SK, Gygi SP, Lefkowitz RJ. Distinct phosphorylation sites on the beta(2)-adrenergic receptor establish a barcode that encodes differential functions of beta-arrestin. Sci Signal 4: ra51, 2011. 167. Noma T, Lemaire A, Naga Prasad SV, Barki-Harrington L, Tilley DG, Chen J, Le Corvoisier P, Violin JD, Wei H, Lefkowitz RJ, Rockman HA. Beta-arrestin-mediated beta1-adrenergic receptor transactivation of the EGFR confers cardioprotection. J Clin Invest 117: 2445–2458, 2007. 168. Obrenovich ME, Palacios HH, Gasimov E, Leszek J, Aliev G. The GRK2 overexpression is a primary hallmark of mitochondrial lesions during early Alzheimer Disease. Cardiovasc Psychiatry Neurol 2009: 327360, 2009. 169. Onorato JJ, Gillis ME, Liu Y, Benovic JL, Ruoho AE. The beta-adrenergic receptor kinase (GRK2) is regulated by phospholipids. J Biol Chem 270: 21346 –21353, 1995. 186. Pitcher JA, Hall RA, Daaka Y, Zhang J, Ferguson SS, Hester S, Miller S, Caron MG, Lefkowitz RJ, Barak LS. The G protein-coupled receptor kinase 2 is a microtubuleassociated protein kinase that phosphorylates tubulin. J Biol Chem 273: 12316 –12324, 1998. 187. Pitcher JA, Inglese J, Higgins JB, Arriza JL, Casey PJ, Kim C, Benovic JL, Kwatra MM, Caron MG, Lefkowitz RJ. Role of beta gamma subunits of G proteins in targeting the beta-adrenergic receptor kinase to membrane-bound receptors. Science 257: 1264 – 1267, 1992. 188. Pitcher JA, Tesmer JJ, Freeman JL, Capel WD, Stone WC, Lefkowitz RJ. Feedback inhibition of G protein-coupled receptor kinase 2 (GRK2) activity by extracellular signal-regulated kinases. J Biol Chem 274: 34531–34534, 1999. 189. Pitcher JA, Touhara K, Payne ES, Lefkowitz RJ. Pleckstrin homology domain-mediated membrane association and activation of the beta-adrenergic receptor kinase requires coordinate interaction with G beta gamma subunits and lipid. J Biol Chem 270: 11707– 11710, 1995. 170. Packiriswamy N, Lee T, Raghavendra PB, Durairaj H, Wang H, Parameswaran N. G-protein-coupled receptor kinase-5 mediates inflammation but does not regulate cellular infiltration or bacterial load in a polymicrobial sepsis model in mice. J Innate Immun 5: 401– 413, 2013. 190. Premont RT, Claing A, Vitale N, Freeman JL, Pitcher JA, Patton WA, Moss J, Vaughan M, Lefkowitz RJ. 2-Adrenergic receptor regulation by GIT1, a G protein-coupled receptor kinase-associated ADP ribosylation factor GTPase-activating protein. Proc Natl Acad Sci USA 95: 14082–14087, 1998. 171. Palczewski K, Benovic JL. G-protein-coupled receptor kinases. Trends Biochem Sci 16: 387–391, 1991. 191. Premont RT, Inglese J, Lefkowitz RJ. Protein kinases that phosphorylate activated G protein-coupled receptors. FASEB J 9: 175–182, 1995. 172. Palczewski K, Buczylko J, Kaplan MW, Polans AS, Crabb JW. Mechanism of rhodopsin kinase activation. J Biol Chem 266: 12949 –12955, 1991. 192. Premont RT, Koch WJ, Inglese J, Lefkowitz RJ. Identification, purification, and characterization of GRK5, a member of the family of G protein-coupled receptor kinases. J Biol Chem 269: 6832– 6841, 1994. 173. Palczewski K, Buczylko J, Lebioda L, Crabb JW, Polans AS. Identification of the N-terminal region in rhodopsin kinase involved in its interaction with rhodopsin. J Biol Chem 268: 6004 – 6013, 1993. 174. Pao CS, Barker BL, Benovic JL. Role of the amino terminus of G protein-coupled receptor kinase 2 in receptor phosphorylation. Biochemistry 48: 7325–7333, 2009. 175. Patial S, Luo J, Porter KJ, Benovic JL, Parameswaran N. G-protein-coupled-receptor kinases mediate TNFalpha-induced NFkappaB signalling via direct interaction with and phosphorylation of IkappaBalpha. Biochem J 425: 169 –178, 2010. 176. Patial S, Shahi S, Saini Y, Lee T, Packiriswamy N, Appledorn DM, Lapres JJ, Amalfitano A, Parameswaran N. G-protein coupled receptor kinase 5 mediates lipopolysaccharide-induced NFkappaB activation in primary macrophages and modulates inflammation in vivo in mice. J Cell Physiol 226: 1323–1333, 2011. 177. Penela P, Elorza A, Sarnago S, Mayor F Jr. Beta-arrestin- and c-Src-dependent degradation of G-protein-coupled receptor kinase 2. EMBO J 20: 5129 –5138, 2001. 178. Penela P, Murga C, Ribas C, Tutor AS, Peregrin S, Mayor F Jr. Mechanisms of regulation of G protein-coupled receptor kinases (GRKs) and cardiovascular disease. Cardiovasc Res 69: 46 –56, 2006. 179. Penela P, Ribas C, Aymerich I, Eijkelkamp N, Barreiro O, Heijnen CJ, Kavelaars A, Sanchez-Madrid F, Mayor F Jr. G protein-coupled receptor kinase 2 positively regulates epithelial cell migration. EMBO J 27: 1206 –1218, 2008. 180. Penela P, Ruiz-Gomez A, Castano JG, Mayor F Jr. Degradation of the G proteincoupled receptor kinase 2 by the proteasome pathway. J Biol Chem 273: 35238 – 35244, 1998. 181. Penn RB, Benovic JL. Structure of the human gene encoding the beta-adrenergic receptor kinase. J Biol Chem 269: 14924 –14930, 1994. 193. Premont RT, Macrae AD, Aparicio SA, Kendall HE, Welch JE, Lefkowitz RJ. The GRK4 subfamily of G protein-coupled receptor kinases. Alternative splicing, gene organization, and sequence conservation. J Biol Chem 274: 29381–29389, 1999. 194. Premont RT, Macrae AD, Stoffel RH, Chung N, Pitcher JA, Ambrose C, Inglese J, MacDonald ME, Lefkowitz RJ. Characterization of the G protein-coupled receptor kinase GRK4. Identification of four splice variants. J Biol Chem 271: 6403– 6410, 1996. 195. Pronin AN, Benovic JL. Regulation of the G protein-coupled receptor kinase GRK5 by protein kinase C. J Biol Chem 272: 3806 –3812, 1997. 196. Pronin AN, Carman CV, Benovic JL. Structure-function analysis of G protein-coupled receptor kinase-5. Role of the carboxyl terminus in kinase regulation. J Biol Chem 273: 31510 –31518, 1998. 197. Pronin AN, Satpaev DK, Slepak VZ, Benovic JL. Regulation of G protein-coupled receptor kinases by calmodulin and localization of the calmodulin binding domain. J Biol Chem 272: 18273–18280, 1997. 198. Raake PW, Schlegel P, Ksienzyk J, Reinkober J, Barthelmes J, Schinkel S, Pleger S, Mier W, Haberkorn U, Koch WJ, Katus HA, Most P, Muller OJ. AAV6 betaARKct cardiac gene therapy ameliorates cardiac function and normalizes the catecholaminergic axis in a clinically relevant large animal heart failure model. Eur Heart J 34: 1437–1447, 2013. 199. Raake PW, Vinge LE, Gao E, Boucher M, Rengo G, Chen X, DeGeorge BR Jr, Matkovich S, Houser SR, Most P, Eckhart AD, Dorn GW 2nd, Koch WJ. G protein-coupled receptor kinase 2 ablation in cardiac myocytes before or after myocardial infarction prevents heart failure. Circ Res 103: 413– 422, 2008. 182. Peppel K, Boekhoff I, McDonald P, Breer H, Caron MG, Lefkowitz RJ. G proteincoupled receptor kinase 3 (GRK3) gene disruption leads to loss of odorant receptor desensitization. J Biol Chem 272: 25425–25428, 1997. 200. Raake PW, Zhang X, Vinge LE, Brinks H, Gao E, Jaleel N, Li Y, Tang M, Most P, Dorn GW, 2nd Houser SR, Katus HA, Chen X, Koch WJ. Cardiac G-protein-coupled receptor kinase 2 ablation induces a novel Ca2⫹ handling phenotype resistant to adverse alterations and remodeling after myocardial infarction. Circulation 125: 2108 –2118, 2012. 183. Peregrin S, Jurado-Pueyo M, Campos PM, Sanz-Moreno V, Ruiz-Gomez A, Crespo P, Mayor F Jr, Murga C. Phosphorylation of p38 by GRK2 at the docking groove unveils a novel mechanism for inactivating p38MAPK. Curr Biol 16: 2042–2047, 2006. 201. Rakesh K, Yoo B, Kim IM, Salazar N, Kim KS, Rockman HA. beta-Arrestin-biased agonism of the angiotensin receptor induced by mechanical stress. Sci Signal 3: ra46, 2010. 184. Petrofski JA, Koch WJ. The beta-adrenergic receptor kinase in heart failure. J Mol Cell Cardiol 35: 1167–1174, 2003. 202. Ramos-Ruiz R, Penela P, Penn RB, Mayor F Jr. Analysis of the human G proteincoupled receptor kinase 2 (GRK2) gene promoter: regulation by signal transduction systems in aortic smooth muscle cells. Circulation 101: 2083–2089, 2000. 185. Pitcher JA, Fredericks ZL, Stone WC, Premont RT, Stoffel RH, Koch WJ, Lefkowitz RJ. Phosphatidylinositol 4,5-bisphosphate (PIP2)-enhanced G protein-coupled receptor kinase (GRK) activity. Location, structure, and regulation of the PIP2 binding site distinguishes the GRK subfamilies. J Biol Chem 271: 24907–24913, 1996. 203. Rankin ML, Marinec PS, Cabrera DM, Wang Z, Jose PA, Sibley DR. The D1 dopamine receptor is constitutively phosphorylated by G protein-coupled receptor kinase 4. Mol Pharmacol 69: 759 –769, 2006. Physiol Rev • VOL 95 • APRIL 2015 • www.prv.org 401 SATO ET AL. 204. Rasmussen SG, Choi HJ, Fung JJ, Pardon E, Casarosa P, Chae PS, Devree BT, Rosenbaum DM, Thian FS, Kobilka TS, Schnapp A, Konetzki I, Sunahara RK, Gellman SH, Pautsch A, Steyaert J, Weis WI, Kobilka BK. Structure of a nanobody-stabilized active state of the beta(2) adrenoceptor. Nature 469: 175–180, 2011. 205. Rasmussen SG, Choi HJ, Rosenbaum DM, Kobilka TS, Thian FS, Edwards PC, Burghammer M, Ratnala VR, Sanishvili R, Fischetti RF, Schertler GF, Weis WI, Kobilka BK. Crystal structure of the human beta2 adrenergic G-protein-coupled receptor. Nature 450: 383–387, 2007. 206. Rasmussen SG, DeVree BT, Zou Y, Kruse AC, Chung KY, Kobilka TS, Thian FS, Chae PS, Pardon E, Calinski D, Mathiesen JM, Shah ST, Lyons JA, Caffrey M, Gellman SH, Steyaert J, Skiniotis G, Weis WI, Sunahara RK, Kobilka BK. Crystal structure of the beta2 adrenergic receptor-Gs protein complex. Nature 477: 549 –555, 2011. 207. Ren XR, Reiter E, Ahn S, Kim J, Chen W, Lefkowitz RJ. Different G protein-coupled receptor kinases govern G protein and beta-arrestin-mediated signaling of V2 vasopressin receptor. Proc Natl Acad Sci USA 102: 1448 –1453, 2005. 223. Sherwood A, Hinderliter AL. Responsiveness to alpha- and beta-adrenergic receptor agonists. Effects of race in borderline hypertensive compared to normotensive men. Am J Hypertens 6: 630 – 635, 1993. 224. Shichi H, Somers RL. Light-dependent phosphorylation of rhodopsin. Purification and properties of rhodopsin kinase. J Biol Chem 253: 7040 –7046, 1978. 225. Shiina T, Arai K, Tanabe S, Yoshida N, Haga T, Nagao T, Kurose H. Clathrin box in G protein-coupled receptor kinase 2. J Biol Chem 276: 33019 –33026, 2001. 226. Shoemaker BA, Portman JJ, Wolynes PG. Speeding molecular recognition by using the folding funnel: the fly-casting mechanism. Proc Natl Acad Sci USA 97: 8868 – 8873, 2000. 227. Shukla AK, Manglik A, Kruse AC, Xiao K, Reis RI, Tseng WC, Staus DP, Hilger D, Uysal S, Huang LY, Paduch M, Tripathi-Shukla P, Koide A, Koide S, Weis WI, Kossiakoff AA, Kobilka BK, Lefkowitz RJ. Structure of active beta-arrestin-1 bound to a G-proteincoupled receptor phosphopeptide. Nature 497: 137–141, 2013. 208. Rengo G, Lymperopoulos A, Zincarelli C, Donniacuo M, Soltys S, Rabinowitz JE, Koch WJ. Myocardial adeno-associated virus serotype 6-betaARKct gene therapy improves cardiac function and normalizes the neurohormonal axis in chronic heart failure. Circulation 119: 89 –98, 2009. 228. Shukla AK, Westfield GH, Xiao K, Reis RI, Huang LY, Tripathi-Shukla P, Qian J, Li S, Blanc A, Oleskie AN, Dosey AM, Su M, Liang CR, Gu LL, Shan JM, Chen X, Hanna R, Choi M, Yao XJ, Klink BU, Kahsai AW, Sidhu SS, Koide S, Penczek PA, Kossiakoff AA, Woods VL Jr, Kobilka BK, Skiniotis G, Lefkowitz RJ. Visualization of arrestin recruitment by a G-protein-coupled receptor. Nature 512: 218 –222, 2014. 209. Richardson RM, Kim C, Benovic JL, Hosey MM. Phosphorylation and desensitization of human m2 muscarinic cholinergic receptors by two isoforms of the beta-adrenergic receptor kinase. J Biol Chem 268: 13650 –13656, 1993. 229. Sibley DR, Strasser RH, Caron MG, Lefkowitz RJ. Homologous desensitization of adenylate cyclase is associated with phosphorylation of the beta-adrenergic receptor. J Biol Chem 260: 3883–3886, 1985. 210. Rockman HA, Chien KR, Choi DJ, Iaccarino G, Hunter JJ, Ross J Jr, Lefkowitz RJ, Koch WJ. Expression of a beta-adrenergic receptor kinase 1 inhibitor prevents the development of myocardial failure in gene-targeted mice. Proc Natl Acad Sci USA 95: 7000 –7005, 1998. 230. Sigurdsson A. Neurohormonal activation in patients with acute myocardial infarction or chronic congestive heart failure. With special reference to treatment with angiotensin converting enzyme inhibitors. Blood Press Suppl 1: 1– 45, 1995. 211. Rockman HA, Choi DJ, Akhter SA, Jaber M, Giros B, Lefkowitz RJ, Caron MG, Koch WJ. Control of myocardial contractile function by the level of beta-adrenergic receptor kinase 1 in gene-targeted mice. J Biol Chem 273: 18180 –18184, 1998. 231. Somers RL, Klein DC. Rhodopsin kinase activity in the mammalian pineal gland and other tissues. Science 226: 182–184, 1984. 212. Rockman HA, Choi DJ, Rahman NU, Akhter SA, Lefkowitz RJ, Koch WJ. Receptorspecific in vivo desensitization by the G protein-coupled receptor kinase-5 in transgenic mice. Proc Natl Acad Sci USA 93: 9954 –9959, 1996. 213. Rockman HA, Koch WJ, Lefkowitz RJ. Seven-transmembrane-spanning receptors and heart function. Nature 415: 206 –212, 2002. 214. Rosenbaum DM, Cherezov V, Hanson MA, Rasmussen SG, Thian FS, Kobilka TS, Choi HJ, Yao XJ, Weis WI, Stevens RC, Kobilka BK. GPCR engineering yields high-resolution structural insights into beta2-adrenergic receptor function. Science 318: 1266 –1273, 2007. 215. Sallese M, Iacovelli L, Cumashi A, Capobianco L, Cuomo L, De Blasi A. Regulation of G protein-coupled receptor kinase subtypes by calcium sensor proteins. Biochim Biophys Acta 1498: 112–121, 2000. 216. Sallese M, Lombardi MS, De Blasi A. Two isoforms of G protein-coupled receptor kinase 4 identified by molecular cloning. Biochem Biophys Res Commun 199: 848 – 854, 1994. 217. Sallese M, Salvatore L, D’Urbano E, Sala G, Storto M, Launey T, Nicoletti F, Knopfel T, De Blasi A. The G-protein-coupled receptor kinase GRK4 mediates homologous desensitization of metabotropic glutamate receptor 1. FASEB J 14: 2569 –2580, 2000. 218. Santulli G, Campanile A, Spinelli L, Assante di Panzillo E, Ciccarelli M, Trimarco B, Iaccarino G. G protein-coupled receptor kinase 2 in patients with acute myocardial infarction. Am J Cardiol 107: 1125–1130, 2011. 219. Schulz R, Wehmeyer A, Schulz K. Visualizing preference of G protein-coupled receptor kinase 3 for the process of kappa-opioid receptor sequestration. Mol Pharmacol 61: 1444 –1452, 2002. 220. Sefton M, Blanco MJ, Penela P, Mayor F, Nieto MA. Expression of the G protein-coupled receptor kinase 2 during early mouse embryogenesis. Mech Dev 98: 127–131, 2000. 221. Shah AS, White DC, Emani S, Kypson AP, Lilly RE, Wilson K, Glower DD, Lefkowitz RJ, Koch WJ. In vivo ventricular gene delivery of a beta-adrenergic receptor kinase inhibitor to the failing heart reverses cardiac dysfunction. Circulation 103: 1311–1316, 2001. 222. Shenoy SK, Drake MT, Nelson CD, Houtz DA, Xiao K, Madabushi S, Reiter E, Premont RT, Lichtarge O, Lefkowitz RJ. Beta-arrestin-dependent, G protein-independent ERK1/2 activation by the beta2 adrenergic receptor. J Biol Chem 281: 1261–1273, 2006. 402 232. Sorriento D, Ciccarelli M, Santulli G, Campanile A, Altobelli GG, Cimini V, Galasso G, Astone D, Piscione F, Pastore L, Trimarco B, Iaccarino G. The G-protein-coupled receptor kinase 5 inhibits NFkappaB transcriptional activity by inducing nuclear accumulation of IkappaB alpha. Proc Natl Acad Sci USA 105: 17818 –17823, 2008. 233. Sorriento D, Santulli G, Fusco A, Anastasio A, Trimarco B, Iaccarino G. Intracardiac injection of AdGRK5-NT reduces left ventricular hypertrophy by inhibiting NF-kappaB-dependent hypertrophic gene expression. Hypertension 56: 696 –704, 2010. 234. Speirs HJ, Katyk K, Kumar NN, Benjafield AV, Wang WY, Morris BJ. Association of G-protein-coupled receptor kinase 4 haplotypes, but not HSD3B1 or PTP1B polymorphisms, with essential hypertension. J Hypertens 22: 931–936, 2004. 235. Spinelli L, Trimarco V, Di Marino S, Marino M, Iaccarino G, Trimarco B. L41Q polymorphism of the G protein coupled receptor kinase 5 is associated with left ventricular apical ballooning syndrome. Eur J Heart Fail 12: 13–16, 2010. 236. Standfuss J, Edwards PC, D’Antona A, Fransen M, Xie G, Oprian DD, Schertler GF. The structural basis of agonist-induced activation in constitutively active rhodopsin. Nature 471: 656 – 660, 2011. 237. Sterne-Marr R, Benovic JL. Regulation of G protein-coupled receptors by receptor kinases and arrestins. Vitam Horm 51: 193–234, 1995. 238. Sterne-Marr R, Leahey PA, Bresee JE, Dickson HM, Ho W, Ragusa MJ, Donnelly RM, Amie SM, Krywy JA, Brookins-Danz ED, Orakwue SC, Carr MJ, Yoshino-Koh K, Li Q, Tesmer JJ. GRK2 activation by receptors: role of the kinase large lobe and carboxylterminal tail. Biochemistry 48: 4285– 4293, 2009. 239. Stevenson NL, Martin-Martin B, Freeman J, Kriston-Vizi J, Ketteler R, Cutler DF. G protein-coupled receptor kinase 2 moderates recruitment of THP-1 cells to the endothelium by limiting histamine-invoked Weibel-Palade body exocytosis. J Thromb Haemost 12: 261–272, 2014. 240. Stoffel RH, Inglese J, Macrae AD, Lefkowitz RJ, Premont RT. Palmitoylation increases the kinase activity of the G protein-coupled receptor kinase, GRK6. Biochemistry 37: 16053–16059, 1998. 241. Stoffel RH, Randall RR, Premont RT, Lefkowitz RJ, Inglese J. Palmitoylation of G protein-coupled receptor kinase, GRK6. Lipid modification diversity in the GRK family. J Biol Chem 269: 27791–27794, 1994. 242. Strasser RH, Benovic JL, Caron MG, Lefkowitz RJ. Beta-agonist- and prostaglandin E1-induced translocation of the beta-adrenergic receptor kinase: evidence that the Physiol Rev • VOL 95 • APRIL 2015 • www.prv.org G PROTEIN-COUPLED RECEPTOR KINASES kinase may act on multiple adenylate cyclase-coupled receptors. Proc Natl Acad Sci USA 83: 6362– 6366, 1986. 243. Strasser RH, Sibley DR, Lefkowitz RJ. A novel catecholamine-activated adenosine cyclic 3=,5=-phosphate independent pathway for beta-adrenergic receptor phosphorylation in wild-type and mutant S49 lymphoma cells: mechanism of homologous desensitization of adenylate cyclase. Biochemistry 25: 1371–1377, 1986. 244. Taguchi K, Kobayashi T, Takenouchi Y, Matsumoto T, Kamata K. Angiotensin II causes endothelial dysfunction via the GRK2/Akt/eNOS pathway in aortas from a murine type 2 diabetic model. Pharmacol Res 64: 535–546, 2011. 245. Taguchi K, Sakata K, Ohashi W, Imaizumi T, Imura J, Hattori Y. Tonic inhibition by G protein-coupled receptor kinase 2 of Akt/endothelial nitric-oxide synthase signaling in human vascular endothelial cells under conditions of hyperglycemia with high insulin levels. J Pharmacol Exp Ther 349: 199 –208, 2014. 246. Taneja M, Salim S, Saha K, Happe HK, Qutna N, Petty F, Bylund DB, Eikenburg DC. Differential effects of inescapable stress on locus coeruleus GRK3, alpha2-adrenoceptor and CRF1 receptor levels in learned helpless and non-helpless rats: a potential link to stress resilience. Behav Brain Res 221: 25–33, 2011. 247. Tarantino P, De Marco EV, Annesi G, Rocca FE, Annesi F, Civitelli D, Provenzano G, Scornaienchi V, Greco V, Colica C, Nicoletti G, Quattrone A. Lack of association between G-protein coupled receptor kinase 5 gene and Parkinson’s disease. Am J Med Genet B Neuropsychiatr Genet 156B: 104 –107, 2011. 248. Tevaearai HT, Eckhart AD, Shotwell KF, Wilson K, Koch WJ. Ventricular dysfunction after cardioplegic arrest is improved after myocardial gene transfer of a beta-adrenergic receptor kinase inhibitor. Circulation 104: 2069 –2074, 2001. 249. Thal DM, Homan KT, Chen J, Wu EK, Hinkle PM, Huang ZM, Chuprun JK, Song J, Gao E, Cheung JY, Sklar LA, Koch WJ, Tesmer JJ. Paroxetine is a direct inhibitor of G protein-coupled receptor kinase 2 and increases myocardial contractility. ACS Chem Biol 7: 1830 –1839, 2012. 250. Theilade J, Strom C, Christiansen T, Haunso S, Sheikh SP. Differential G protein receptor kinase 2 expression in compensated hypertrophy and heart failure after myocardial infarction in the rat. Basic Res Cardiol 98: 97–103, 2003. 251. Thiyagarajan MM, Stracquatanio RP, Pronin AN, Evanko DS, Benovic JL, Wedegaertner PB. A predicted amphipathic helix mediates plasma membrane localization of GRK5. J Biol Chem 279: 17989 –17995, 2004. 252. Tilley DG, Kim IM, Patel PA, Violin JD, Rockman HA. beta-Arrestin mediates beta1adrenergic receptor-epidermal growth factor receptor interaction and downstream signaling. J Biol Chem 284: 20375–20386, 2009. 253. Ungerer M, Bohm M, Elce JS, Erdmann E, Lohse MJ. Altered expression of betaadrenergic receptor kinase and beta 1-adrenergic receptors in the failing human heart. Circulation 87: 454 – 463, 1993. 254. Usui I, Imamura T, Satoh H, Huang J, Babendure JL, Hupfeld CJ, Olefsky JM. GRK2 is an endogenous protein inhibitor of the insulin signaling pathway for glucose transport stimulation. EMBO J 23: 2821–2829, 2004. 255. Valanne S, Myllymaki H, Kallio J, Schmid MR, Kleino A, Murumagi A, Airaksinen L, Kotipelto T, Kaustio M, Ulvila J, Esfahani SS, Engstrom Y, Silvennoinen O, Hultmark D, Parikka M, Ramet M. Genome-wide RNA interference in Drosophila cells identifies G protein-coupled receptor kinase 2 as a conserved regulator of NF-kappaB signaling. J Immunol 184: 6188 – 6198, 2010. 259. Vinge LE, Oie E, Andersson Y, Grogaard HK, Andersen G, Attramadal H. Myocardial distribution and regulation of GRK and beta-arrestin isoforms in congestive heart failure in rats. Am J Physiol Heart Circ Physiol 281: H2490 –H2499, 2001. 260. Vinge LE, Raake PW, Koch WJ. Gene therapy in heart failure. Circ Res 102: 1458 – 1470, 2008. 261. Vinge LE, von Lueder TG, Aasum E, Qvigstad E, Gravning JA, How OJ, Edvardsen T, Bjornerheim R, Ahmed MS, Mikkelsen BW, Oie E, Attramadal T, Skomedal T, Smiseth OA, Koch WJ, Larsen TS, Attramadal H. Cardiac-restricted expression of the carboxyl-terminal fragment of GRK3 uncovers distinct functions of GRK3 in regulation of cardiac contractility and growth: GRK3 controls cardiac alpha1-adrenergic receptor responsiveness. J Biol Chem 283: 10601–10610, 2008. 262. Voigt C, Holzapfel HP, Meyer S, Paschke R. Increased expression of G-proteincoupled receptor kinases 3 and 4 in hyperfunctioning thyroid nodules. J Endocrinol 182: 173–182, 2004. 263. Volkers M, Weidenhammer C, Herzog N, Qiu G, Spaich K, von Wegner F, Peppel K, Muller OJ, Schinkel S, Rabinowitz JE, Hippe HJ, Brinks H, Katus HA, Koch WJ, Eckhart AD, Friedrich O, Most P. The inotropic peptide betaARKct improves betaAR responsiveness in normal and failing cardiomyocytes through G(betagamma)-mediated Ltype calcium current disinhibition. Circ Res 108: 27–39, 2011. 264. Von Lueder TG, Gravning J, How OJ, Vinge LE, Ahmed MS, Krobert KA, Levy FO, Larsen TS, Smiseth OA, Aasum E, Attramadal H. Cardiomyocyte-restricted inhibition of G protein-coupled receptor kinase-3 attenuates cardiac dysfunction after chronic pressure overload. Am J Physiol Heart Circ Physiol 303: H66 –H74, 2012. 265. Vroon A, Kavelaars A, Limmroth V, Lombardi MS, Goebel MU, Van Dam AM, Caron MG, Schedlowski M, Heijnen CJ. G protein-coupled receptor kinase 2 in multiple sclerosis and experimental autoimmune encephalomyelitis. J Immunol 174: 4400 – 4406, 2005. 266. Wang WC, Mihlbachler KA, Bleecker ER, Weiss ST, Liggett SB. A polymorphism of G-protein coupled receptor kinase5 alters agonist-promoted desensitization of beta2-adrenergic receptors. Pharmacogenet Genomics 18: 729 –732, 2008. 267. Wang Y, Li B, Zhao W, Liu P, Zhao Q, Chen S, Li H, Gu D. Association study of G protein-coupled receptor kinase 4 gene variants with essential hypertension in northern Han Chinese. Ann Hum Genet 70: 778 –783, 2006. 268. Wang Z, Armando I, Asico LD, Escano C, Wang X, Lu Q, Felder RA, Schnackenberg CG, Sibley DR, Eisner GM, Jose PA. The elevated blood pressure of human GRK4gamma A142V transgenic mice is not associated with increased ROS production. Am J Physiol Heart Circ Physiol 292: H2083–H2092, 2007. 269. Weiss ER, Raman D, Shirakawa S, Ducceschi MH, Bertram PT, Wong F, Kraft TW, Osawa S. The cloning of GRK7, a candidate cone opsin kinase, from cone- and rod-dominant mammalian retinas. Mol Vis 4: 27, 1998. 270. Weller M, Virmaux N, Mandel P. Light-stimulated phosphorylation of rhodopsin in the retina: the presence of a protein kinase that is specific for photobleached rhodopsin. Proc Natl Acad Sci USA 72: 381–385, 1975. 271. Whalen EJ, Foster MW, Matsumoto A, Ozawa K, Violin JD, Que LG, Nelson CD, Benhar M, Keys JR, Rockman HA, Koch WJ, Daaka Y, Lefkowitz RJ, Stamler JS. Regulation of beta-adrenergic receptor signaling by S-nitrosylation of G-protein-coupled receptor kinase 2. Cell 129: 511–522, 2007. 272. Whitcomb T, Sakurai K, Brown BM, Young JE, Sheflin L, Dlugos C, Craft CM, Kefalov VJ, Khani SC. Effect of G protein-coupled receptor kinase 1 (Grk1) overexpression on rod photoreceptor cell viability. Invest Ophthalmol Vis Sci 51: 1728 –1737, 2010. 256. Vandell AG, Lobmeyer MT, Gawronski BE, Langaee TY, Gong Y, Gums JG, Beitelshees AL, Turner ST, Chapman AB, Cooper-DeHoff RM, Bailey KR, Boerwinkle E, Pepine CJ, Liggett SB, Johnson JA. G protein receptor kinase 4 polymorphisms: betablocker pharmacogenetics and treatment-related outcomes in hypertension. Hypertension 60: 957–964, 2012. 273. White DC, Hata JA, Shah AS, Glower DD, Lefkowitz RJ, Koch WJ. Preservation of myocardial beta-adrenergic receptor signaling delays the development of heart failure after myocardial infarction. Proc Natl Acad Sci USA 97: 5428 –5433, 2000. 257. Vatter P, Stoesser C, Samel I, Gierschik P, Moepps B. The variable C-terminal extension of G-protein-coupled receptor kinase 6 constitutes an accessorial autoregulatory domain. FEBS J 272: 6039 – 6051, 2005. 274. Wilden U. Duration and amplitude of the light-induced cGMP hydrolysis in vertebrate photoreceptors are regulated by multiple phosphorylation of rhodopsin and by arrestin binding. Biochemistry 34: 1446 –1454, 1995. 258. Villar VA, Jones JE, Armando I, Palmes-Saloma C, Yu P, Pascua AM, Keever L, Arnaldo FB, Wang Z, Luo Y, Felder RA, Jose PA. G protein-coupled receptor kinase 4 (GRK4) regulates the phosphorylation and function of the dopamine D3 receptor. J Biol Chem 284: 21425–21434, 2009. 275. Williams SM, Ritchie MD, Phillips JA, 3rd Dawson E, Prince M, Dzhura E, Willis A, Semenya A, Summar M, White BC, Addy JH, Kpodonu J, Wong LJ, Felder RA, Jose PA, Moore JH. Multilocus analysis of hypertension: a hierarchical approach. Hum Hered 57: 28 –38, 2004. Physiol Rev • VOL 95 • APRIL 2015 • www.prv.org 403 SATO ET AL. 276. Winstel R, Freund S, Krasel C, Hoppe E, Lohse MJ. Protein kinase cross-talk: membrane targeting of the beta-adrenergic receptor kinase by protein kinase C. Proc Natl Acad Sci USA 93: 2105–2109, 1996. 281. Yi XP, Zhou J, Baker J, Wang X, Gerdes AM, Li F. Myocardial expression and redistribution of GRKs in hypertensive hypertrophy and failure. Anat Rec A Discov Mol Cell Evol Biol 282: 13–23, 2005. 277. Wisler JW, DeWire SM, Whalen EJ, Violin JD, Drake MT, Ahn S, Shenoy SK, Lefkowitz RJ. A unique mechanism of beta-blocker action: carvedilol stimulates beta-arrestin signaling. Proc Natl Acad Sci USA 104: 16657–16662, 2007. 282. Zhang Y, Matkovich SJ, Duan X, Gold JI, Koch WJ, Dorn GW 2nd. Nuclear effects of G-protein receptor kinase 5 on histone deacetylase 5-regulated gene transcription in heart failure. Circ Heart Fail 4: 659 – 668, 2011. 278. Xia Z, Yang T, Wang Z, Dong J, Liang C. GRK5 intronic (CA)n polymorphisms associated with type 2 diabetes in Chinese Hainan Island. PLoS One 9: e90597, 2014. 283. Zhao X, Haeseleer F, Fariss RN, Huang J, Baehr W, Milam AH, Palczewski K. Molecular cloning and localization of rhodopsin kinase in the mammalian pineal. Vis Neurosci 14: 225–232, 1997. 279. Xing W, Li Y, Zhang H, Mi C, Hou Z, Quon MJ, Gao F. Improvement of vascular insulin sensitivity by downregulation of GRK2 mediates exercise-induced alleviation of hypertension in spontaneously hypertensive rats. Am J Physiol Heart Circ Physiol 305: H1111–H1119, 2013. 280. Yarfitz S, Hurley JB. Transduction mechanisms of vertebrate and invertebrate photoreceptors. J Biol Chem 269: 14329 –14332, 1994. 404 284. Zhao X, Yokoyama K, Whitten ME, Huang J, Gelb MH, Palczewski K. A novel form of rhodopsin kinase from chicken retina and pineal gland. FEBS Lett 454: 115–121, 1999. 285. Zidar DA, Violin JD, Whalen EJ, Lefkowitz RJ. Selective engagement of G protein coupled receptor kinases (GRKs) encodes distinct functions of biased ligands. Proc Natl Acad Sci USA 106: 9649 –9654, 2009. Physiol Rev • VOL 95 • APRIL 2015 • www.prv.org
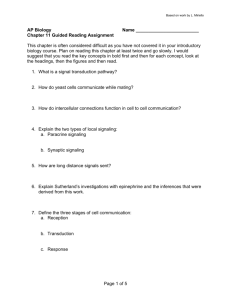
![Anti-VEGF Receptor 1 antibody [AP-MAB0702] ab56300 Product datasheet 2 References Overview](http://s2.studylib.net/store/data/012124206_1-d32314b990f15ec4dec65dd038b8f15c-300x300.png)



![Anti-VEGF Receptor 3 antibody [AFL4] (Biotin) ab93529](http://s2.studylib.net/store/data/012128850_1-8f9f7cd32e3d7603face275ba471b332-300x300.png)

