Modelling transmission dynamics and the impact of Modelling transmission dynamics and the impact of diff
advertisement

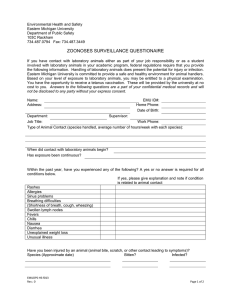
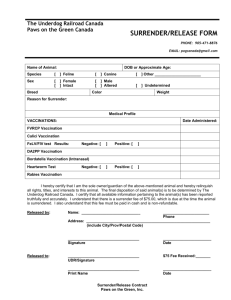
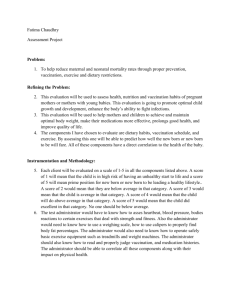
Modelling transmission dynamics and the impact of Modelling transmission dynamics and the impact of diff different vaccination strategies on Respiratory i i gi pi y Syncytial Virus associated hospitalizations Syncytial Virus associated hospitalizations Kinyanjui T.M1*, Munywoki P.K1, Kiti M.C1, Cane P.A2, Medley G.F3, Nokes D.J1,3 1 Centre for Geographic Medicine Research‐Coast, Kenya Medical Research Institute, Kenya Centre for Geographic Medicine Research‐Coast Kenya Medical Research Institute Kenya 2 Health Protection Agency, London, UK Health Protection Agency London UK 3 School of Life Sciences, University of Warwick, Coventry, UK School of Life Sciences, University of Warwick, Coventry, UK * Address correspondence to, Email: tkinyanjui@kilifi.kemri-wellcome.org (TABLE 1) VACCINATION STRATEGIES RATIONALE DISCUSSION • Model M d l with heterogeneous ith h t mixing assumption captures the age specific profile of hospital cases with RMSD 7.54 vs 14.61 for homogeneous assumption. • There is merit in delaying age at vaccination i i to 4 months h if protective MatAbs last for a month Benefit is reduced month. beyond y 4 months of age g at vaccination. •For the model assuming h heterogeneous mixing, i i the h benefit of vaccination appears to be greater and this may be attributed a bu ed to o sstronger o ge indirect d ec benefit of vaccination arising from the nature of the contacts in the population. • RSV has been identified as an iimportant t th human pathogen th majority of severe disease occurring in developing countries ((Nair et al.,, 2010)) • Severe disease associated with p primary/early y y infection 1-3 months key age group (H d l 1979 (Henderson ett al., 1979, Gl Glezen ett al., 1986) AGE STRUCTURED MODEL • No vaccine available for this target g g group. p Immunogenicity g y vs safety (Karron et al., 2005) • Explore p vaccine effectiveness outside key target group => use mathematical modelling 2 Contin o s Ageing Continuous OBJECTIVES •Model M d l th the ttransmission i i d namics of RSV using dynamics sing a Realistic Age Structured (RAS) model WORK TO BE COMPLETED • Complete estimating the epi epiparameters: WAIFW matrix1 (Nokes DJ., 2008 CID, proposed contact study in Kilifi) WAIFW – β(a,a’): Who Acquires Infection F From Wh Whom matrix. t i This Thi matrix t i describes d ib the probability that an infectious person in age class a will infect a susceptible person in age p g class a’. 1 •Estimate E i d demographic hi and d epidemiological id i l i l parameters t – e g WAIFW1 e.g. •Conduct a sensitivity analysis on the least certain parameters The basic reproductive p number,, R0, is defined as the average number of secondary infections produced when one infected individual is introduced into a host population where everyone is susceptible 2 •Investigate the impact of different vaccination strategies on iincidence id off severe LRTI (see Table 1) n bij (α 0 , j I 0 , j + α 1, j I1, j + α 2 , j I 2 , j ) j =1 Ni λi = ∑ •Complete the implementation of the vaccination strategies • Investigate the role of household structure t t on infection i f ti dynamics d i using a household stochastic model •Discrete age classes are considered •Ageing is continuous •Infection disease are dependent I f ti and d di d d t on a) Age b) Number of previous infections •Develop D l an individual-based i di id l b d stochastic t h ti model d l tto study t d household transmission ACKNOWLEDGMENTS Warwick University Thomas House Sam Mason Wellcome Trust support: Grant Ref No. 084633 PRELIMINARY RESULTS 5 10 15 Age classes 20 25 Fig 1 shows a model fit to age specific RSV hospitalisation data from Kilifi District Hospital (KDH), Kenya, in children aged 0 to 5 years with a) a homogeneous and b) a heterogeneous mixing assumption dynamic models. References 0.2 0.4 0.6 Vaccination coverage 0.7 0.8 Fig 2 shows the proportion reduction in the number of hospitalised cases cumulatively over four years as a function of the vaccination coverage and the month at vaccination. There is benefit in delaying vaccination up to 4 months th but b t reduced d d benefit b fit iin waiting iti longer l than th 4 months th for higher vaccination coverage. 0 .7 0 .8 0 .9 8 7 0. 0 .9 0 .9 0 .8 0 .7 Ti Time series i off model d l prediction di ti ffor effect ff t off vaccination i ti Model data KDH data 70 No o of hos spitalizzations s per m onth 0 .6 0. 6 0. 0. 0 0 .6 0 .5 0.2 0..1 0 .4 6 60 50 40 30 20 10 2 1 0 .4 0 .3 8 0.8 8 0 .6 0 .2 0 .1 10 4 0.9 0 .8 0 .5 0 .4 5 1 0 12 0 .3 0 .9 2 0.2 0.1 0.3 0 .7 0 .6 5 2 0 0 3 0. 80 14 Mon nth at vaccin v ation 0 .8 0 .7 0 .6 0 .5 6 3 20 0 .4 7 4 40 0 .3 8 0 .2 0 .1 9 0.5 60 10 0. 4 80 0 .1 8 0. 0 .9 12 Mon nth at vaccin v ation 100 R l ti reduction d ti in i h it li d cases - H t i i Relative hospitalised Heterogeneous mixing 16 11 120 18 7 0. 0. 5 0 .4 0 .3 0 .2 13 140 N o of in ndividu uals 0 .1 KDH data Homogeneous model Heterogeneous model 160 Relative reduction in hospitalised cases - Homogeneous mixing 14 0 .2 A di Age distribution t ib ti off h hospitalised it li d cases with ith model d l fits fit 180 KEMRI/Wellcome Unit Alex e Maina a a - Librarian ba a RSV team 0.2 0 0 .8 0 . 5 0. 6 . 7 0.4 0.6 Vaccination coverage g 0.9 0.8 Fig 3 shows the proportion reduction in the number of hospitalised cases cumulatively over 4 years as a function of the vaccination coverage and the month at vaccination. There is benefit in delaying vaccination with greater benefit compared d to t homogeneous h model d l and d may be b attributed tt ib t d to t stronger indirect effects. 1 0 2004 2006 2008 2010 2012 2014 Year 2016 2018 2020 2022 Fig 4 shows Fi h the th h homogeneous model d l fit to t KDH d data t ffrom Nov2004 to Aug2010. Maximum likelihood method was used to fit the model to data assuming a Poisson distribution distribution. The fitted values are: bij = 3.1, amplitude (a) = 0.183 and seasonal offset value (p) = 0.182. Vaccination is introduced in Feb 2012 at 70% coverage at 4 months. Note the honeymoon period of about 2 years and the subsequent y q change g in the epidemiology p gy of RSV after the introduction of a vaccine. Vaccine is assumed to elicit an immune response equivalent to a natural infection. Nair H et al. (2010) Global burden of acute lower respiratory infections due to respiratory syncytial virus in young children: a systematic review and meta-analysis. Lancet 375: 1545-1555. Henderson FW et al (1979) (19 9) Respiratory-syncytial-virus infections, f reinfections f and immunity. A prospective, longitudinal study in young children. N Engl J Med 300: 300 530-534. 30 3 Glezen W et al(1986) Risk of primary infection and reinfection with respiratory syncytial virus. American Journal of Diseases of Children 140: 543-546. Karron RA et al. (2005) Identification of a recombinant live attenuated respiratory syncytial virus vaccine candidate that is highly attenuated in infants. J Infect Dis 191: 1093-1104. Nokes DJ et al. (2008) ( ) Respiratory p y syncytial y y virus infection and disease in infants and young y g children observed from birth in Kilifi District,, Kenya. y Clin Infect Dis 46: 50-57.