Pharmacist Intervention in a Heart Failure Clinic
advertisement

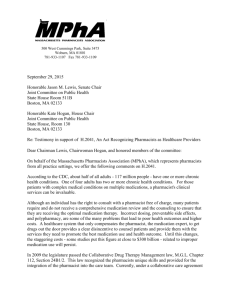
Pharmacist Intervention in a Heart Failure Clinic Marie Claire Aquilina, Lilian M. Azzopardi, Anthony Serracino-Inglott Department of Pharmacy, Faculty of Medicine and Surgery, University of Malta, Msida Malta University of Malta E-mail: maqu0012@um.edu.mt Introduction Aim Heart failure (HF) patients usually require polypharmacy to manage their condi- To introduce and evaluate the pharmacist’s intervention in HF care within a tion including medication such as angiotensin-converting enzyme inhibitors, clinical environment. and diuretics, as well as medication to treat concurrent disease. Pharmacists Setting can benefit HF patient care actively by collaborating with other professionals Heart Failure Clinic (HFC) at Mater Dei Hospital (MDH) in Malta which is a nurse 1 and supportively by helping patients with their medication . -driven clinic with cardiologists available as required. Questionnaire Sections Method Questionnaire compiled Minnesota Living with Heart Fail2 ure Questionnaire® (MLHFQ) to assess quality of life (QoL) Lifestyle Management of HF Psychometric testing of the questionnaire (validity and reliability) Microsoft® Excel and SPSS v.17® (Wilcoxon Signed Ranks Test) and to assess for significant changes in responses to questions from week 0 to 6 50 patients recruited by convenience sampling Pharmacist Intervention Adherence Data Analysis Ethical approval obtained from University Research Ethics Committee of University of Malta 2nd interview (Week 6) Questionnaire readministered to patients Further queries discussed with patient 6 weeks later 1st interview (Week 0) Preparation of individual patient treatment chart Patient advice concerning management of condition, lifestyle, importance of self-care and of adherence Answered queries regarding medication discussed Encouraged patients to contact HFC if problems arise Patients completed the questionnaire Investigator compiled a medical history form on each patient. Results ADHERENCE DEMOGRAPHICAL DATA (n=50): There was a significant increase from n = 32 (week 0) to n = 47 (week 6) in the Gender: 42 male, 8 female Age: 43—83 years (mean age = 65.36) number of patients who felt the treatment chart was always useful (p<0.001). There was also a significant increase in patients who improved adherence due to not forgetting doses and expense of medicines (Table 1). QUALITY OF LIFE Patient did not take medicine due to Week Forgetting Expenses A significantly improved QoL at week 6 was observed since the lower the MLHFQ score the greater the QoL (p=0.001) (Figure 1). LIFESTYLE Always 0 0 0 6 0 0 Often 0 1 0 6 0 0 Sometimes 0 14 3 6 6 1 Rarely 0 25 7 6 31 2 Never 0 10 40 6 13 47 P-value 0.038 0.038 Figure 1: Mean MLHFQ scores obtained Table 1: Patients’ responses concerning adherence which showed significance from week 0 to 6 (n=50) Conclusion A significant improvement was noted in daily self-monitoring of weight where The pharmacist’s participation at the HFC contributed to improving patients’ patients who self-monitored their weight increased from n = 31 (week 0) to n = QoL. An increase in patients who would refer to a pharmacist signifies in- 43 (week 6) (p=0.008). creased confidence in the pharmacist’s professional opinion. Patients benefitted from the pharmacist-prepared treatment charts which also included written MANAGEMENT OF HF advice. The pharmacist intervention enabled them to understand the impor- The majority of patients refer to heart specialists, family doctors, and HFC tance of adherence despite certain issues, which they felt prevented them from nurses when obtaining information about or experiencing problems with medi- following their dosage regimen. In conclusion, the pharmacist intervention at cines. An insignificant increase from n = 8 (week 0) to n = 13 (week 6), was ob- the HFC was positively evaluated and demonstrated the pharmacist’s potential served in those referring to pharmacists. The patients who would refer to a in improving patient care in such a setting. pharmacist before taking medicines not taken on a regular basis, significantly References increased from n = 22 (week 0) to n = 41 (week 6) (p<0.001). [1] Murray M. Implementing pharmacy practice research programs for the management of heart failure. Pharm World Sci 2010;32:546-8. [2] University of Minnesota. Minnesota Living with Heart Failure Questionnaire Measures the Effects of Heart Failure and its Treatments on an Individual’s Quality of Life. [Online]. Last modified: June 2010. [Cited Jan 2011]; [1 screen]. Available from: http://www.license.umn.edu/Products/Minnesotata-LivingLiving--WithWith--HeartHeart--FailureFailure--Questionnaire__Z94019.aspx