Introduction Hospital Course
advertisement

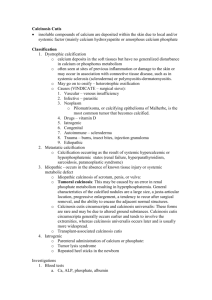
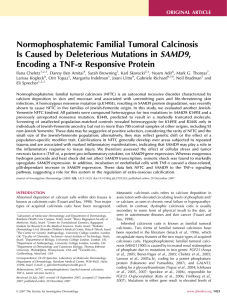
A lump in the elbow—where did all that calcium come from? Arielle Dumas, BS, Mamta Parikh, MD, Jeremy DeMartini, MD, Paul Aronowitz, MD, FACP University of California, Davis Medical Center; Sacramento, CA Introduction Gross Pathology • Tumoral Calcinosis involves the deposition of calcium within periarticular soft tissue forming lobular, radiodense masses. • Patient was restarted on scheduled peritoneal dialysis. • Joint pain was initially treated with NSAIDs and steroids, however, it persisted and radiographs were obtained. • It is a rare, benign condition that is usually familial but in some instances can result from metabolic abnormalities. • The strict definition of tumoral calcinosis requires a hereditary predisposition to the disease and normal calcium levels. However, sporadic or idiopathic occurrences of tumoral calcinosis have also been reported. • On follow up questioning, the patient reported taking high dose calcium acetate while he was in Mexico. Gross images of left hand / right elbow showing nodular deformities at the metacarpal • During hospitalization, calcium acetate was not restarted and his calcium levels normalized. joint and olecranon bursa • Patient was discharged after three weeks with outpatient follow up. Radiology Take Home Points • We present a patient whose kidney failure combined with excessive calcium intake led to tumoral calcinosis. • Tumoral calcinosis, although usually a benign condition, can result in patient discomfort and functional limitations. Case Description • A 62 year old man with a history of chronic kidney disease stage 5, diabetes mellitus, gout and hypertension, presented to the hospital after running out of solution for his chronic peritoneal dialysis. He had lost his insurance after an extended trip to his home country of Mexico, and thus was hospitalized for peritoneal dialysis. On review of systems he complained of mild, chronic right knee pain. Physical Exam • Secondary tumoral calcinosis has been associated with a calcium phosphate product greater than 65-75 with chronic kidney disease, where secondary hyperparathyroidism often coexists. • Our patient had a calcium phosphate product of 89, but did not have secondary hyperparathyroidism. Radiographic imaging of right elbow mass showing lobular calcification • Firm, fixed, non-tender nodule on the right elbow (diameter 2cm) and over the bilateral metacarpal joints. There was mild tenderness over the right olecranon bursa with extreme flexion and extension. References 1. Eisenberg, B., et al., Periarticular tumoral calcinosis and hypercalcemia in a hemodialysis patient without hyperparathyroidism: a case report. J Nucl Med, 1990. 31(6): p. 1099-103. Laboratory Results 2. Lykoudis, E.G., K. Seretis, and S. Ristanis, Huge recurrent tumoral calcinosis needing extensive excision and reconstruction: report of a rare case and brief literature review. Aesthetic Plast Surg, 2012. 36(5): p. 1194-7. • Calcium: 12.0 mg/dL • Phosphate: 7.4 mg/dL • PTHrP: negative • Treatment involves symptomatic management and normalization of phosphate and calcium levels. • With normalization of calcium and phosphate, deposits can gradually decrease in size. • Afebrile, normal vital signs, no apparent distress. • Vitamin D 16 ng/mL Hospital Course Right knee with extensive vascular calcifications 3. Olsen, K.M. and F.S. Chew, Tumoral calcinosis: pearls, polemics, and alternative possibilities. Radiographics, 2006. 26(3): p. 871-85.