Training Programme

Training Programme
Background
Reason for the Trial
NHS Ambulance Service Quality Indicators
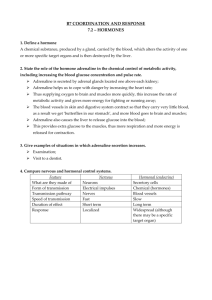
6%
Perkins GD, Cooke MW. Emergency Medical Journal 2011
Adrenaline
20%
Chance of survival
10%
0%
0 5 10 15
Adrenaline doses (mg)
Adrenaline reduces blood supply to the brain
Adrenaline Placebo
Ristagno G. Crit Care Med 2009;37:1408-15
Adrenaline for treatment of cardiac arrest : Clinical data
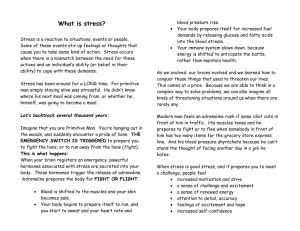
Understanding forest plots
Intervention worse/
Control better
Unity
(no diff)
Intervention better
What does the evidence say?
Likelihood of favourable neurologic outcome following adrenaline
Patanwala AE et al. Minerva Anestesiol. (2013)
Suggests adrenaline reduces the likelihood of favourable neurologic outcome!
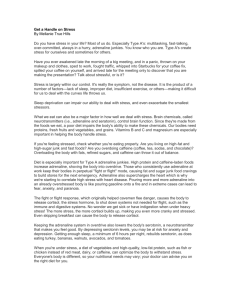
What does the evidence say?
Likelihood of Hospital Admission following adrenaline
Patanwala AE et al. Minerva Anestesiol. (2013)
Suggests adrenaline might increase likelihood of hospital admission,
RCT data favours adrenaline but overall diamond straddles unity!
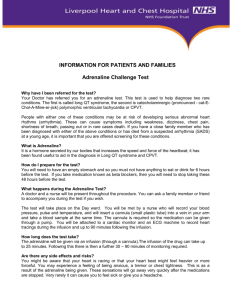
What does the evidence say?
Likelihood of survival to discharge following adrenaline
Patanwala AE et al. Minerva Anestesiol. (2013)
Suggests adrenaline reduces the likelihood of survival to discharge!
Adrenaline for cardiac arrest?
• Higher ROSC rates
• Long term outcome may be worse
• Might be due to suboptimal dose or delivery strategy
• Large placebo-controlled trial essential
300
250
200
150
100
50
0
Assess opinion for the need of a trial
“Overall the risks of IV adrenaline in cardiac arrest outweigh the benefit”: Equipoise!
Public consultation - What outcomes are important?
Risks outweigh benefit
100
80
Short term Heart Long term survival Long term survival without brain damage
60
40
20
0
1 2
Strongly Disagree
3 4 5 6 7
Strongly Agree
180
160
140
120
100
80
60
40
20
0
There is a need for a large RCT of standard dose adrenaline
”
Need for trial
1
Strongly
2 3 4 5 6 7
Strongly
Disagree Agree
140
120
100
80
60
40
20
0
What should be the comparator in a RCT of adrenaline?
Adrenaline compared with
Placebo Adrenaline / beta blocker
Low dose adrenaline
Adrenaline given as a continuous infusion
Consensus on Science
Deakin C et al ILCOR COSTR Resuscitation 2010
Trial is supported by national bodies
Trial Management
Trial Management
• Collaboration between Universities of Warwick and Surrey, and 5
NHS ambulance services.
• Funded by National Institute for Health Research HTA £2.7m
• Sponsored by University of Warwick
• Managed by Warwick Clinical Trials Unit
• Project started 1 st March 2014, due to end 31 st Aug 2018 (includes, set up, pilot, recruitment follow up analysis)
• Supported by: Resuscitation Council UK & ILCOR
• Co-Investigators: Professor Tom Quinn, Professor Charles Deakin, Dr
Jerry Nolan, Professor Judith Finn, Professor Ian Jacobs
Oversight:
• Data will be reviewed for safety (by Data Monitoring Committee)
• Annual review by: Trial Steering Committee, Research Ethics
Committee, funder
Key Points
• Recruitment target 8,000 patients in OHCA
• 5 ambulance services involved (WMAS, LAS,
WAST, NEAS, SCAS)
• Individual patient randomisation
• Outcomes we will measure:
– Survival to hospital, discharge, 30d, 3m, 6m, 12m
– Neurological status
– Quality of life
Ethical and Legal Aspects
Ethical and Legal aspects
• Approval for this trial has been granted by
South Central Oxford C Ethics Committee
(NRES)
• Consent issues addressed for this trial in the emergency setting (see next slide)
• MHRA approval in place
• Legal duty for the trial team to “Contact patient as soon as practicably possible”
Consent in an Emergency Situation
Which Patients do you include in the trial?
• Inclusion Criteria:
– Cardiac arrest in out of hospital environment
– Advanced life support attempted (i.e. you would normally give adrenaline
• Exclusion criteria :
– Known or apparent pregnancy
– Known or apparently aged under 16 years
– Cardiac arrest secondary to anaphylaxis
– Adrenaline given prior to arrival of ambulance service clinician trained in the trial (i.e. you)
Respecting Patient Wishes
(not to participate)
• Same method used by ROC (Resuscitation Outcomes
Consortium) in US & Canada:
– Staff attending a cardiac arrest should look for this bracelet
Good Clinical Practice (GCP)
Principles
Why we need Good Clinical Practice in Research
Good Clinical Practice (GCP) is an international ethical and scientific quality standard for designing, conducting, recording and reporting trials that involve the participation of human subjects.
What is the significance of standards in clinical research?
• Safeguard and protect research subjects
• Risk reduction
• Quality data/ outcomes
• Excellent research, good science
All research carried out today is carried out by conduct underpinned by the Declaration of Helsinki.
Why we need Good Clinical Practice in Research
UK Regs
SI 2984
UK Regs
SI 1928
EU Directive
UK Regs
SI 1031
(Clinical Trials Directive)
ICH GCP
2001
2004
2006
2005
EU Directive
(GCP)
Thalidomide 1997
1964 Declaration of Helsinki
Cough Syrup
Disaster!
1940’s
1960’s
Wartime atrocities
1938
1906 Pure Food and Drug Act (US)
Declaration of Helsinki
(World Medical Organisation)
• Recommendation for physicians in research involving human subjects
• The most commonly recognised & cited research guidance world wide.
• The interests/health/welfare of the patient are paramount
• Privacy of subject is essential
• Consent obtained for all patients (NB UK regulations on emergency research apply for the PARAMEDIC-2 trial)
• Refusal does NOT Impact Patient/clinician relationship (voluntary participation)
• Should be assured of best care/treatment
• Clinical Research requires:
Documented Protocol
Benefits vs risk
Approval independently of researchers
Qualified personnel involved
Data to be published
The 13 Principles of GCP…
Good clinical practise is the standard that all trials MUST follow to ensure the rights, safety and well being of trial participants and to ensure accurate and valid data is collected to produce research of the highest quality. GCP is based on the Declaration of Helsinki .
1.
Ethical principles
2.
Anticipated benefits justify the risks
3.
Information on trial drug adequate to support the trial
4.
Confidentiality of records
5.
Systems + procedures to assure quality
6.
Rights, safety & well-being of patients most important and prevail over interests of science and society
7.
Trials must be scientifically sound and described in clear, detailed protocol
8.
Study drugs must used in accordance with the protocol
9.
All involved must be qualified by education, training & experience for relevant tasks
10. Care given to and medical decisions made on behalf of patients are the responsibility of a qualified doctor or dentist
11. Freely given Informed consent [NB UK regulations on emergency research ]
12. All information recorded, handled & stored to ensure accurate reporting, interpretation & verification
13. Compliance to a protocol approved by independent Ethics Committee
Informed Consent – GCP
Data privacy
Maintain rights
Completed
PRIOR to any study related procedures
Time for questions & review
Given signed copy
Approved by Ethics
PATIENT PROTECTION
Clear and
Fully informed including disclosure of safety information and risks
Personal signing and dating
Concise language
Vulnerable
Patients
BUT…
Medicines for Human Use
(UK Regulations)
Amendment (No2)
SI 2006 No 2984
• Effective from 12 th Dec 2006
• Permits emergency treatment of incapacitated adults prior to consent where :
Treatment is required urgently
The nature of the trial requires urgent action
Not possible to obtain consent
Ethics Committee have approved the protocol
This applies to the PARAMEDIC2 Trial
What does this mean for you?
• Follow the trial protocol
– Include the right patients
– Give the assigned drug from the trial pack
– Complete the study documentation
– Report any serious adverse events
– Ask if you are unsure