IFS PRESS RELEASE
advertisement

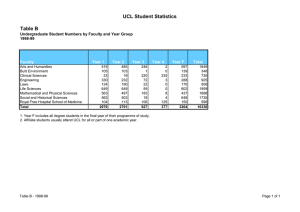
IFS PRESS RELEASE THE INSTITUTE FOR FISCAL STUDIES 7 Ridgmount Street, London WC1E 7AE 020 7291 4800, mailbox@ifs.org.uk, www.ifs.org.uk Middle-aged English healthier than their American counterparts Embargoed until 21.00 Tuesday 2 May 2006 Contacts: Emma Hyman or Bonnie Brimstone, IFS press office on 020 7291 4800 or 07730 667013 Judith Moore, UCL press office, 020 7679 7678, 07917 271364 or 07733 307596 Warren Robak, RAND press office, +1 310 451-6913, robak@rand.org Middle-aged English people are healthier than their American counterparts, according to a collaborative study issued today by English and US researchers. Americans aged between 55 and 64 suffer from diseases such as diabetes, high-blood pressure and lung cancer at rates up to twice those seen among similar aged people in England, reports the study, published on 2 May in the Journal of the American Medical Association. By analysing a large representative sample of people from each country, researchers from the Institute for Fiscal Studies, UCL (University College London) and RAND3 in the US found that English people were less likely to report suffering from a wide array of diseases. The differences were confirmed when researchers analysed separate studies that collected blood samples from participants to look for biological markers of disease – showing that the differences were not just a result of Americans’ increased willingness to report illness. James Smith, of RAND and one of the study’s authors, says: “You don’t expect the health of middle-aged people in these two countries to be too different, but we found that the English are a lot healthier than the Americans. “It’s not just a difference in how people characterise their own health. The biological measures confirm there is a difference.” English people reported better health than their American peers across a range of illnesses. The prevalence of diabetes was nearly twice as high in the United States (12.5 percent) as compared to England (6.1 percent), while high blood pressure was approximately 10 percentage points higher in the US than in England. Heart disease was 50 per cent higher among middle-aged Americans than the English, while the rates of stroke, lung disease and cancer were higher as well. The figure shows the prevalence of heart disease, diabetes and cancer in the two countries across the population divided into three income groups. Prevalence of disease by income group in England and the US 20 Low income Likelihood of disease (%) Medium income High income 15 10 5 0 England US Heart Disease England Diabetes US England US Cancer Reports of poorer health were seen for all socioeconomic groups in the US in comparison to their English peers, not just among the poor. With the exception of cancer, people with lower incomes and educational achievement in both of the nations were more likely to report being ill than those with higher incomes and educational achievement. But, because of the differences between the two nations, those at the top of the education and income scale in the US reported rates of diabetes and heart disease that were similar to those at the bottom of the scale in England. Michael Marmot, of the UCL Department of Epidemiology & Public Health, says: “In the US and England there were remarkably similar socioeconomic differences in health: the less education and income people had, the worse their health. We cannot blame either bad lifestyle or inadequate medical care as the main culprits in these socioeconomic differences in health. We should look for explanation to the circumstances in which people live and work.” The study shows that the differences in health between the two nations are not fully explained by lifestyle factors, such as smoking, drinking, excess weight and poor exercise. Smoking behaviour is similar in the two nations, while excessive drinking of alcohol is more common in England. Obesity is more common in the US, and Americans get less exercise, according to the study. But researchers estimate that those factors together account for less than half of the differences. Nor are the differences accounted for by higher rates of black and Hispanic population in the US, who are groups known to have poorer health, since these are excluded from the study. Researchers say that past differences in health risk factors may be one explanation for the disparities seen in the subjects covered by the study. Rising obesity has occurred in the UK only recently, with the rate increasing from seven per cent in 1980 to 23 percent in 2003. Meanwhile, the prevalence of obesity in the US rose from 16 per cent to 31 per cent during the same period. James Banks, of the UCL Department of Economics and Institute for Fiscal Studies and one of the authors of the study, says: “It may be that England’s shorter history of obesity or differences in childhood experiences create an advantage with respect to middle-aged Americans. But this may mean that over time the gap between England and the United States will begin to close.” The difference in health between middle-aged people in England and the US occurs despite the fact that per person medical spending in the US is more than twice as high as it is in the UK. The two nations also have different health systems, with the UK providing publicly funded health care for all households, while the US has publicly funded health care only for citizens over age 65. The study uses older middle aged members of several large surveys conducted in each nation from 1999 to 2003. In England, the data are drawn from the English Longitudinal Study of Ageing (3,681 people aged 55-64) and the Health Survey for England (5,526 people aged 40-70). For the US, the surveys used were: the Health and Retirement Survey (4,386 people aged 55-64) and the National Health and Nutrition Examination Survey (2,097 people aged 40-70). ENDS Notes to editors: 1. The authors of the study are Professor James Banks, Institute for Fiscal Studies and Department of Economics, University College London; Professor Sir Michael Marmot, International Institute for Society and Health, Department of Epidemiology and Public Health, University College London; Professor James P. Smith, RAND; and Zoë Oldfield, Institute for Fiscal Studies. 2. Michael Marmot is available: Friday 28 April (before midday or after 3pm), and Tuesday 2 May (intermittently). James Banks is available: Thursday 27 April (afternoon), Friday 28 April and Tuesday 2 May (morning). Neither will be contactable over the bank holiday weekend. 3. The research was supported by a grant from the US National Institute of Aging to RAND and the Institute for Fiscal Studies, from the Economic and Social Research Council to IFS and from the MRC to UCL. IFS is an independent institute researching public policy in the UK; RAND corporation is a non-profit research organisation in the US. About UCL: Founded in 1826, UCL was the first English university established after Oxford and Cambridge, the first to admit students regardless of race, class, religion or gender, and the first to provide systematic teaching of law, architecture and medicine. In the government’s most recent Research Assessment Exercise, 59 UCL departments achieved top ratings of 5* and 5, indicating research quality of international excellence. UCL is the fourth-ranked UK university in the 2005 league table of the top 500 world universities produced by the Shanghai Jiao Tong University. UCL alumni include Mahatma Gandhi (Laws 1889, Indian political and spiritual leader); Jonathan Dimbleby (Philosophy 1969, writer and television presenter); Junichiro Koizumi (Economics 1969, Prime Minister of Japan); Lord Woolf (Laws 1954, former Lord Chief Justice of England & Wales); Alexander Graham Bell (Phonetics 1860s, inventor of the telephone); and members of the band Coldplay. 4. Numbers from the figure showing the prevalence of some diseases by income group: Likelihood of disease (%) Low income Medium income High income England 14.3 9.1 6.9 Heart Disease US 20.2 13.1 12.1 England 8.1 7.7 6 Diabetes US 16.8 11.4 9.2 England 5.7 5.1 5.5 Cancer US 9.3 9.8 9.5 Note: Numbers adjusted to take account of differences in drinking, smoking and obesity/overweight Total 10.1 15.1 7.2 12.5 5.4 9.5