AUTHORIZATION AGREEMENT FOR DIRECT DEPOSIT
advertisement

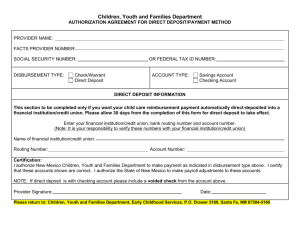
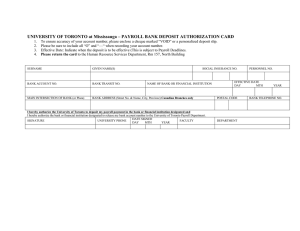
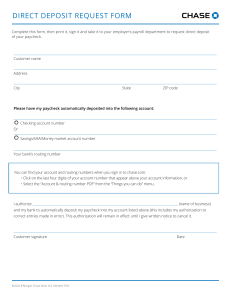
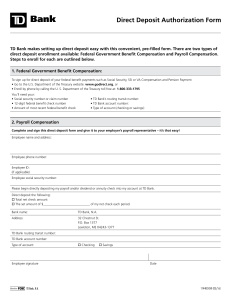
AUTHORIZATION AGREEMENT FOR DIRECT DEPOSIT 1. INSTITUTUION: RSCC ___ 2. Social Security Number: TTCC____ TTCH____ TTCJ____ TTCO____ ___ ___ ___ - ___ ___ - ___ ___ ___ ___ 3. Employee Name: _____________________________________________ 4. Transaction Code: ______ (A=Add C=Change D=Delete) 5. Account Type: CHECKING _____ SAVINGS _____ 6. Name of Financial Institution: ________________________________________________________ 7. CALL FINANCIAL INSTITUTUION TO VERIFY TRANSIT ROUTING (8) AND ACCOUNT NUMBER (9) INFORMATION 8. Transit Routing Number: |: __ __ __ __ __ __ __ __ __ |: 9. Account Number: __ __ __ __ __ __ __ __ __ __ __ __ __ __ __ __ __ __ __ __ __ __ __ __ __ __ I hereby authorize Roane State Community College to deposit my net pay automatically to the account at the financial institution indicated above. I understand this agreement may be terminated by me at any time upon proper execution of another authorized agreement. Employee Signature Original – Payroll Office PA-004 Revised 4/99 __________________ Date