Early Supported Discharge for Stroke Referral Form
advertisement

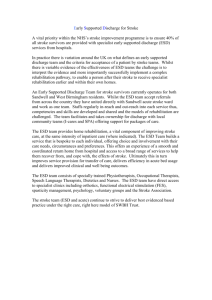
Early Supported Discharge for Stroke Referral Form Patient Name: Hospital no: DOB: Address: GP name: Practice: Address: Phone number(s): Next of Kin: Relationship to the patient: Phone number: Phone number: Other contacts: History of admission and stroke symptoms: Type of stroke: TACI / PACI / POCI / LACI Cause of stroke: Past medical history: Why are you referring to ESD? e.g. Which disciplines will be required to provide input? Criteria Do the patient and family know you are making this referral to ESD? Confirmed diagnosis of new stroke Is the patient medically fit to go home? Is the patient continent? Yes No Comments CT result and date: Predicted discharge date: Please send a medical discharge summary at point of discharge. Buff notes must be returned to the JR Stroke Unit – ESD Office immediately on discharge. If no, how is it managed? Is the patient managing eating and/or drinking? Specify any modified diet or interventions: MUST Score: Date: If >2 please send a copy of the latest MUST score with this referral. Does the patient have any difficulties with communication? Please state specific problems here: Is the patient able to manage their own medications? Are there any other nursing needs? e.g. pressure sores Does the patient live alone? Do they have anyone that can support with shopping, laundry, cooking and cleaning etc? Please send a Speech and Language discharge summary if follow-up is required. Specify if any system required? Please specify: If no, specify who with? Criteria Yes No Does the patient require care visits? Did they have any preadmission social support? Have you noticed any concerns regarding the patient’s cognition, perception or memory? Has the patient been screened or assessed for mood disorders? Has a home assessment been completed? Comments Details of support required: Date care requested: If yes, briefly specify what help they had, who provided it and when. If yes, please send an occupational therapy discharge summary with details of any assessments (including MMSE) If yes, please send a copy of any assessments e.g. Hospital Anxiety and depression Scale (HADS) If yes, give date of OT access/ home visit/ brief summary of outcome or send a copy of the home visit report with this referral. If no, does a visit need to be completed? A member of the ESD team may be able to assist with this visit. Please contact the team to make arrangements. Current mobility: Ability on stairs: Provisional timescale: Goals: Please state at least one goal for each discipline required. Set by the MDT. Outcome measures (e.g.) 9HPT, Berg, TUAG Name of referrer and designation: Telephone Number: Ward: Score: Date: Consultant: Section below for use by ESD team Clinician name/designation: Referral received date/time: Signature: Date of ESD assessment visit if carried out prior to decision: Decision: Accept / Defer / Decline (please circle) Date: Comments: Discussed with the team? If accepted, planned date of admission to ESD: Please EMAIL the completed form and additional information to oxford.esd@nhs.net or FAX to JR Stroke Unit – 01865 851040 Contact ESD team on 01865 221180 (JR Stroke Unit) or 01865 572723 (ESD Office) or Lead Therapist mobile 07717587631 Patient name: DOB: Hospital number: Early Supported Discharge for Stroke Referral Please retain for your records Yes, No or N/A ESD Referral checklist Medical discharge summary sent to ESD team Buff notes returned to JR Stroke Unit, ESD office Speech and Language discharge summary sent FIM paperwork sent MUST Score paperwork sent Occupational therapy home visit report sent Occupational therapy discharge summary sent Physiotherapy discharge summary sent Patient name: DOB: Date referred: Please FAX referral information to: Oxford Stroke Unit – 01865 851040 The ESD team can be contacted on 01865 572723 (ESD Office) or 01865 221180 (JR Stroke Unit) or Lead Therapist mobile 07717587631