Health Care Quality Improvement (QI) Q y p
advertisement
 Q y p")
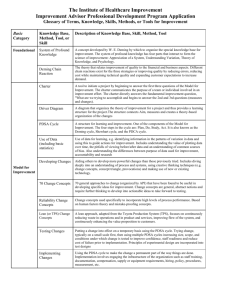
Health Care Q Qualityy Improvement p (QI) (Q ) “A A broad range of activities of varying degrees of complexity and methodological and statistical rigor through which health care providers develop develop, implement, and assess small-scale interventions and identify those that work well and implement them more broadly in order to improve clinical practice.” * The Ethics of Improving Health Care Quality & Safety: A Hastings Center/AHRQ Project, Mary Ann Baily, PhD, Associate for Ethics & Health Policy, The Hastings Center, Garrison, New York, October, 2004 Characteristics of Health Care QI – Contextual factors (background variables or confounders in research) are usually a major focus – The initial intervention (changes to the system) are adapted and modified as study progresses – Measurement is done over time (improvement is temporal) – Graphical analysis and presentation (Statistical Process Control, SPC) – Involvement of local expertise in conducting project – Multiple experimental cycles for rapid feedback and learning Multi-factor factor experiments to learn from complex systems with – Multi non-linear and dynamic cause and effect relationships – Building reliability of the interventions can be a major part of the effort ff – Sustainability is a consideration from the beginning of the project Gold Standard for Building g Evidence Clinical Research: Of all research designs, the randomized controlled trial with adequate numbers of patients, patients blinding of therapists, patients and researchers, and carefully standardized methods of measurement and analysis is the best evidence for cause-effect relationships. Quality Improvement: Satisfactory prediction of the results of tests conducted over a wide range ove ange of conditions. Minimum Standard for Reporting in QI Projects: Annotated Time Series QI Project to Reduce Length of Stay in ED 320 300 Quick-look x-rays Work-up done on floor Bed ahead LOS (minutes) L 280 260 Individual responsible for bed control 240 220 G l Goal 200 180 160 2/16/98 3/16 4/13 Week 5/11 6/8 Time Series Chart vs. Before/After Summary Average of multiple points before and after change 80 90 70 Cycle Time (min.) 100 80 70 60 50 60 50 40 30 20 40 10 30 0 D ec N ov Oct Sep A ug Avg Before Change Jul M ar Feb Jan 0 A pr 10 Jun 20 M ay Change Made date Cyycle Tim e (m in.) Cli i A Clinic Measures of Visit Cycle time (minutes) Avg After Change Time Series Chart vs. Before/After Summary Average of multiple points before and after change Clinic B 80 70 Cycle Time (min.) 100 80 70 60 60 50 40 30 50 20 40 10 30 0 20 Avg Before Change Dec Nov Oct Sep Aug Jul Jun Apr Mar Feb 0 Jan 10 May Change Made date Cyclle Time (m min.) 90 Measures of Visit Cycle time (minutes) Avg After Change Time Series Chart vs. Before/After Summary Average of multiple points before and after change Cli i C Clinic 80 100 70 Cycle Time (min.) 80 70 60 50 60 50 40 30 20 40 10 30 0 20 Avg Before Change Dec Nov Oct Sep Aug Jul Jun Mar Feb Jan 0 Apr 10 May Change Made date Cyccle Time (m min.) 90 Measures of Visit Cycle time (minutes) Avg After Change 100 80 Cycle Tim me (min.) Clinic A 70 60 50 40 30 Dec Nov Oct Sep Aug Jul May Apr Mar Jan 0 Feb 10 Jun Change Made 20 date Time Series Ch t vs. Chart Before/After Summary 90 100 90 60 50 40 30 20 Dec Nov Oct Sep Aug Jul May Apr Feb Jan Mar 60 date 0 Jun Change Made 10 70 100 50 90 40 30 20 Dec Nov Apr Mar 0 Feb Avg After Change Jan Avg Before Change Oct Change Made 10 Sep 0 50 Aug 10 60 Jul 20 Clinic B 70 Jun 30 80 May 35 40 Cycle Tim me (min.) C y cle T im e (m iin .) 70 Clinic U itB2 Unit 70 date 80 Cycle Time (min C n.) Cycle Time Results for Clinics A, B, C 80 The Foundation of the Science of Improvement: D i ’ S Deming’s System t off P Profound f dK Knowledge l d Appreciation of a system Theory of Knowledge g y gy Psychology Understanding Variation “The aim “Th i off this hi chapter h is i to provide id an outside id view i – a lens l – that h I call ll a system off profound Knowledge. It provides a map of theory by which to understand the organizations that we work in.” The Science of Improvement: Increased capability to make improvements Subject Matter Knowledge Learn to combine subject matter knowledge and profound knowledge in creative ways to develop effective changes for improvement Appreciation off a System S t Increased capability to Make Improvements Profound Knowledge Theory of Knowledge Psychology Understanding Variation Framework or Roadmap for Improvement Project Act - What changes are to be made? - Next cycle? St d Study - Complete the analysis of the data - Compare data to predictions - Summarize what was learned Plan - Objective - Questions and predictions (Why?) - Plan to carry out th cycle the l (who, what, where, when) - Plan for Data collection Do - Carry out the plan - Document problems and unexpected observations - Begin analysis of the data PDSA – The Continuous Application of the Scientific Method for Improvement 11 Repeated p Use of the PDSA Cycle y Model for Improvement What are we trying to accomplish? How will we know that a change is an improvement? Changes That Result in Improvement A P What change can we make that will result in improvement? S D Implementation of Change Wide-Scale Tests of Change A P S D Hunches Theories Ideas Follow-up Tests Very Small Scale Test 12 The Beginning of the Science of Experimental Design (1920’s) Sir Ronald Fisher Rothamsted Experimental Station 13 Internal Validity Sampling Sample Sample Selection Measurement ?? g Confounding Chance E t External l Validity V lidit Conclusion (generalizability) Clinical epidemiology Fletcher, Fletcher, Wagner W E W. E. Deming’s Deming s Two Types of Studies The aim of any experiment is to provide a rational basis for action Enumerative study: an experiment in which action will be taken on the universe. Chapter 7 from Some Theory of Sampling, 1950 (First discussion in JASA, 1942) Analytic study: an experiment in which action will be taken on a cause system to improve performance in the future. Environment for Enumerative Study Internal Validity Sampling Random Sample Sample Selection Measurement ?? g Confounding Chance Conclusion External Validity (generalizability) Clinical Epidemiology Fletcher, Fletcher, Wagner Environment for Analytic Study (QI Studies) Internal Validity Sample Selection Sample Measurement ?? Confounding Chance C Conclusion l i Clinical epidemiology It is i impossible i ibl tto step t iin th the same river i ttwice i Heraclitus , BC Fletcher, Fletcher, Wagner Important Aspects of Enumerative and Analytic Studies Type of Study Aspects of Study Enumerative Analytic Aim Estimation Prediction Method of Access Frame & Sample Models of product or process o p ocess Major Source of uncertainty Sampling Error Extrapolation to the future Major Source of uncertainty quantifiable? Yes No Environment of the study Static Dynamic Role of the statistician Assess important effects Support subject matter expert Role of the subject matter expert Define the universe approve the frame Identify variables, levels: assess conditions in the future; assess degree of belief Planned Experimentation, 1999 18 Estimation & Prediction in Various Types of Studies Leverage For Improvement Low Estimation Application Examples Acceptance sampling Value inventory Census Theory to support use of the standard error of prediction Probability distribution in combination with a frame and sampling by random numbers Role of subject matter expert Approvall off the A th frame and definition of the complete coverage Exit Poll of voters Stable Process - no expected changes Stable process - minor changes St bl process – major Stable j changes h Shewhart Shewhart Weaker justification Shewhart Weaker justification Poll 2-4 months before election None Prediction that conditions will be relatively l ti l unchanged h d in the future. Prediction that The change will not interact with future conditions. Reasonable simulation of the real thing Pilot p plant studies Prototype testing Accelerated life tests Low dose extrapolation High Prediction Planned Experimentation, 1999 19 Understanding Variation The Shewhart chart is a statistical tool used to distinguish between variation in a measure due t common causes and to d variation due to special causes Walter Shewhart (1891 – 1967) W. Edwards Deming ((1900 - 1993)) Chart Title 100 Upper Lim it Measu ure 90 Center Line 80 Low er Lim it 70 60 1 2 3 4 5 6 7 8 9 10 11 12 13 Run Order 14 15 16 17 18 19 20 21 22 23 24 Using Shewhart Chart to Provide Evidence of Improvement Evidence of Improvement Percent Adm witth Harm 45 40 35 30 25 20 15 10 5 0 1 3 5 7 9 11 13 15 17 19 21 23 25 27 29 31 33 35 37 39 41 43 45 47 Months Figure 4-12: Shewhart Chart Revealing Process or System Improvement Data Guide p. 4‐13 Using Shewhart Chart to Provide Evidence of Sustainability of Improvement 45 Holding the Gain Perce ent Admissiions with Ha arm 40 35 30 25 20 15 10 5 0 4-15: Shewhart Charts Depicting a Process or System “Holding the Gain” Data Guide p. 4‐15 Experimental Patterns for QI Studies Speroff and O’Connor, Study Designs for PDSA Quality Improvement Research, Q .Manage Health Care, Vol 13, No.1, 2004 Multiple Time Series Design Speroff and O’Connor, Study Designs for PDSA Quality Improvement Research, 2004 Study Design for IHI/GCHS Under 5 Mortality Project Multiple Baseline, Baseline Interrupted Time-Series Design Health Center A O O X X X X X X M M M M M M M M Health Center B O O O X X X X X M M M M M M M M Health Center C O O O O O X X X X M M M M Health Center D O O O O O O X X X X M M M M M M Health Center E O O O O O O O O O X X X X M M M Health Center F O O O O O O O O O X X X M M M M Health Center G O O O O O O O O O X X X M M M M Health Center H O O O O O O O O O X X Month 1 2 3 Wave One O – baseline data 4 O 5 6 7 8 9 X M M M M M M 10 11 12 13 14 15 Wave Two X –intervention period M – maintenance period 25 Improving Care in a Pediatric Diabetes Clinic Percent of Diabetes Patients whose HgbA1c measurement has reached CCHMC goal Latest HgbA1c result in preceding 13 months was used for each patient All Therapies Included 40% Control limits: 3 sigma g n = 1308 range g 1205 - 1413 average 35% Protected Phone Time CNPs 25% Tighter Blood Glucose Targets 20% 15% 10% Choice of Th Therapy att Onset Ease in Changing NPH to BBT Consensus Sick Day Guidelines Insulin Pens in Pharmacy Care M Management t for f DKA Heightened A1c Goal G Awareness 5% Short-staffed CNPs Care Management for A1c 0% Ja nFe 03 b0 M 3 ar -0 Ap 3 rM 03 ay -0 Ju 3 n0 Ju 3 l-0 Au 3 gS e 03 p0 O 3 ct N 03 ov -0 D 3 ec -0 Ja 3 nFe 04 b0 M 4 ar -0 Ap 4 rM 04 ay -0 Ju 4 n0 Ju 4 l-0 Au 4 gS e 04 p0 O 4 ct N 04 ov -0 D 4 ec -0 Ja 4 nFe 05 b0 M 5 ar -0 Ap 5 rM 05 ay -0 Ju 5 n0 Ju 5 l-0 5 Percentt of Patients 30% Month Control Limits Percent Center Line Last update: 06-23-05 by H. Atherton, Data source: Disease Management Database Special Cause 26 Factorial Design for Improvement in Diabetes Clinic Response Variables: • HbA1C level • ED visits Care Management g p of Tests either subgroups patients or time periods Therapy Th 1 Therapy Th 2 No C N Care Management Th Therapy Th Therapy 1 2 Manage to easy Glucose G ucose Targets No Sick day guidelines Test 12 Test 7 Test 3 Test 14 Sick day guidelines Test 2 Test 16 Test 11 Test 6 Manage to Tight Glucose Targets No Sick day guidelines Test 9 Test 13 Test 1 Test 15 Sick day guidelines Test 10 Test 4 Test 8 Test 5 27 2^4-1 Factorial for Diabetes Clinics Standard Therapy Self Management Visit Freq: std No Screening g Preventive Screening Education Extensive Optional Therapies Self Management Education Test 3 Test 7 accell T t8 Test T t4 Test std Test 1 Test 6 accel Extensive Test 5 Randomize order of tests and/or sub-sets of patients populations Test 2 Analysis of Data from Quality Improvement Studies The aim of the analysis is to give the experts in the subject matter the best possible chance to take the right action. Fi steps: Five t 1. Show all the data 2. Plot the data in the order in which the tests were conducted. 3. Use graphical displays to assess how much of the variation in the d can be data b explained l i d by b factors f that h were deliberately d lib l changed. h d 4. Rearrange this plot to study other sources of variation 5. Summarize i the h results l off the h study d with i h appropriate i graphical hi l displays. 29 Some References for Analytic QI Studies • • • • • • • • • • “Classification Problems of Statistical Inference” W. E. Deming, Journal of the American Statistical Association, June 1942. Some Theory of Sampling Sampling, W. W Edwards Deming (1950), (1950) Dover Publications, Publications NY. NY “On Probability as a Basis for Action”, The American Statistician, Vol. 29, No. 4, (1975), pp 146-152. Out of the Crisis Crisis, W. W Edwards Deming (1982), (1982) MIT CAES CAES, Cambridge. Cambridge Quality Improvement Through Planned Experimentation, Ron Moen, Thomas Nolan, Lloyd Provost (1999), McGraw-Hill, NY. ssu pt o s for o Stat Statistical st ca Inference”, e e ce , The he American me ican Statistician, Vo Vol 47, 7, No. 1,, Ge Gerald ad “Assumptions Hahn, William Meeker (1993), pp 1-11. “A Primer for Enumerative Vs. Analytic Studies: Using Caution in Statistical Inferences,” ASQ Statistics Division Newsletter, Vol 16, No. 3 Eileen Beachell, Marilyn Monda (1996), pp 6-10. Quality Improvement through Planned Experimentation, 2nd edition Ron Moen, Thomas Nolan, Lloyd Provost (1999), McGraw-Hill, NY. The h New Economics for f Industry, d Government, Education. d 2ndd Edition. d W. Edwards d d Deming, Cambridge: MIT Press, 2000 The Data Guide: Learning from Data to Improve Health Care, L. Provost and S. Murray, Associates in Process Improvement, Improvement 2010. 2010