Objectives
advertisement

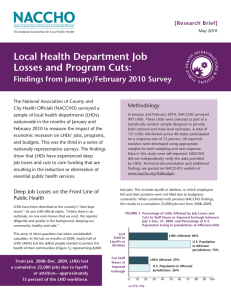
Objectives • To determine the proportion of LHDs that have had their budgets reduced compared to previous fiscal year • To examine the extent to which LHD budgets have decreased over the past year Factors Associated with Recent Budget Reductions for Local Health Departments Evidence from Two Nationwide Surveys • To identify organizational characteristics that are associated with vulnerability to budget cut Gulzar H. Shah, PhD, MStat, MS Carolyn J. Leep, MS, MPH Barbara Laymon, MPH Study Design Study Design (2) • Linked data from two cross-sectional nationwide surveys of LHDs conducted by NACCHO in late 2008 • National Survey of LHD Budget Changes – Predominantly census approach (N=2,422) •with exception of five states, where some sampling was performed to prevent one individual from receiving multiple surveys – Respondents = 1,079 • The 2008 National Profile of LHDs (core questionnaire) Statistical Methods: • Bivariate analysis using t-tests/eta-square, chi-square, Somer’s D and Kendal’s Tau B as appropriate • Three-way Tables • Logistic regression of dichotomous variable “whether or not LHD experienced a budget cut” – Complete census of all LHDs (N=2,794) – Respondents = 2,332 Number of LHDs that participated in both surveys =1,021 Results – Whether Budget was Reduced Results – Whether Budget was Reduced by LHD Size Percent of LHDs with reduced current budget compared with prior year Percent of LHDs with type of change in current operating year budget (vs. prior year) Approximately same 47.5 50.0 45.0 50% Percent of LHDs 35.0 30.0 Less 26.5 40% Greater 26.0 25.0 45% 45% 40.0 Percent of LHDs • 37% 35% 30% 25% 25% 22% 20% 20% 15% 20.0 10% 15.0 5% 0% 10.0 <25,000 25,000 - 49,999 50,000 - 99,999 5.0 100,000 499,999 500,000 + LHD size .0 Nature of budget change Note: Differences among LHDs in different population size strata were statistically significant, based on Chi-square and Somers’ d statistic (P<0.000) Level of Budget Reduction Jurisdiction Population Starts at coast; moves in All LHDs <25,000 25,000 - 49,999 50,000 - 99,999 100,000 - 499,999 500,000+ Starts at coast; moves in Budget Decrease (Current Year vs. Prior) Median Mean 6% 9% 6% 10% 10% 10% 9% 9% 5% 7% 5% 9% Note: Differences among LHDs in different population size strata were statistically non-significant, based on ANOVA test (P=0.08) NOTE: At the time of data collection in late 2008, some states were just entering budget periods, recession not fully recognized Average Amount of Budget Reduction Jurisdiction Population All LHDs <25,000 25,000 - 49,999 50,000 - 99,999 100,000 - 499,999 Percent with Reduced Budget by LHD Size and Governance Category Budget Decrease (Current Year vs. Prior) Median Mean $100,000 $480,000 $25,000 $45,000 $70,000 $110,000 $100,000 $180,000 $250,000 $540,000 LHD population size <50000* 50000-499999* 500000+ LHD budget Type of was less than governance previous year 40.4% State 19.1% Local 59.7% State 25.4% Local 50.0% State 40.0% Local * Differences are statistically significant based on Chi-square, Somer's d and Kendal's Tau B (P<0.01) Percent with Reduced Budget by LHD Size and Presence of a Local Board of Health Presence of local board LHD population size of health <50000 Yes No 50000-499999* Yes No 500000+ Yes No LHD budget was less than previous year 20.9% 26.5% 25.5% 54.7% 35.3% 46.4% * Differences are statistically significant based on Chi-square, Somer's d and Kendal's Tau B (P<0.000) Total LHD Expenditures and Revenues and Source-Specific Percentage of Revenues After controlling for the LHD size (Small, Medium, Large), the following relationships were noted with budget cut: • Larger LHD revenue (+ ; p<0.0001) • Larger LHD expenditure (+ ; p<0.0001) • Higher percent of revenues from State (direct and federal passthrough) (+ ; p<=0.001) • Higher percent of revenues from Federal sources (direct) (+ ; p<0.0001) • Higher percent of revenues from Medicaid (- ; p<0.0001) • Higher percent of revenueset from Patient personal fees (- ; p=0.009) Results of Logistic Regression of Whether LHD Budget was Reduced (1) Results of Logistic Regression of Whether the Budget was Reduced (2) After controlling for other covariates in the model, the following variable were significantly associated with budget cut [listed in the order of effect and with direction of association] 4. Performing certain emergency preparedness activities (+): 1. Centralized Governance (+ ; 3 times more likely) 2. Employing epidemiologist – (+ ;1.6 times more likely) 3. Percent of revenues from patient personal fees — high (-) – Reviewed relevant legal authorities to isolate and/or quarantine individuals, groups, facilities, animals, and food products – Participated in drills or exercises: functional level – Provided emergency preparedness training to staff on NIMS compliance 5. Percent of revenues from State (direct and federal pass-through) –high (+) 6. Employing nutritionist -- (-) 7. Screening of certain diseases (HIV/STD; Tuberculosis; Cardiovascular disease) (+) 8. Size of LHD (9 population categories) – (direction Questions • Thanks you • Contact info – Gulzar H. Shah; email gshah@naccho.org inconclusive)