Melanoma — An Unlikely Poster Child for Personalized Cancer Therapy
advertisement

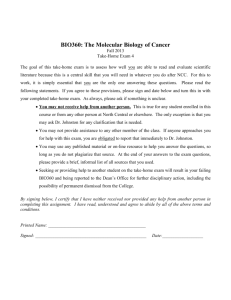
The n e w e ng l a n d j o u r na l of m e dic i n e edi t or i a l s Melanoma — An Unlikely Poster Child for Personalized Cancer Therapy Keiran S.M. Smalley, Ph.D., and Vernon K. Sondak, M.D. Personalized medicine has long been a mainstay of the treatment of localized melanoma, involving surgical decisions that are individualized on the basis of measured differences as small as 0.01 mm, as well as other biomarkers of metastatic potential, such as the presence of ulceration or mitoses.1 Once melanoma spreads beyond the regional nodes, however, the lack of validated molecular targets hampers efforts to individualize therapy. In this issue of the Journal, Flaherty and coworkers2 provide clinical proof that mutations in the gene encoding the serine–threonine protein kinase B-RAF (BRAF) are bona fide therapeutic targets in melanoma. A remarkable 81% of patients whose melanomas had an activating mutation in BRAF had a response to treatment with the new BRAF kinase inhibitor PLX4032 in a multicenter, phase 1, dose-escalation trial. Responses to PLX4032 were dependent on mutation status, with no complete or partial responses (according to the Response Evaluation Criteria in Solid Tumors [RECIST]) seen in patients with melanomas carrying wild-type BRAF. These results represent a major breakthrough and provide proof of the principle that the treatment of metastatic melanoma can be individualized for a substantial percentage of patients. Over the past decade, great strides have been made in unraveling the unique biology of melanoma, and the research investment is paying off. The discovery in 2002 that approximately 50% of human melanomas harbor an activating mutation in BRAF resulting in a substitution of glutamic acid for valine at amino acid 600 (the V600E mu- 876 tation) first raised the possibility that melanoma may be amenable to targeted therapy.3 Since then, extensive preclinical data have validated the V600E mutation as an important therapeutic target in melanoma. In parallel studies, activating mutations in the human KIT gene (encoding the v-kit Hardy–Zuckerman 4 feline sarcoma viral oncogene homologue) were identified in a small minority of melanomas, and there is now evidence that imatinib therapy leads to tumor regression in this group of patients.4 But the very low frequency of KIT mutations in melanoma limited the impact of this discovery. BRAF is an upstream component of the growthpromoting mitogen-activated protein (MAP) kinase pathway, and it is known that melanoma cells containing mutant BRAF are dependent on MAP kinase signaling for their growth and survival.5 Flaherty and colleagues confirmed this in paired-biopsy studies and showed that PLX4032 effectively blocked intratumoral MAP kinase activity, leading to reduced expression of cyclin D1 and the proliferation marker Ki-67. Responses to PLX4032 occurred in patients who had previously received multiple chemotherapy regimens, as well as at organ sites such as bone and liver that are typically refractory. Overall, PLX4032 had moderate toxicity, with rash of grade 2 or 3, fatigue, and arthralgia being the major dose-limiting toxic effects. Somewhat unexpectedly, cutaneous squa­ mous-cell carcinomas, mostly of the keratoacanthoma type, developed in a significant percentage of patients. Even after accounting for the facts that such tumors have been seen with the use of other kinase inhibitors and patients with one cu- n engl j med 363;9 nejm.org august 26, 2010 The New England Journal of Medicine Downloaded from nejm.org at UC SHARED JOURNAL COLLECTION on July 14, 2014. For personal use only. No other uses without permission. Copyright © 2010 Massachusetts Medical Society. All rights reserved. editorials taneous neoplasm are at high risk of others, the incidence of this type of squamous-cell carcinoma was quite high. PLX4032 is not the first agent aimed at BRAF to be evaluated for the treatment of melanoma. The most thoroughly investigated anti-BRAF agent to date is the multikinase inhibitor sorafenib (Nexavar). Unlike PLX4032, sorafenib has little single-agent activity in melanoma, and two large trials of sorafenib and chemotherapy, as compared with the same chemotherapy alone, showed no significant effect of the addition of the inhibitor (ClinicalTrials.gov numbers, NCT00111007 and NCT00110019).6,7 This led many to question the validity of BRAF as a target in melanoma, and had the more specific inhibitors of mutant BRAF been a clinical failure, the approach might well have been abandoned. Instead, the future holds the promise that patients with metastatic melanoma will undergo screening, before the initiation of therapy, for the presence of mutations in BRAF, KIT, and probably other key genes. An important reason to confirm the BRAF mutational status of patients comes from the surprise finding that BRAF inhibitors paradoxically stimulate MAP kinase–mediated cell proliferation in cell lines lacking BRAF mutations.8 Mechanistically, this seems to occur because BRAF inhibitors have the ability to transactivate RAF1 (the v-raf-1 murine leukemia viral oncogene homologue 1, also known as CRAF),8 and this may well underlie the frequent development of keratoacanthomas in patients receiving PLX4032. Clearly, the administration of PLX4032 or similar BRAF inhibitors to patients whose melanomas do not carry BRAF mutations should be avoided for the time being. The impressive responses seen in the study by Flaherty and colleagues do not necessarily persist for extended periods, although the median duration of progression-free survival was not yet reached at the time of publication and will probably exceed 7 months. This pattern of initial response and eventual resistance is similar to that seen with targeted therapy in other tumors. Although we currently know little about the mechanisms of resistance to PLX4032 therapy, Flaherty and colleagues did not find that any tumors had new or novel BRAF mutations (such as the “gatekeeper” mutations found in the epidermal growth factor receptor after erlotinib therapy). The mech- anisms of PLX4032 resistance may be diverse; personalized therapy may equal personalized failure. Studies in vitro indicate that exogenous growth factors or cytokines rescue melanoma cells from apoptosis when BRAF is knocked down by small interfering RNA,9 and that resistance to BRAF inhibitors can be mediated through pathway switching, wherein MAP kinase signaling is routed from BRAF to RAF1 (Fig. 1A).10 Melanoma cells that are resistant to BRAF inhibitors seem to remain reliant on MAP kinase signaling, and this may direct future efforts: preclinical data already suggest that combined inhibition of BRAF and MEK (a component of the MAP kinase pathway) abrogates the emergence of resistance,11 and a clinical trial is currently under way to investigate this dual approach to treating melanoma (NCT01072175). Although much attention has focused on acquired PLX4032 resistance, in the extension cohort in the study by Flaherty and colleagues, 19% of the patients with melanomas carrying the V600E BRAF mutation showed evidence of intrinsic resistance (i.e., did not have an objective response on the basis of RECIST criteria). A number of mechanisms probably underlie this intrinsic resistance; melanoma cells that either lack phosphatase and tensin homologue (PTEN) function or possess cyclin D1 amplification may be able to survive and proliferate when BRAF is inhibited (Fig. 1B). These and other “escape routes” could limit dual-inhibitor approaches as well; thus, even more novel strategies may be needed. The recent observation that ipilimumab, a monoclonal antibody directed against the inhibitory cytotoxic T-lymphocyte–associated antigen 4 (CTLA4) molecule on T cells, improves survival in patients with metastatic melanoma12 suggests the possibility of combining CTLA4 blockade with BRAF inhibition. CTLA4 blockade also offers a viable alternative therapy for patients who do not have a defined mutation to target. Even for patients whose melanomas contain mutant BRAF, decisions about therapy with an inhibitor versus ipilimumab will have to be individualized, since the overall effect of PLX4032 therapy on survival is still undefined. Nonetheless, the data provided by Flaherty and colleagues represent a major advance in the treatment of metastatic melanoma. But what’s next? How much can we improve on these results — especially in terms of extending the duration of dis- n engl j med 363;9 nejm.org august 26, 2010 The New England Journal of Medicine Downloaded from nejm.org at UC SHARED JOURNAL COLLECTION on July 14, 2014. For personal use only. No other uses without permission. Copyright © 2010 Massachusetts Medical Society. All rights reserved. 877 The n e w e ng l a n d j o u r na l A Tumor PI3K PLX4032 BRAF V600E MEK inhibitor MEK PTEN RAF1 AKT ERK Apoptosis Cyclin D1 Growth B PI3K RAS PLX4032 BRAF V600E MEK inhibitor MEK PTEN RAF1 AKT ERK Cyclin D1 Apoptosis Amplified Growth COLOR FIGURE ease control — through combination therapy Draft 5 8/09/10 or even by manipulating the dose and schedule of Author Sondak 1 Fig # single-agent therapy?13 When should this therapy Inhibition of Mutated, Activated Title BRAF in Metastatic be moved to the adjuvant setting? How Melanoma can we ME achieve similar success in treating patients with DE Longo Artist Knoper wild-type BRAF? The prospects for patients with AUTHOR PLEASE NOTE: metastatic melanoma haveFigurenever been brighter, has been redrawn and type has been reset Please check carefully but the need for further Issue progress through labodate 8/26/10 ratory research and well-conducted clinical trials is as great as — or greater than — ever. Disclosure forms provided by the authors are available with the full text of this article at NEJM.org. From the Departments of Molecular Oncology (K.S.M.S.) and Cutaneous Oncology (K.S.M.S., V.K.S.), Moffitt Cancer Center and Research Institute, Tampa, FL. 1. Case Records of the Massachusetts General Hospital (Case 2-2007). N Engl J Med 2007;356:285-92. 2. Flaherty KT, Puzanov I, Kim KB, et al. Inhibition of mutated, activated BRAF in metastatic melanoma. N Engl J Med 2010; 363:809-19. 3. Davies H, Bignell GR, Cox C, et al. Mutations of the BRAF gene in human cancer. Nature 2002;417:949-54. 4. Hodi FS, Friedlander P, Corless CL, et al. Major response to imatinib mesylate in KIT-mutated melanoma. J Clin Oncol 2008; 26:2046-51. 878 n engl j med 363;9 m e dic i n e Figure 1. Intracellular Signaling Pathways in Melanoma Known to Be Important in the Response and Resistance to Targeted Therapy. Panel A shows two signaling pathways known to be important for the growth and progression of melanoma. Constitutive mitogen-activated protein (MAP) kinase signaling in the RAS–RAF–MEK–ERK pathway drives the growth of melanoma cells through the up-regulation of cyclin D1 expression. Treatment with PLX4032 can result in the regression of melanomas harboring the BRAF V600E mutation because the drug blocks the activity of the mutant BRAF. Survival of melanoma cells and resistance to apoptosis are often mediated through the constitutive activity of phosphoinositide-3-kinase (PI3K) and the serine–threonine protein kinase AKT, which arises through multiple mechanisms, including loss of expression of the tumor suppressor phosphatase and tensin homologue (PTEN). Panel B illustrates potential mechanisms by which BRAF V600E mutated melanomas may show intrinsic or acquired resistance to BRAF inhibition. Increased signaling through RAF1, possibly due to increased RAF1 expression or increased receptor tyrosine kinase activity, restores MEK and ERK activity and results in cyclin D1 expression. In addition, some melanomas harboring BRAF V600E mutations may already have cyclin D1 amplification, whereas others may have lost PTEN expression; these melanomas may be particularly likely to manifest intrinsic resistance to BRAF-inhibitor therapy. Since resistance to BRAF inhibitors is associated with a continued reliance on the RAS– RAF–MEK–ERK pathway, MEK inhibitors will probably be useful in the management of acquired resistance to BRAF inhibitors. Increased receptor tyrosine kinase activity RAS of 5. Wellbrock C, Karasarides M, Marais R. The RAF proteins take centre stage. Nat Rev Mol Cell Biol 2004;5:875-85. 6. Hauschild A, Agarwala SS, Trefzer U, et al. Results of a phase III, randomized, placebo-controlled study of sorafenib in combination with carboplatin and paclitaxel as second-line treatment in patients with unresectable stage III or stage IV melanoma. J Clin Oncol 2009;27:2823-30. 7. Flaherty KT, Lee SJ, Schuchter LM, et al. Final results of E2603: a double-blind, randomized phase III trial comparing carboplatin (C)/paclitaxel (P) with or without sorafenib (S) in metastatic melanoma. J Clin Oncol 2010;28:Suppl:613s. abstract. 8. Poulikakos PI, Zhang C, Bollag G, Shokat KM, Rosen N. RAF inhibitors transactivate RAF dimers and ERK signalling in cells with wild-type BRAF. Nature 2010;464:427-30. 9. Christensen C, Guldberg P. Growth factors rescue cutaneous melanoma cells from apoptosis induced by knockdown of mutated (V600E) B-RAF. Oncogene 2005;24:6292-302. 10. Montagut C, Sharma SV, Shioda T, et al. Elevated CRAF as a potential mechanism of acquired resistance to BRAF inhibition in melanoma. Cancer Res 2008;68:4853-61. 11. Paraiso KH, Fedorenko IV, Cantini LP, et al. Recovery of phospho-ERK activity allows melanoma cells to escape from BRAF inhibitor therapy. Br J Cancer 2010;102:1724-30. 12. Hodi FS, O’Day SJ, McDermott DF, et al. Improved survival with ipilimumab in patients with metastatic melanoma. N Engl J Med 2010;363:711-23. 13. Gatenby RA. A change of strategy in the war on cancer. Nature 2009;459:508-9. Copyright © 2010 Massachusetts Medical Society. nejm.org august 26, 2010 The New England Journal of Medicine Downloaded from nejm.org at UC SHARED JOURNAL COLLECTION on July 14, 2014. For personal use only. No other uses without permission. Copyright © 2010 Massachusetts Medical Society. All rights reserved.