Lower Extremity Critiques -- File 00 Image # 8
advertisement

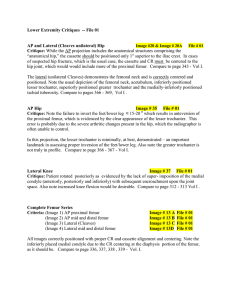
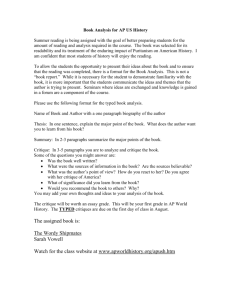
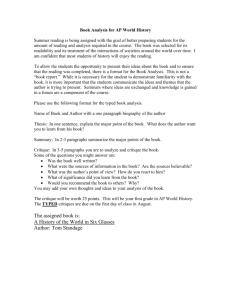
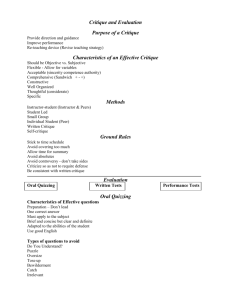
Lower Extremity Critiques -- File 00 Ankle: AP(1); Oblique(2); Lateral(3) Image # 8 File # 00 Critique: AP - correctly positioned . Ankle mortis (joint) is clearly seen. Obl. - more obliquity needed. Note shape of talus, and see Vol I- pg. 297 - 15-20 0 versus 45 0 obliquity. Lat - Not true lateral; note fibula positioned posterior to tibia. Knee - Intercondylar Fossa Image # 33 File # 00 Critique: Note the distortion of the superior aspect of intercondylar fossa due to rotation of the femur. Note also the enlarged appearance of the medial condyle due also to femoral rotation. Compare to pages 320, 321, 322, 323 - 324, 325, Vol. I. Patella - Settegast et al Image # 7 File # 00 Critique: Note the angled and off-centered appearance of the patella due to minimal femoral obliquity or CR not parallel to patella. (Probably due more so to CR, rather than femoral obliquity, although slight femoral obliquity is present). Compare to pages 331, 332, 334, 335, Vol I. Lateral Knee Image # 32 File # 00 Critique: Note the ≈ 45 0 over- flexion of the knee joint as compared to the preferred 20-30 0 flexion as depicted on page 312 - 313 - Vol I. Lateral Foot (customary mediolateral projection) Image # 22 File # 00 Critique: Note the lack of dorsiflexion and the improper placement/ alignment of the foot with the long-axis of the film. A 10 x 12 cassette would have improved the accommodation of this patient’s foot. Compare with page 292 - Vol I. AP Knee Image # 18 File # 00 Critique: Note the off-centered location of the knee joint. The knee joint appears “somewhat” closed due to the violation of the law of tangents. Remember, the CR must enter ½" below the patellar apex. Also remember, the patella is an inverted anatomically positioned triangle. So, palpate the apex. Compare to 309, image B - Vol I. Lateral Knee Image # 19 File # 00 Critique: Note the rotation of the femur and the subsequent lack of superimposition of the femoral condyles - not a true lateral. Also note the extent to which the medial condyle obscures the knee joint, which is greatly influenced by the failure to center the knee to the CR. Another example of violation of the law of tangents. The CR should enter 1" below the femoral medial epicondyle, with the cassette centered to the CR. The purpose of CR angulation of 5-7 0 is to achieve superimposition of the condyles, which opens the joint space. Compare to page 312 313 Vol I . Page 1 AP and Oblique Ankle Image # 5 File # 00 Critique: Note failure to dorsiflex AP and Oblique positions. Also note off-centering of ankle joint which, in this case, could have resulted in clipping of the orthopedic alignment/reduction plates . Compare to pages 291, 295, 296, 297, Vol I . Lateral Ankle Image # 6 File # 00 Critique: Not a true lateral. Note posteriorly positioned fibula with respect to the tibia. Lack of dorsiflexion is due to the cast, which the radiographer is unable to control. Compare to page 292 - 293, Vol I . Lateral Ankle Image # 34 File # 00 Critique: Note failure to dorsiflex. Orthopedic alignment/reduction plates may play a role which the radiographer is often unable to control. Compare to page 292 - 293, Vol I . AP and Oblique Ankle Image # 23 File # 00 Critique: AP - demonstrates minimal foot inversion with lack of sufficient dorsiflexion. Both positioning errors contribute to a closed joint appearance (talus-fibula articulation Obl demonstrates failure to dorsiflex. Note fibula encroaching upon tibia and talus, thus diminishing visibility of the ankle mortis joint . Compare to page 291, 295, 296, 297 - Vol I . Note: Comments regarding minimal foot inversion on AP ankle projections are intended to suggest that the intermalleolar line is not with the plane of the film/table. Hence, there is rotation from normal anatomical position. Page 2