Document 11157073
advertisement

Comparing Long-term Antiplatelet Strategies To Prevent Morbidity And Mortality In Patients With
Drug-Eluting Coronary Stents
by
J. Stewart Evans
MD, Drexel University College of Medicine, 2001
Diplomate in Internal Medicine, American Board of Internal Medicine
Submitted to Health Science and Technology in
Partial Fulfillment of the Requirements for the Degree of
Master of Science in Biomedical Informatics
MASSACHUEr"-!N!$ rI I~ I
at the
Massachusetts Institute of Technology
MAR 01 2
BLIRARIES
August 6, 2010
©2010 J. Stewart Evans, All rights reserved
The author hereby grants to MIT permission to reproduce and to distribute publicly paper and electronic
copies of this thesis document in whole or in part.
Signature of Auth or .
' I-- ---- --- --
.............................................................
*******- *- -
Post-Doctoral Fellow, Boston-Area Biomedical Informatics Research Training Program
August 6, 2010
Certified by.......
Program
Certified by.......
Alexa T. McCray
ector, B ston-Area Biomedical Informatics Research Training Program
Thesis Supervisor
. . .........
... .... ... ... ............
Stephen G. Pauker
Professor of Medicine, Tufts University School of Medicine
Thesis Supervisor
Certified by...
John B. Wong
Professor of Medicine, Tufts University School of Medicine
Thesis Supervisor
Accepted by....... ....................... .
.....................................................................
Ram Sasisekharan, PhD/Director
Harvard-MIT Division of Health Sciences and Technology/
Edwa rd Hood Taplin Professor of Health Sciences & Technology and Biological Engineering
Comparing Long-term Antiplatelet Strategies to Prevent Morbidity and Mortality in Patients with
Drug-Eluting Coronary Stents
by
J. Stewart Evans
Submitted to the Division of Health Sciences and Technology
on August 6, 2010 in partial fulfillment of the
requirements for the Degree of Master of Science in
Biomedical Informatics
1.ABSTRACT
Background: The optimal long-term antiplatelet therapy (APT) that balances the benefit of
preventing myocardial infarction (MI) with the risk of severe bleeding is unknown in patients
greater than one year after drug-eluting stent (DES) placement.
Methods: We modeled life expectancy (LE) using published data by building a Markov model to
compare several APT strategies composed of aspirin and clopidogrel, both as monotherapy and in
various clinically plausible combinations. The base case examined a 65-year old person treated
with a DES then continuous aspirin plus clopidogrel (Dual-Rx) for one year without
complications. We considered risk of mortality from myocardial infarction and severe bleeding.
We used a lifetime horizon and projected LE without quality-adjustment.
Results: In the base-case analysis, APT yielding greatest LE was a toss-up between Dual-Rx
indefinitely (LE of 13.48 years), clopidogrel indefinitely (LE of 13.45 years), and aspirin
indefinitely (LE of 13.42 years); of the strategies considered, no APT was least preferred (LE of
13.36 years). All parameters were varied over plausible ranges in sensitivity analyses, including
the duration of future treatment with clopidogrel (base-case, life long). The choice of APT
remained a toss-up unless: the annual probability of MI fell below 0.0087 (base-case, 0.013) or
the relative risk of systemic bleeding exceeded 1.52 (base case, 1.00), in which case clopidogrel
indefinitely was preferred; or the efficacy of clopidogrel to prevent MI fell below 0.09 (base case,
0.20) or the relative risk of clopidogrel for severe gastrointestinal hemorrhage exceeded 3.33
(base case, 2.01), in which case aspirin indefinitely was preferred.
Conclusions: For patients with a drug-eluting stent placed greater than one year ago, the antiplatelet therapy which yields the greatest life expectancy is a toss-up between dual antiplatelet
therapy (clopidogrel plus aspirin indefinitely), clopidogrel indefinitely, and aspirin indefinitely.
However, additional research (including a clinical trial, subgroup analysis, and modeling) is
needed.
Thesis Supervisor: Alexa T. McCray
Title: Associate Professor of Medicine, Harvard Medical School
Thesis Supervisor: Stephen G. Pauker
Title: Professor of Medicine, Tufts University School of Medicine
Thesis Supervisor: John W. Wong
Title: Professor of Medicine, Tufts University School of Medicine
ACKNOWLEDGEMENTS
I would like to thank for their support: my thesis advisers; the National Library of Medicine; my
patients; my family and friends; and the many more who I have not mentioned.
I am deeply grateful to everyone.
2
TABLE OF CONTENTS
1. A B ST R A C T .......................................................................................................................
6
2 . BA C KG R O U N D ...............................................................................................................
7
2 .1. Introd u ctio n ................................................................................................................
7
2 .2 . A im .............................................................................................................................
8
3. MATERIALS AND METHODS.......................................................................................
9
3 .1. D ata - O verv iew .........................................................................................................
9
3.2. Data - M eta-A nalysis................................................................................................
9
3.2.1.Meta-Analysis - General Principles...........
...................................
3.2.2.Meta-Analysis - Selection of Methods..............................................................
3.2.3.Meta-Analysis - Fixed Effect and Random Effects Methods............................
9
9
10
3.2.3.1.
Meta-Analysis - Fixed Effect Methods............................................
10
3.2.3.2.
Meta-Analysis - Random Effects Methods.......................................
12
3.2.4.Meta-Analysis - Confidence Interval for Overall Effect..........
........
13
3.2.5.Meta-Analysis - Test Statistic for Overall Effect...............................................
14
3.2.6.Meta-Analysis - Test Statistic of Homogeneity.................................................
14
3.3. Data - C ardiovascular Events.....................................................................................
14
3.3.1.Cardiovascular Events - Overview.....................................................................
14
3.3.2.Cardiovascular Events - Rate of Myocardial Infarction (MI) Incidence.............
15
3.3.2.1.
Rate of MI Incidence - Overview..
.......................................
15
3.3.2.2.
Rate of MI Incidence - Meta-Analysis..............................................
15
3.3.2.2.1.
Meta-Analysis - Study Selection..........................................
15
3.3.2.2.2.
Meta-Analysis - Data Extraction..........................................
17
3.3.2.2.3.
Meta-Analysis - Data Conversion.....................
18
3.3.2.2.4.
Meta-Analysis - Meta-analytic Methods............................
19
3.3.2.2.5.
Rate of MI Incidence - Additional Considerations..............
20
3
3.3.3.Cardiovascular Events - Rate of Myocardial Infarction (MI) Mortality..........
3.4. D ata - H em orrhage....................................................................................................
20
3.4.1. H em orrhage - D efinition...................................................................................
20
3.4.2. Hem orrhage - Bleeding Sites............................................................................
21
3.5. Data - A ntiplatelet Therapy......................................................................................
21
3.5. I.A ntiplatelet Therapy - Efficacy.........................................................................
21
3.5.2.A ntiplatelet Therapy - R isk..............................................................................
23
3.6. Decision M odel..........................................................................................................
4.
20
23
3.6.1. D ecision M odel - O verview ..............................................................................
23
3.6.2.D ecision M odel - Structure..............................................................................
24
3.6.3.D ecision M odel - A ssum ptions.........................................................................
24
3.7. Sensitivity A nalysis..................................................................................................
26
RESU LTS..........................................................................................................................
27
4.1. Meta-A nalysis............................................................................................................
27
4.1 . .Rate of M yocardial Infarction Incidence............................................................
27
4.1.2.Efficacy of D ual A ntiplatelet Therapy................................................................
27
4.2. Decision M odeling.....................................................................................................
29
4.2.1.Base-Case A nalysis............................................................................................
29
4.2.2.Sensitivity A nalysis.............................................
29
4
5. DISCUSSION ....................................................................................................................
31
5.1. Overview ....................................................................................................................
31
5.2. Lim itations.................................................................................................................
32
5.3. Com parison w ith Other Studies................................................................................
32
5.4. Future Directions.......................................................................................................
33
REFERENCES ..................................................................................................................
35
7. APPEN DICES...................................................................................................................
39
6.
7.1. Appendix A : List of Abbreviations............
........
..............
7.2. Appendix B: List of Tables and Figures.................................
...............
39
.............................
39
.......
7.3. Appendix C: Tables..................................................................................................
40
7.4. Appendix D : Figures..................................................................................................
52
5
2.BACKGROUND
2.1. Introduction
Since their approval by the United States Food and Drug Administration in 2003 and 2004
respectively, the paclitaxel and sirolimus drug-eluting coronary stent systems (DES) have quickly
become the most commonly deployed type of coronary stent in the United States, together
comprising 58% of stents placed. More than one million DES are now placed annually in the
U.S., and over six million have been placed worldwide.
Both types of DES reduce the risk of in-stent restenosis in the first six to nine months postpercutaneous coronary intervention compared to bare-metal stents. However, since Food and
Drug Administration approval, DES have been associated with an increased risk of stent
thrombosis compared to bare-metal stents, particularly greater than one year post-DES placement
[1, 2]. Stent thrombosis is an uncommon complication (estimates vary from 0.2-2.0%), but one
that has a high morbidity, mainly myocardial infarction (MI) and mortality, regardless of stent
type [3, 4].
The benefits of APT with aspirin or clopidogrel as monotherapy in coronary heart disease are
well-known [3, 5].
Due to their complementary antiplatelet effects, combining aspirin and
clopidogrel, hereafter referred to as dual antiplatelet therapy (DAT), has been shown to have
more benefit than aspirin monotherapy in patients above certain risk thresholds for MI [6]. In
2007, this benefit was expanded to include reducing the risk of MI and death in patients with DES
compared to aspirin monotherapy.
Moreover, studies have suggested that this risk reduction
might progressively increase greater than one year post-DES placement [7].
As a result,
guidelines were changed from recommending Dual-Rx from three and six months for sirolimus
and paclitaxel DES, respectively, to DAT at least one year for both, and possibly longer if its
benefit of preventing stent thrombosis continues to outweigh the risk of major bleeding [3, 8, 9].
However, the optimal duration of DAT for patients with DES is unknown, in part due to
significant evidence that the most commonly prescribed medications in DAT also increase the
risk of severe bleeding [5, 10-12]. This balance of risks and benefits is especially complex in
patients with certain risk combinations of MI and severe bleeding [7, 12].
While plans are underway to conduct a clinical trial to inform the optimal APT for patients with
DES, with the understandable time course of a clinical trial, results are not scheduled to be
available until four years after trial initiation. In the meantime, for a significant proportion of the
six million patients world-wide who have had DES placed, and many more to follow, important
decisions remain in the interim with regard to optimal duration and type of APT.
2.2 Aim
The aim of the current study is to construct a Markov state transition model [13] to examine the
optimal APT to prevent MI and death for patients who have had an acute MI treated with DES
one year ago.
3.MATERIALS AND METHODS
3.1. Data - Overview
For each data element used in the current study, we applied widely used methods for finding and
summarizing estimates, depending on the best evidence available publicly or in published form
[14]. These included meta-analyses, systematic reviews of primary studies, 'best' single study,
and expert opinion. When there was more than one high quality source, we conducted our own
meta-analyses.
Meta-analysis was also conducted to manage temporal complexity and
uncertainty, as summarized below. Fuller description of meta-analytic principles are in [15, 16].
3.2. Data - Meta-Analysis
3.2.1.
Meta-Analysis - General Principles
Meta-analysis is a two-stage process which involves, for a set of N studies, first calculating a
summary statistic for each study, then combining these statistics into a weighted average. The
weights are chosen to reflect the amount of information each trial contains, and are often the
inverse of the variance of the treatment effect, which is closely related to sample size. The
precision (confidence interval) and statistical significance of the overall estimate are also
calculated. All commonly used methods of meta-analysis follow these basic principles. There
are, however, other aspects that vary between methods. None of the methods can compensate for
publication bias, nor bias introduced through poor trial design and execution.
3.2.2.
Meta-Analysis - Selection of Methods
Selection of a meta-analysis method for a particular analysis should reflect the data type, choice
of summary statistic (considering the consistency of the effect and ease of interpretation of the
statistic), observed heterogeneity, and the known limitations of the computational methods.
There are three aspects of choosing a method for meta-analysis: identifying the data type (binary,
continuous, time to event), choosing an appropriate summary statistic, and selecting a weighting
method for combining the studies.
The choice of a summary statistic depends upon the consistency of estimates of the treatment
effect across data sets - the more consistent the estimate, the greater the justification for
expressing the effect of treatment in a single summary number. A second consideration is that
the summary statistic should be in a form that is easily understood and applied. For the purposes
of the current application, the choice of summary statistic was based on what form of data was
required for input into the model, and what form of data would be understood most easily by
those using the results of the analysis were reported to those who may not be as familiar with
modeling (e.g., clinicians, policy makers). Selection of a summary statistic for continuous data
also requires consideration of whether all data sets report the outcome using the same scale.
The choice of weighting method depends deciding between various fixed and random effects
methods. It is important to be aware of circumstances in which methods may give erroneous
results. Erroneous results may occur with inverse variance methods when data sets are small or
when events rates or very low. In the current application, it was determined that the data sets and
events for our use of the inverse variance method were sufficient to provide reliable results.
3.2.3.
Meta-Analysis - Fixed Effect and Random Effects Methods
3.2.3.1. Fixed Effects Methods
Fixed effect models average the summary statistics, weighting them according to a measure of the
quantity of information they contain. It is assumed that the true effect of treatment is the same
value in each study, or "fixed", the differences between study results being due solely to chance.
The assumption of a fixed effect can be tested using a test of homogeneity. Several methods are
available, which differ mainly in the computations used to calculate the individual study weights.
For the current application, we chose the inverse variance method.
With the inverse variance method, the effect sizes are combined to give a pooled estimate by
calculating a weighted average from the individual data sets:
The weights are the reciprocals of the squared standard errors:
SEOI
Thus larger data sets, which have smaller standard errors, are given more weight than smaller
studies, which have larger standard errors. This choice of weight minimizes the variability of the
pooled treatment effect.
The standard error is given by
(
SE~
E
I
The heterogeneity statistic is given by
The strength of the inverse variance method is its wide applicability. It can be used to combine
any estimates that have standard errors available. In the current study, we applied this method to
combine event rates for MI and efficacy of Dual-Rx.
3.2.3.2. Random Effects Methods
Random effects methods incorporate an estimate of between study variation (heterogeneity) into
the calculation of the common effect.
The treatment effects for the individual studies are
assumed to vary around some overall average treatment effect.
Usually the effect sizes are
assumed to have a normal distribution with a certain mean and variance. A test for homogeneity
tests whether the variance is zero - the smaller the variance, the more similar are the fixed and
random effects models. Of the methods available, we chose the DerSimonian and Laird method
[17]. Under the random effects model, the assumption of a common treatment effect is relaxed,
and the effect sizes are assumed to have a normal distribution with a given mean and variance.
The usual DerSimonian and Laird estimate of variance is given by
T
J-=Q(-(k-1)
nZ~
mraXlZ
ot
O
where 0 is the heterogeneity statistic, with the variance T set to zero if 0 < k - 1, and the
weights are calculated as in the inverse variance method. If the variance is zero, the weights
reduce to those given by the inverse variance method. If the variance is greater than zero, then
the weights in the random effects model will be smaller and more similar to each other than the
weights in the fixed effect model; this means that the random effects model will be more
conservative (the confidence intervals will be wider) than the fixed effect analyses since the
variance of the pooled effect is the inverse of the sum of the weights. In addition, the random
effects models give relatively more weight to smaller studies than the fixed effects model.
Like the inverse variance method, an advantage of the DerSimonian and Laird method is its wide
applicability.
It can be used to combine any type of estimates provided standard errors are
available.
3.2.4.
Meta-Analysis - Confidence Interval for Overall Effect
The confidence interval for the overall effect is given by
6-SEO}Q(1-La/2)
where 0 is the overall estimate and
to
6+SE{6}0(1-a/2)
) is the standard normal deviate.
3.2.5.
Meta-Analysis - Test Statistic for Overall Effect
A test statistic for the overall difference between groups is derived as
I
z 0
SE(6)
Under the null hypothesis that there is no treatment effect, Z will follow a standard normal
distribution.
3.2.6.
Meta-Analysis - Test Statistic of Homogeneity
For a formal test of homogeneity, the statistic
Q will follow
a chi-squared distribution on k - 1
degrees of freedom under the null hypothesis that the true treatment effect is the same for all data
sets being compared:
s
in1t
ott-Y
The Q-statistic provides descriptive information of between-study variation. Tests for
homogeneity can be underpowered, meaning a statistically nonsignificant result may be a falsenegative, i.e., between-study variation may be present but not detected by the test. This can be
somewhat compensated for by using a random-effects methods, which weigh the outcomes of the
study according to both within-study as well as the between-study variance.
We tested for statistically significant differences between eras using chi-square tests. We chose a
p-value < 0.05 for statistical significance. For the analyses we used Microsoft Excel 2007
(Microsoft Corporation, Seattle, WA).
3.3. Data - Cardiovascular Events
3.3.1.
Cardiovascular Events - Overview
The challenges of defining stent thrombosis in the absence of angiographic confirmation or
results on autopsy, particularly in long-term follow-up, are well-documented [1, 2, 4]. Moreover,
distinguishing stent thrombosis-associated MI from non-stent thrombosis-associated MI is
oftentimes not possible for many reasons, not the least of which is that diagnosis of stent
thrombosis requires catherization.
As such, after careful consideration of both the clinical
significance for patients, as well as the available evidence, rather than stent thrombosis as an
outcome measure, we instead chose MI and coronary heart disease (CHD)-mortality as indicative
of the overall safety and efficacy profile of DES and APT in treating patients with coronary artery
disease [I].
3.3.2.
Cardiovascular Events - Rate of Myocardial Infarction (MI) Incidence
3.3.2.1. Rate of MI Incidence - Overview
For estimates of the rate of MI incidence, we included published data on patients involved in the
clinical trials (a total of nine trials) used to support FDA approval of the two DES available in the
US [1]. In addition, since the application of DES has been extended to population of patients not
represented in these trials, we included additional evidence for these patients [2]. We conducted
meta-analyses to not only synthesize estimates from these studies, but also to extrapolate MI risk
beyond one year.
3.3.2.2. Rate of MI Incidence - Meta-Analysis
3.3.2.2.1.
Meta-Analysis - Study Selection
We selected two studies to estimate MI risk, one by Stone and another by Schomig [1, 2].
The study by Stone et al. was selected based on the following criteria: the inclusion of patients
with strictly on-label use of DES (single, previously untreated coronary lesions) as reflected in
the labels for sirolimus-eluting DES and paclitaxel-eluting DES that were approved by the Food
and Drug Administration; the length of follow-up (four years after device implantation; at the
time of this thesis, the longest follow-up publically available); the overall high-quality of the
study; and the authors of the study having obtained of databases for all four trials from Cordis
(manufacturer for the sirolimus-eluting DES) and Boston Scientific (manufacturer for the
paclitaxel-eluting DES). The latter criteria was considered important because these nine trials are
the only double-blind trials that compared each of the DES with bare-metal controls and also
served as the basis for the approval of the DES in the United States and Europe.
The study by Schomig et al. was selected for inclusion based on the following criteria: the
expansion of patients included in Stone (strict on-label use) to include patients in whom off-label
use occurred (estimated to be the majority of DES placement in daily clinical practice at the time
of this study); the length of follow-up (two years after device implantation; at the time of this
thesis, the second-longest follow-up publically available); and the overall high-quality of the
study.
Stone et al. performed a patient-level pooled analysis of data from nine double-blind trials - four
trials in which 1748 patients were randomly assigned to receive either sirolimus-eluting DES or
bare-metal stents, and five trials in which 3513 patients were randomly assigned to receive either
paclitaxel-eluting DES or bare-metal stents. Three trials were from the United States, two were
from Europe, two were global, and one was from Canada. Major clinical end points analyzed
included stent thrombosis and MI. The Breslow-Day test for heterogeneity demonstrated that
trials
involving
sirolimus-eluting
DES
and
paclitaxel-eluting
stents
were
sufficiently
homogeneous to justify the pooled analyses performed. The pooled results of the nine studies are
given in Table 1 [1].
Schomig et al. combined data from sixteen randomized trials of SES versus PES with a total of
8,695 patients in a meta-analysis.
Stone.
These trials were unique from the nine trials analyzed by
Clinical end points analyzed included stent thrombosis and MI.
No significant
heterogeneity was found across trials. While patient-level data could only be obtained from twothirds of the trials, the treatment effects on the patient- and population-levels are in accordance
with one another. All trials were open-label trials due to the impossibility of blinding different
devices from different manufacturers. Results from the pooled studies are shown in Figure 1 [2].
We conducted meta-analysis to not only synthesize estimates from these studies, but also to
extrapolate MI risk beyond one year, thereby considering variation both between and within
studies.
3.3.2.2.2.
Meta-Analysis - Data Extraction
A standard spreadsheet was used to collect the data from the studies. Data was extracted by one
reader (J.S.E.) and independently verified by two others (J.B.W., S.G.P.). Discrepancies were
resolved by discussion. Readers were not blinded to information about the authors, author
affiliation, and journal name. The extracted study characteristics included author, publication
year and number of patients. We extracted data from text, tables, graphs and web-based
supplemental appendices of the selected studies.
3.3.2.2.3.
Meta-Analysis - Data Conversion
Both Stone and Schomig reported cumulative percentages of MI by year after DES implantation.
The relevant time intervals applicable to the current study were greater than one year after DES
implantation. The study Stone provided four year follow-up data (i.e., years one-to-two, two-tothree, and three-to four after DES implantation). The study by Schomig provide two year followup data (i.e., years one-to-two after DES implantation). These data were extracted and then
converted to average annual event rates.
The conversion was done as follows with an illustrative example. From Stone, the cumulative
percent of MI for the time interval year two-to-three post DES implantation is reported to be 6%.
After extracting this data, we converted it to the probably of having MI (pMI):
pMI = (cumulative% / 100)
pMI = (6% / 100)= 0.06
Assuming binary outcomes (i.e., pMI + probability of not having an MI = I), we then calculated
the probability of not having an MI (pNoMI):
pNoMI= (I - pMI)
pNoMI = (I - 0.06) = 0.94
We then calculated the relative proportion of patients not having MI (relative) by dividing pNoMI
for each time interval by the pNoMI from the previous interval - for example, the pNoMI for
time interval two-to-three (pNoMIy2-3) by pNoMI for time interval one-to-two (pNoMlyl-2):
relative = (pNoMIy2-3 / pNoMIy l -2)
relative = (0.94 / 0.95)
0.989
The relative proportion was then converted into an annual event rate of having MI (rMI):
rMI = - ln(relative)/t
rMI = - In(0.989)/1 = 0.0 107
where In is the natural logarithm, and t is the time period in years (in this case one).
3.3.2.2.4.
Meta-Analysis - Meta-Analytic Methods
We combined the results from Stone and Schomig using both fixed effect (inverse variance) and
random effects methods and tested for heterogeneity. We also used these meta-analytic methods
to determine if, for the results from Stone, if the incident rate of MI varied significantly between
time intervals.
3.3.2.3. Rate of Myocardial Infarction (MI) Incidence - Additional Considerations
We assumed that all patients were receiving aspirin, thus the resulting annual incidence rate
represented patients who were receiving aspirin. We defined the MI rate in patients not treated
with APT as the
MI rate untreated
3.3.3.
MI rate with aspirin
(1 - efficacy of aspirin).
Cardiovascular Events - Rate of Myocardial Infarction (MI) Mortality
A single best study from Mauri et. al. was selected to estimate rate of MI mortality [4]. The study
by Mauri et. al. was selected because of its use of patient-level data from eight of the nine trials
used for FDA approval of the sirolimus and paclitaxel DES, all events being adjudicated by an
independent clinical-events committee (the Harvard Clinical Research Institute), the reporting of
events in a form suitable for inclusion in the model; and its overall high quality.
3.4. Data - Hemorrhage
3.4.1.
Hemorrhage - Definition
We also estimated bleeding risk.
Accurately estimating bleeding risk requires careful
consideration of many interrelated factors, including, but not limited to: how bleeding is defined
(e.g., definitions set forth by the Thrombolysis In Myocardial Infarction (TIMI) and the Global
Utilization of Streptokinase and Tissue Plasminogen Activator for Occluded Coronary Arteries
(GUSTO) trials); bleeding site (e.g., gastrointestinal, intracranial, aortic aneurysm, intraocular,
epistaxis or hemoptysis); patient subgroups (e.g., age-dependent incidence rates); and potentially
confounding variables (e.g., co-morbidities or medication effects). To best represent bleeding
risk from the data available, we defined severe bleeding as: fatal bleeding, bleeding requiring
transfusion, or intracranial.
3.4.2.
Hemorrhage - Bleeding Sites
We focused on bleeding sites which have the greatest impact on mortality, due to their
combination of frequency, risk of recurrence and excess mortality. By an order of magnitude,
gastrointestinal hemorrhage is the most frequent site of major bleeding, particularly as it related
to APT [10, 11]. When severe, it has a significant risk of recurrence and mortality. While
certainly less common than gastrointestinal hemorrhage, intracranial hemorrhage has a significant
risk of recurrence and high mortality [18].
We also defined a variable which represents a patient's propensity to bleed or thrombose called
"systemic risk".
It has been suggested that patients on DAT continuously without severe
bleeding may have passed a "bleeding stress test" [6]. These patients may have both a decreased
risk of bleeding while on Dual-Rx as well as an increased risk of thrombosis if taken off Dual-Rx.
For this variable, we defined a relative risk of one as average risk (neither increased risk of
bleeding nor thrombosis), greater than one as increased risk of bleeding, and less than one as an
increased risk of thrombosis.
3.5. Data - Antiplatelet Therapy
3.5.1.
Antiplatelet Therapy - Efficacy
We defined the efficacy of APT in preventing MI in terms of the annual MI rate with and without
APT, or the
efficacy of APT = I -
(RR of MI with APT)
(RR of MI without APT).
Thus, if APT has an efficacy of one, then the MI rate among patients receiving APT is zero; but if
APT has an efficacy of zero, then the MI rate is the same regardless of whether the patient has
received APT. The efficacy estimates for the included APT medications (aspirin and clopidogrel)
as secondary prevention of MI are summarized in Table 1 [3, 5, 6, 12].
For Dual-Rx, efficacy estimates are more complicated, including possible temporal variation. For
example, the efficacy of Dual-Rx increases over time, including greater than one-year post-DES
placement [7]. To determine if this increase in efficacy is statistically significant, we used similar
methods as described in section 3.2. (titled "Data - Cardiovascular Events"; please see above).
Namely, we extracted cumulative percentage of MI, converted these data to annual rates of MI
for each of the six-month time intervals reported, and using meta-analytic techniques, to
determine if there was statistically significant heterogeneity across time intervals.
Efficacy was then calculated by first converting annual rates of MI while receiving Dual-Rx or
control to annual probabilities, assuming the rate is constant over the year, by
p = 1 - exp(- r*t)
where p is the probability, r is the rate and t is the time period (in this case, one year).
The probability of MI while receiving Dual-Rx (pMId) or control (pMIc) were then used to
calculate efficacy (or the relative risk reduction):
(pMIc - pMId)/pMIc
3.6. Data - Antiplatelet Therapy - Risk
We also estimated the increased risk of gastrointestinal hemorrhage and intracranial hemorrhage
with APT. The risk estimates for aspirin and clopidogrel are well-defined in the literature and
summarized in Table 1 [3, 5, 6, 12]. For Dual-Rx, bleeding risk estimates are less well-defined.
For example, compared to aspirin monotherapy, Dual-Rx risk estimates range from no increased
risk [6], to a moderately increased risk [II], to more than a three times increased risk [10]. And
all estimates have wide confidence intervals. Given this uncertainty, we used wide ranges in
sensitivity analysis.
We assumed the bleeding risk for Dual-Rx was a multiplicative model
composed of the bleeding risks of aspirin and clopidogrel.
3.7. Decision Model
3.7.1.
Decision Model - Overview
Clinical decision-making, including decision modeling, has been identified as one of four core
content areas in the evolving subspecialty of clinical informatics, and is in a proposed curriculum
for clinical informatics fellowship [19, 20]. Decision modeling, including decision analysis,
Markov modeling, Monte Carlo simulation, comparative effectiveness, and other modeling
methodologies, have roots which reach to the very beginning of the scientific discipline of
biomedical informatics, having been adapted to the health care domain from other domains [13,
21-25]. The use of decision modeling has been and continues to be of value in informing
important decision-making on both population as well as individual patient levels, facilitating the
translation of an exponentially expanding biomedical knowledge base into actions which improve
human health [26-28].
We built of Markov state transition model [25, 29] using a standard computer program for
decision modeling (WinDM, Version 2009.6.1 (Pratt Medical Group, Boston, MA) [30, 31])
which compared several APT strategies composed of aspirin and clopidogrel, both as
monotherapy and in various clinically plausible combinations.
The model estimates life
expectancy for a hypothetical cohort of patients. All patients in the cohort are 65 years-old with a
past medical history significant for MI treated acutely with DES placement, then treated with
DAT continuously for one year without complications.
They have no history of intracranial
hemorrhage or gastrointestinal hemorrhage.
3.7.2.
Decision Model - Structure
The model is shown in Figure 1 and works as follows. Health states are represented as circles.
At the beginning of modeling, each patient in the cohort begins the simulation in the health state
called status-post DES (S/P DES) and is followed over time. The other health states are defined
by events which may occur in the course of the modeling: MI, intracranial hemorrhage,
gastrointestinal hemorrhage, any combination of these events, or death. The passage of time is
modeled as a series of cycles (in this case, the cycle length is I month). During each cycle, each
cohort member may remain in the same health state or transition to another (represented by
arrows between states). The model accounts for time lived by the cohort over the course of
modeling, and the simulation continues until all patients in the cohort have died (stopping criteria,
less than one patient remaining alive). The average life expectancy for a patient in the cohort is
determined by summing the life years lived by the cohort, then dividing by the number of patients
in the original cohort. We also performed a half-cycle correction.
3.7.3.
Decision Model - Assumptions
In addition to the assumptions inherent in choosing the model's structure, we made the following
additional assumptions:
1. We modeled only survival, MI, intracranial hemorrhage and gastrointestinal hemorrhage.
2.
At the beginning of modeling, patients have a history of MI (at the time DES of placement),
but no history of intracranial hemorrhage or gastrointestinal hemorrhage.
3. If MI, intracranial hemorrhage or gastrointestinal hemorrhage does not occur during
modeling, the incidence rates for these events remain constant throughout the course of the
modeling. Knowing that these rates may in reality change over time, we explored different
rates in sensitivity analysis.
4.
If MI, intracranial hemorrhage or gastrointestinal hemorrhage occur during modeling, the
incidence rates (rate of recurrence) increase, as is consistent with the respective natural
histories of MI, intracranial hemorrhage and gastrointestinal hemorrhage [18].
5. Demographic-related mortality rates, based on age and gender, and disease-specific excess
mortality rates were additive.
6.
Intracranial hemorrhage during modeling results in patients having all APT discontinued for
the remainder of modeling.
In contrast, patients who have gastrointestinal hemorrhage
during modeling are continued on the APT strategy to which they were allocated at the
beginning of modeling.
7. MI during modeling results in patients being started on DAT, if not already being received,
unless they have already had intracranial hemorrhage during modeling.
8. The efficacies and risks of different APT are constant throughout the course of the
modeling.
3.8. Sensitivity Analysis
To further manage complexity, uncertainty, and potential inaccuracy in baseline estimates and
assumptions, we performed extensive structural and deterministic sensitivity analyses. For the
latter, the baseline values of key variables are varied over a clinically plausible range to determine
to what extent the life expectancy of each APT strategy changes.
When available, 95%
confidence intervals (statistically plausible range) guided the defining of clinically plausible
ranges. When 95% confidence intervals were not available, we used expert opinion to define
clinically plausible ranges.
4.RESULTS
4.1. Meta-Analyses
4.1.1.
Rate of Myocardial Infarction Incidence
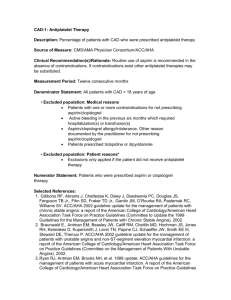
The rates of myocardial infarction (MI) incidence for various yearly time intervals after drugeluting stent (DES) implantation are shown in Table 2, along with the 95% CIs. Rates are
calculated from data extracted from studied by Stone et al. and Schomig et al. where indicated.
The results of meta-analyses of rates of MI are shown in Table 3. The estimated rate of MI
resulting from combining rates from the studies by Stone et al. and Schomig et al. (i.e., from each
study, year 1-2 after DES implantation) was 0.0106 (95% CI, 0.00722 to 0.0140). The test for
heterogeneity showed that the rates were not statistically significantly different, with a p-value
=
0.98. The estimated rate of MI resulting from combining rates from the study by Stone et al.
from different time intervals (i.e., from Stone et al., year 1-2, year 2-3, and year 3-4) was 0.00963
(95% CI, 0.00666 to 0.0 126). The test for heterogeneity showed that the rates were not
statistically significantly different, with a p-value = 0.76.
In both cases, since heterogeneity was not found, the random effects model reduces to the fixed
effect model (i.e., the estimate rate for the fixed effect and random effects models are equal).
4.1.2.
Efficacy of Dual-Antiplatelet Therapy
The rates of myocardial infarction (MI) for various six-month time intervals after DES
implantation while receiving either Dual-Rx or control are shown in Table 4, along with 95% CIs.
All rates are calculated from data extracted from Eisenstein et al. For months 6-12: the rate of MI
while receiving Dual-Rx was 0.0 120 (95% CI, 0.00331 to 0.0208); the rate of MI while receiving
control was 0.0181 (95% CI, 0.00549 to 0.0307); the p-value was 0.44; and the efficacy is 0.33.
For months 12-18: the rate of MI while receiving Dual-Rx was 0.0162 (95% CI, 0.00592 to
0.0264); the rate of MI while receiving control was 0.0285 (95% CI, 0.0 124 to 0.0445); the pvalue was 0.21; and the efficacy is 0.43. For months 12-18: the rate of MI while receiving DualRx was 0.0 122 (95% CI, 0.000 to 0.0250); the rate of MI while receiving control was 0.0414
(95% CI, 0.0142 to 0.0686); the p-value was 0.057; and the efficacy is 0.70.
The results of meta-analyses of rates of MI while receiving either Dual-Rx or control are shown
in Table 5. After combining rates of MI from different time intervals while receiving Dual-Rx
(i.e., month 6-12, month 12-18, and month 18-24) the estimate rate of MI while receiving DualRx was 0.0134 (95% CI, 0.00754 to 0.0 193). The test for heterogeneity showed that the rates
were not statistically significantly different, with a p-value = 0.82. After combining rates of MI
from different time intervals while receiving control (i.e., month 6-12, month 12-18, and month
18-24) the estimate rate of MI were different for the fixed effect model (0.0243 (95% CI, 0.0150
to 0.0336)) than the random effects model (0.0254 (0.0140 to 0.0368)). The test for heterogeneity
showed that the rates were not statistically significantly different, with a p-value = 0.26.
For Dual-Rx, since heterogeneity was not found, the random effects model reduces to the fixed
effect model (i.e., the estimate rate for the fixed effect and random effects models are equal). For
control, heterogeneity is suggested by the p-value which approaches statistical significance. The
fixed effect and random effects models yield slightly different estimates (fixed effect = 0.0243;
random effects = 0.0254).
This trend was also reflected in the calculated efficacy of Dual-Rx for various six-month time
intervals after DES implantation, as shown in Table 5. For months 6-12, the efficacy is 0.33. For
months 12-18, the efficacy is 0.43. And for months 18-24, the efficacy is 0.70. The overall
efficacy is 0.47. The range of efficacies was quite wide across time intervals. Given this, and the
challenges inherent in temporal representation of data, we explored alternative assumptions and
hypotheses in wide ranges during sensitivity analysis. For our base-case estimates, we drew on
supplemental evidence that the baseline efficacy of Dual-Rx as secondary prevention of MI is the
sum of its constituents [6]. This value approximates both the efficacy during the 12-18 month
time-period and the overall estimate.
4.2. Decision Modeling
4.2.1.
Base-Case Analysis
The baseline values for input into the decision model are shown in Table 7. The results of the
baseline analysis are summarized in Table 8. The APT strategy Dual-Rx indefinitely yielded a
life expectancy of 13.48 years.
Clopidogrel indefinitely yielded 13.45 years.
Dual-Rx
indefinitely modestly increased life expectancy by 1.44 months compared to no APT, and 0.72
months compared to aspirin indefinitely.
Under these circumstances, when the difference in
value between two or more therapeutic approaches is so close that none are clearly preferable, the
decision is considered a "toss up", or "close call" [32].
4.2.2.
Sensitivity Analysis
Figure 3 shows a one-way sensitivity analysis of the efficacy of clopidogrel to prevent MI. The
horizontal axis shows the efficacy of clopidogrel, and the vertical axis shows the life expectancy
in years.
Each line on the graph represents an APT strategy (including those labeled "DAT
Indefinitely" and "Aspirin Indefinitely"). For each efficacy value, the preferred strategy is
represented by the line that is highest on the graph. A portion of the 95% CI for the variable is
represented as a bracket near the x-axis. Where two lines intersect is called a threshold. For
efficacy values greater than the threshold, one strategy is preferred, and for values less than the
threshold, the other strategy is preferred. If a threshold is not found, then the analysis is termed
insensitive to that parameter. If a threshold is found and is particularly close to the baseline
value, the analysis is sensitive to that variable. Figure 3 shows the threshold is 0.09, well below
not just the baseline value but also the lower limit of the 95% confidence interval.
Figure 4 shows a one-way sensitivity analysis of the relative risk of severe gastrointestinal
hemorrhage with clopidogrel.
While, at baseline (2.01), DAT indefinitely is the preferred
strategy, the threshold value (3.33) is well within the 95% confidence interval (as indicated near
the x-axis).
5.DISCUSSION
5.1. Overview
We evaluated the long-term prevention of myocardial infarction and death with antiplatelet
therapy in patients with drug-eluting coronary stents (DES) greater than one year post-DES
placement. Our analysis indicates that three antiplatelet strategies yield similar life expectancy Aspirin monotherapy indefinitely, Clopidogrel monotherapy indefinitely, and Dual-Antiplatelet
therapy indefinitely.
Compared to placebo, Dual-Rx indefinitely (unless the patient experiences
hemorrhage) increases life expectancy modestly (about 1.5 months).
intracranial
In this comparison, the
mortality risk of intracranial hemorrhage or gastrointestinal hemorrhage is outweighed by the
mortality benefit of Dual-Rx as secondary prevention of MI. For perspective, this gain in life
expectancy approaches that of other accepted medical interventions for a similar target population
(patients who have survived an acute MI) when compared to placebo. For example, beta-blocker
therapy increases life expectancy by 5.6 months for patients with a high risk of recurrence. And
revascularization with coronary-artery bypass grafting increases life expectancy by 1-7 months
for patients with one vessel disease, and 0-8 months for patients with two-vessel disease [33].
While the current study's baseline estimates for rates of MI, intracranial hemorrhage,
gastrointestinal hemorrhage and death, as well as efficacy and risk of APT (Table 1) included a
broad range of patient populations that represents clinical practice, and we explored different
assumptions in extensive sensitivity analysis, we have purposely designed the model structure to
be generalizable to a variety of patient sub-populations, with a flexible structure that is suitable
for future analyses that focus on specific subgroups: patients with off-label use of drug-eluting
stents or multiple stents; women; or the elderly; and many others with varying risks of MI and/or
severe bleeding.
5.2.Limitations
Our study has several limitations.
We used study-level and synthesis-level data from each
published data source, so our projections may be more precise with individual patient-level data.
We also made lifetime projections of outcomes which require assumptions based on the best
evidence at the time our model was built. Additional evidence and scientific understanding in
this rapidly evolving area may require adjustment in our analyses. For our meta-analyses, while
we carefully chose our methods and primary data sets, no meta-analysis can compensate if the
primary data contain bias - either publication bias or bias from poor study design and execution.
And while we conducted extensive structural and deterministic sensitivity analysis, we did not
conduct probabilistic sensitivity analysis.
5.3.Comparison with Other Studies
The findings of this analysis are consistent with a trial published in 2010 [34]. However, this trial
may have been underpowered to see an effect, only examined the 12 to 24 month period postDES placement, and, by the authors own conclusions, should be confirmed through larger,
randomized clinical trials with longer-term follow-up [34, 35].
Such a trial to address the
question of optimal type and duration APT for patients greater than one-year post-DES placement
is planned.
Until results from larger trials are available, models like the current analysis can inform important
patient-level and policy-level decisions with regard to ongoing management decisions in a
number of ways.
For example, in other areas of medicine, such as HIV and hyperlipidemia,
comparison of models with new and ongoing clinical trials has led to deepening our
understanding of these health conditions. And in absence of trials, models have been compared
with other independently-developed models (lending convergence validity), as demonstrated by
collaborations such as the U.S. National Institute of Health's and National Cancer Institute's
Cancer Intervention and Surveillance Modeling Network [36].
5.4. Future Directions
Future directions for the current work is to refine and validate the model, then implement results
to inform health policy and routine clinical practice. There are long-standing and numerous ways
comparative effectiveness studies like the current study can inform policy as well as be
implemented into routine clinical practice [37]. These have taken the form of clinical practice
guidelines, clinical algorithms, clinical balance sheets, and decision aids [28, 38-40].
One example of successful implementation of clinical practice guidelines related to anti-platelet
therapy and DES is that of primary percutaneous coronary intervention.
Several keys to
successful implementation have included providing local institutions several core strategies that
define high-quality care, but giving substantial latitude in determining the best method of local
application of the strategies.
In general, implementation research has demonstrated that
approaches which take into account local constraints, infrastructure, and practice patterns are
more likely to be successful. While sometimes requiring fundamental changes within complex
clinical systems, evidence is emerging on effective practices, including a collaborative teambased approach and data-monitoring systems with prompt, effective feedback on performance
[41, 42].
Many of these principles and strategies for efficiently and successfully implementing into routine
clinical practice the findings from comparative effectiveness and other evidence-based, outcomes,
and health services research is the Department Veterans Affairs (VA)'s Quality Enhancement
Research Initiative (QuERI) [41].
QuERI was launched in 1998 by the VA's Health Services Research and Development Service as
a part of a system-wide transformation aimed at improving the quality and outcomes of healthcare
for Veterans by implementing evidence-based clinical research findings into routine clinical
practice. QuERI is organized into centers, each of which focuses on a condition that is either
common among Veterans or places a high burden on patients, family members, and the VA
healthcare system [43].
A QuERI center applicable to long-term antiplatelet therapy in patients with DES is the Ischemic
Heart Disease (IHD) QuERI, whose mission is to improve the quality of care and health outcomes
of Veterans with IHD by enabling implementation of best practices (e.g., guideline-indicated
therapies) in acute care, chronic illness care, and secondary prevention [44]. Data resulting from
IHD-QuERI analyses have provided additional evidence regarding the risk of stent thrombosis for
DES for patients taking and not taking clopidogrel [45].
Follow-up studies for the current study may include collaboration with the IHD-QuERI, along
with the QuERI which includes data on intracranial hemorrhage (i.e., Stroke QuERI) [46, 47].
Currently, there is not a QuERI focused on gastrointestinal hemorrhage, but this may be created.
Data can be collected from the IHD-QuERI (Table 9) and Stroke QuERI databases, as well as
VistA via Bayesian longitudinal histories [48]. These data can be synthesized in a multimodeling approach [49]. Risk factors for MI, major hemorrhage, and potential discordance with
a patient's overall MI/hemorrhage risk profile and her/his APT regimen can be identified. This
information would serve as screening and early detection of areas for optimizing a patient's APT
and care.
6.REFERENCES
1.
Stone, G.W., et al., Safety and efficacy ofsirolimus- andpaclitaxel-elutingcoronary
stents. N Engi J Med, 2007. 356(10): p. 998-1008.
2.
Schomig, A., et al., A ineta-analysis of 16 randomized trialsof sirolimus-elutingstents
versus paclitaxel-elutingstents in patientswith coronary artery disease. J Am Coll
Cardiol, 2007. 50(14): p. 1373-80.
3.
Becker, R.C., et al., The primary and secondaryprevention of coronaryartery disease:
American College of Chest PhysiciansEvidence-Based ClinicalPractice Guidelines (8th
Edition). Chest, 2008. 133(6 Suppl): p. 776S-814S.
4.
Mauri, L., et al., Stent thrombosis in randomizedclinical trials of drug-eluting stents. N
Engl J Med, 2007. 356(10): p. 1020-9.
5.
A randomised,blinded, trial of clopidogrel versus aspirin in patients at risk of ischaemic
events (CAPRIE). The Lancet, 1996. 348(9038): p. 1329-1339.
6.
Bhatt, D.L., et al., Patientswith prior myocardial infarction,stroke, or symptomatic
peripheralarterialdisease in the CHARISMA trial.J Am Coll Cardiol, 2007. 49(19): p.
1982-8.
7.
Eisenstein, E.L., et al., Clopidogrel use and long-term clinical outcomes after drugeluting stent implantation.Jama, 2007. 297(2): p. 159-68.
8.
Kushner, F.G., et al., 2009 Focused Updates:ACC/AL4 Guidelinesfor the Management
of Patients With ST-Elevation MyocardialInfarction (updatingthe 2004 Guideline and
2007 Focused Update) andACC/AHA/SCAI Guidelines on PercutaneousCoronary
Intervention (updating the 2005 Guideline and 2007 Focused Update): a reportof the
American College of Cardiology Foundation/AmericanHeartAssociation Task Force on
Practice Guidelines.Circulation, 2009. 120(22): p. 2271-306.
9.
Grines, C.L., et al., Prevention ofpremature discontinuationof dual antiplatelettherapy
in patients with coronary arterystents: A science advisoryfrom the American Heart
Association, American College of Cardiology,Society for CardiovascularAngiography
and Interventions, American College of Surgeons, and American DentalAssociation,
with representationfrom the American College of Physicians. J Am Dent Assoc, 2007.
138(5): p. 652-655.
10.
Hal las, J., et al., Use of single and combined antithrombotic therapy and risk ofserious
upper gastrointestinalbleeding: population based case-controlstudy. BMJ, 2006.
333(7571): p. 726-.
11.
Buresly, K., et al., Bleeding complications associatedwith combinations of aspirin,
thienopyridinederivatives, and warfarin in elderly patientsfollowing acute myocardial
infarction. Arch Intern Med, 2005. 165(7): p. 784-9.
12.
Baigent, C., et al., Aspirin in the primary and secondaryprevention of vascular disease:
collaborativemeta-analysisof individualparticipantdatafrom randomisedtrials.
Lancet, 2009. 373(9678): p. 1849-60.
13.
Pauker, S.G. and J.P. Kassirer, Decision analysis. N Engl J Med, 1987. 316(5): p. 250-8.
14.
Hunink, M.G., P., Siegal, J. Weeks, J. Pliskin, J. Elstein, A. Weinstein, M., Decision
making in health and medicine: integratingevidence and values. 2001, Cambridge:
Cambridge University Press.
15.
Egger, M., G. Smith, and D. Altman, Systematic Reviews in Health Care: Meta-Analysis
in Context. 2001, London: BMJ Publishing Group.
16.
Higgins, J. and S. Green. Cochrane Handbookfor Systematic Reviews of Interventions.
2009 [cited Version 5.0.2 [updated September 2009]; Available from: www.cochranehandbook.org.
17.
DerSimonian, R. and N. Laird, Meta-analysis in clinical trials. Control Clin Trials, 1986.
7(3): p. 177-88.
18.
Renee, B.V.S., PrimaryIntracerebralHemorrhage: NaturalHistory,Prognosis,and
Outcomes. 2005. 5(3): p. 163-167.
19.
Safran, C., et al., ProgramRequirementsfor FellowshipEducation in the Subspecialty of
ClinicalInformatics. Journal of the American Medical Informatics Association. 16(2): p.
158-166.
20.
Gardner, R.M., et al., Core Contentfor the Subspecialty of ClinicalInformatics. Journal
of the American Medical Informatics Association. 16(2): p. 153-157.
21.
RL Keeney, H.R., Decisions with Multiple Objectives: Preferencesand Value Tradeoffs.
1976, New York, NY: John Wiley & Sons.
22.
Shortliffe, E.H. and J.J. Cimino, Biomedical Informatics: Computer Applications in
Health Care and Biomedicine. Third ed. 2006, New York, NY: Springer.
23.
Keeney, R. and H. Raiffa, Decisions with Multiple Objectives: Preferencesand Value
Tradeoffs. 1976, New York, NY: John Wiley & Sons.
24.
Barnett, G.O., Computers in patient care.N Engl J Med, 1968. 279(24): p. 1321-7.
25.
Beck, J.R. and S.G. Pauker, The Markov process in medicalprognosis. Med Decis
Making, 1983. 3(4): p. 419-458.
26.
Weinstein, M.C., et al., Principlesof good practicefor decision analytic modeling in
health-care evaluation: reportof the ISPOR Task Force on Good Research Practices-Modeling Studies. Value Health, 2003. 6(1): p. 9-17.
27.
Briggs, A., K. Claxton, and M. Sculpher, Decision Modellingfor Health Economic
Evaluation. 2006, Oxford: Oxford University Press.
28.
Hunink, M. and P. Glasziou, Decision making in health and medicine: integrating
evidence and values. 2001, Cambridge, UK: Cambridge University Press.
29.
Sonnenberg, F.A. and J.R. Beck, Markov models in medical decision making: a practical
guide. Med Decis Making, 1993. 13(4): p. 322-38.
30.
Pauker, S.G., et al., Clinicaldecision analysis by personalcomputer. Arch Intern Med,
1981. 141(13): p. 1831-7.
31.
Lau, J., J.P. Kassirer, and S.G. Pauker, Decision Maker 3.0. Improved decision analysis
by personalcomputer. Med Decis Making, 1983. 3(1): p. 39-43.
32.
Kassirer, J.P., J.B. Wong, and R.I. Kopelman, Learning ClinicalReasoning. 2010,
Baltimore: Lippincott Williams & Wilkins.
33.
Wright, J.C. and M.C. Weinstein, Gains in life expectancyfrom medical interventions-standardizingdata on outcomes. N EngI J Med, 1998. 339(6): p. 380-6.
34.
Park, S.J., et al., Duration of dual antiplatelettherapy after implantationof drug-eluting
stents. N Engl J Med, 2010. 362(15): p. 1374-82.
35.
Berger, P.B., Optimal duration of clopidogrel use after implantation of drug-eluting
stents--still in doubt. N Engl J Med, 2010. 362(15): p. 1441-3.
36.
Cancer Intervention and Surveillance Modeling Network: Modeling to guide public
health research andpriorities. 2010 30 Jun 2010 [cited 2010 July 15]; Available from:
http://cisnet.cancer.gov/.
37.
Ratner, R., et al., Institute of Medicine. Initial nationalprioritiesfor comparative
effectiveness research.2009, National Academies Pr: Washington, DC.
38.
Pauker, S.P. and S.G. Pauker, The amniocentesis decision: an explicit guidefor parents.
Birth Defects Orig Artic Ser, 1979. 15(5C): p. 289-324.
39.
Eckman, M.H., et al., Making decisions about antithrombotictherapy in heartdisease:
decision analytic and cost-effectiveness issues. Chest, 1998. 114(5 Suppl): p. 699S-714S.
40.
Pauker, S.G. and S.P. Pauker, Prescriptivemodels to supportdecision making in
genetics. Birth Defects Orig Artic Ser, 1987. 23(2): p. 279-96.
41.
Naik, A.D. and L.A. Petersen, The neglectedpurpose of comparative-effectiveness
research.N Engl J Med, 2009. 360(19): p. 1929-3 1.
42.
Nallamothu, B.K., E.H. Bradley, and H.M. Krumholz, Time to treatment in primary
percutaneous coronary intervention. N Engl J Med, 2007. 357(16): p. 1631-8.
43.
QUERI: Quality EnhancementResearch Initiative. 2010 July 6, 2010 [cited 2010 July
10]; Available from: http://www.queri.research.va.gov/default.cfim.
44.
Ischemic HeartDisease (IHD) Quality Enhancement Research Initiative. 2010 June 14,
2010 [cited 2010 July 10]; Available from:
http://www.queri.research.va.gov/ihd/default.cfm.
45.
Ho, P.M., et al., Clopidogrel and long-term outcomes after stent implantationforacute
coronarysyndrome. Am Heart J, 2007. 154(5): p. 846-51.
46.
Williams, L.S. and R.L. Roudebush. Stroke QUERIStrageticPlan 2008. 2008 December
2008 [cited 2010 July 16]; Available from:
http://www.queri.research.va.gov/about/strategicplans/str.pdf.
47.
Ischemic HeartDisease IHD Cube Manual. June 4, 2010 [cited 2010 July 16]; Available
from:
http://www.visn20.med.va.gov/V20/DataWarehouse/Documents/OLAPMetaData.asp#de
fs.
48.
Reis, B.Y., I.S. Kohane, and K.D. Mandl, Longitudinal histories as predictors offuture
diagnoses of domestic abuse: modelling study. Bmj, 2009. 339(339): p. b3677.
49.
Tsafnat, G. and E.W. Coiera, Computationalreasoningacross multiple models. J Am
Med Inform Assoc, 2009. 16(6): p. 768-74.
7.APPENDICES
7.1. Appendix A: List of Abbreviations
Antiplatelet therapy..........................
Drug-eluting stent(s)........................
Dual-antiplatelet therapy..................
Life expectancy.............................
Myocardial infarction...................
Veterans Administration..............
Veterans Health Administration......
APT
DES
Dual-Rx
LE
MI
VA
VHA
7.2. Appendix B: List of Tables
Table 1: Clinical outcomes at four years (complete results, all pre-specified intervals).
Table 2: Rates of myocardial infarction for various yearly time intervals after drug-eluting stent
implantation.
Table 3: Results of meta-analyses of rates of myocardial infarction.
Table 4: Rate of myocardial infarction for various six-month time intervals while receiving either
dual-antiplatelet therapy or control.
Table 5: Results of meta-analyses of rates of myocardial infarction while receiving either dualantiplatelet therapy or control.
Table 6: Calculated efficacy of dual-antiplatelet therapy.
Table 7: Base-case values. Panel A, event probabilities; Panel B, medication risk and efficacy.
Table 8: Base-case analysis.
Table 9: Ischemic heart disease cube measures.
7.3. Appendix C: List of Figures
Figure 1: Analysis of myocardial infarction according to the drug-eluting stent type.
Figure 2: Markov state transition model.
Figure 3: One-way sensitivity analysis varying the value of the variable efficacy of clopidogrel to
prevent myocardial infarction.
Figure 4: One-way sensitivity analysis varying the value of the variable clopidogrel risk
associated with severe gastrointestinal hemorrhage.
mrin-arler.
1 year
o)
1.3% (11)
33 days - 1 year
p22)
6 4%(ii)
0.0% (0)7
3.)
:)
.21)
.. o43)
40.3%
o (
-5
6.6% i55)
1.1%o (17)
63
(5)
.6%P
0
2.5%
at intarction, -
,
6 115 1)
0
7
05%(0)
(0
4
(11
'9)2
0 23
2.2 o(19)
44'o(37
0.0% ()l
i7'o(221
]
2]
£96].
3
1 29 (.68, 2.42]
4 ]
0.91 (.7
0.57 [C7. 2C]
i1]
' !0 [26 06]
1 0' [t 71
in
13 ' [C60
L27 '(.74
71
0.43
-
009
)
3.6o% (491
33 u
0.01AL
(0:
10Pa(81 )
1 -? [0:-
'17%'
0 3
036
1.3I [0'73B]
(01)
C. 1.93]
0.99 [
0.3%* (3)
2.3% o(16)
001, (2
0- 0 (73)
La
4016
4-5o(5
0.96
13.6]
040
2Aio34)
[005,
5L2.118]
0 39
0 .9
12 61
60110O
6 L o1S6)
Q*0(
170 .2Q;
28 [0.73 2.2]
(3)
]J
]
0
0
1.2 1 (
96 1 5
032
166 C-60 4.56]
037
12 '(.79. 87]
86 .
2
0.99 [0.05, l5iS6]
12'
(1
393
0.25
[3.6K3]
[0.4:'35.62]
2.0
[05%0 Cl|*
jtrg stent
2.6%o(22(
0.1t
4.60' (3c)
0.7% (6
5.2%(44)
0.1% (1)
)3(4t)
0.00
0 .50
0.10
0. 6% ( )
(N=378)
0 - 30 days
33 days - 4 years
lvlyccard
1 year - 4 years
33 days -
3D days - 4 years
0 - 30 days
IHeath.
1 year - 4 years
3D days - 1 year
33 days - 4 years
Death, cardiac
0-30 days
33 days - 1 year
1 year - 4 years
'33 day - 4 year s
0 - 30 days
Death, all :aLse
1 year - 4 years
3Ddays - I year
3D days - 4 years
0 - 30 days
Stent thrombosis
(N=870)
vauat
P
11~ 184.
21 -03}
(y
1.3%
(31:
C
6 '(l")
I1
0.60 (11)
(3l0, (39
3
1.8% i22:
C3% (1
0.O%(5)
(42'
3.%
43% (61'
[J68 1. 49
[162. 1 34
0. '5 [3.21, 0.851
0.91
1.20 [.84 1. 721
1I97
[ri 1 1 0'
106[3R-
0.
1.19[53 2.65
(01
1 01 [I 6x 1 497
P
0.90
0.74
0.7
0.14
099
0,6
G.0 S'
ValueoI
L[ 1.
D[1,9 . 2. 07:
[16' 1.377
L73]
[18. 1.47
0-37 [11. 1 s3
0.96 [33 1 7]
0.92
0,16
0_96
100 [5
0.97 [r7o 131
1501(25:
('-0 [2)0S,
02% (5'
.07]
(±.94 [1/'0, 1 261
4 54[0-98
1(7]
[3 98. 9.1-
201 [0.3
03s
.80 [131 2.0S4_
14
6.3% (87,
6.6% (92.
0.0 (1-
06% (131,
U.5%
(114:
(N=1,78)
[05% Cl]'
Hazard ratio
-,
-U)
0
Co
-h
0.
CD
-o
(DQ
-3 (/)O
o0
0 0
Hazard ratin
Dare ntal
stAent
Eare meia
stent
S roliimteittng steft
0:-n
11.Clinical Outcomes at 4 Years (complete results, all pre-specified intervals)
(D0
1 yo0r1- a1 yar(
ii
.
e ar
iJ)11,0
yeCA
61% (1)
L6% 14)
74f)
0.%o7]
2 82% 0)
t#2
i0)
00
(2-1
8)
S%
10]
.)
3]
49]
46]
I 12 [0.
-_59]
7
]
1
.71]
'3
[1 16]
.
L7 [0.77 48]
1.')
(0)
f
5 C%(4)
1
0.4-1
0_44
09
0 07
0.16
0.99
.59
0.56
90
11)
19%6)
12.40
.1
127)
2)
14%n7o
2.6%!
140o> 9
18%
17
0!'
0.69
-
-39]
I9)
1-1 -5
0.67'.
S.90
() o
0
(19
)
0
o0
(29)
5%
(136)
i%(68)
1%
7 0% (97)
0.6o (11)
7.
7
6.5% (84)
9( 274
9.2' 1 -(4
3. 1 (4
3.3%()
11 8 1U
3
I 6
70 cS(48)
% :0900
0%
1 45 [8.7
1
(13)
38 [6
'000
28
49]
IT
[6S3
LT7
1.03 [3.1 1. 30
0. 99 [71 1)9']
[
129
0.82 [334 .L)1
1.0.2 [377 L >
1.11 [167 LS3
099[
1.08 [1.80 9 46]
045([.74 LD2]
_1)
4.
1.3F
0.70 ['.46 L 36]
11
L
0i
71:
0
0.82
0-66
0.l0
69
0
0_60
0_067
0
079D
00.
0.73 [3.17 111
184
09,(
0- 1
_17
106
0
42' ] -
1.23 [
1.0 [394 L26'
0
)3)
1 02[176 13
38[336111
90.3 6
.55c/)
-. 34[61
15[173
[J.3
1.00(3 [1
1 30 [3.69 245
-a-ak
0
One
0.381 540u >oT r~(8
0.9 [3 J67 L'57 0. 7t
0.03
OJS 33 03'
-4j
_1
52% 67
.8% 32)
S.9% 09)
.%(9)
U3(131)
7.1% .9C)
) [0f1 9] 0,4
0.
0.13
035
0.39
0.14
1O0j0.71 41]
0.86 9.1% (127)
[1) .7- .4!i' C.:±
:zlo
(17
0.51
2.2%8
49]
),2 [0.45.
117 [0.81
(c
1.0
2
10
1.[091. 16]
348 [0.7.16 74]
S
L12 [0S4
1.27 [0.69
2_0'o( 1oW .5ok
14
63 0(53)
13% ( 17
0.2% (20
6o40
6. 30(3)
2.%
4[0P
1 22 [0.69
'0f
XS1 [0. 17.' .11]
. 99]
[097. 36]
1 09 [03
038
1.11 [0.13. 1.]
(3)
(8(11)
.8(II
8
yeat- 4 yeji
.20 f-4
3 4.
o
1.27 -0.91.]
0-30c
4. 1'o .3o
3Io (45)
1.19 [3.80
0
Ta ia x
w'' wae:e x th efi Kap's,Jil fer t t,- eI
Idi Vi :Ile aceItua1 nIun11ber ofIt [7nt [NIt;i eve11c
a"n iiirer".4. CI conifidence interval. :Thtimate LakCulted from11 a Co pr JAOPoIio.nal hazard.s model: 'I 2-sided k)2oa-'nK oi -exact
patient hiad t1x4- tueiu uauumbus' v, cnom. outI loefcu- I :!l Lul woa1c el I~t 1Y21
i
I
[2 y
X) doys:- 4 years
Carl ac death cr myocarrlva
I year- 4
0 - 30 lys
30days -4 yars
30daysf- 1 eu
lnlarclion
1year- 4 yCas
or O-wave iucaoidlinfulcUu
Deudo
740
2
2.3%
30 days - 4 years9%
1ycar
17.4C
-()
(28)
1100) LO.4 (0 )
.6%, i23)
11%o (A)
160
30dcys
D[-oth or rnyc'cordial infarchon
0 - 30 Lays
I year- 4 ytrs
(17)
I ro
0 7%
2.1,
.3
1 year
1.
16)
r43
6
0.6%): (5)
2.8 9)
8
L8%
4.5
- 30 days
non-C-Wave
(23[077]
.1
7)
01
A(t 7)
0.'
199 [0.29. 342]
0.99
067
0.oc (So
12%o)U
ear
I I')
[_412
1 s 4
0.6%66
0Ac(7)
(A%(7)
49.46]
009
[0.7
z96
0-1C (1)
f6
d
1. P0 (17
0.7
04
22
1.4%
-]
0.19
6
1 4[0.77.3.47]
1 3 o(
8[
2.1% (18)
30days - I years
30 diys -
0
Myocardial ifarcti.
' days - I year
0 - 30 days
30days-4years
I year - 4 yrs
Myocard il inifarction 0-wave
CD
CD
(D
0rl h i'taer scurdxa
(
0-
3
0
0
(Do0
0
Table 2: Rates of myocardial infarction for various yearly
time intervals after drug-eluting stent implantation.
All time intervals are from Stone, 2007 [1] or Schomig, 2007
[2] where indicated. Abbreviation: Cl = Confidence Interval.
Study, time interval
within study
Incident rate (95% CI)
Stone, year 1-2
0.0107 (0.00448 to 0.0169)
Stone, year 2-3
0.0106 (0.00549 to 0.0158)
Stone, year 3-4
0.00839 (0.00394 to 0.0128)
Schomig, year 1-2
0.0106 (0.00652 to 0.0146)
Table 3: Results of meta-analyses of rates of myocardial infarction.
All time intervals are from Stone, 2007 [1] or Schomig, 2007 [2] where indicated. The
random effects model reduced to the fixed effect model (i.e., the estimated rate for the
fixed and random effects models are equal. Abbreviations: CI = Confidence Intervals; IV
= Inverse Variance; DL = DerSimonian and Laird.
Study, time interval within
study, method
Estimated rate (95% CI)
Test for heterogeneity
0.00963 (0.00666 to 0.0126)
X2
= 0.54, P = 0.76
0.0106 (0.00722 to 0.0140)
X2
= 0.00089, P = 0.98
Stone: year 1-2;
year 2-3; year 3-4
Fixed effect (IV)
Random effects (DL)
Stone, year 1-2;
Schomig, year 1-2
Fixed effect (IV)
Random effects (DL)
Table 4: Rate of myocardial infarction for various six-month time intervals while
receiving either dual-anti platelet therapy or control.
All time intervals are from Eisenstein, 2007 . Abbreviations: D = Dual-Antiplatelet
Therapy; C = Control; Cl = Confidence Interval.
Six-month time
interval within study
Incident rate (95% Cl)
C
D
Test for
heterogeneity
Months 6-12
0.0120
(0.00331 to 0.0208)
0.0181
(0.00549 to 0.0307)
X2= 0.60,
P = 0.44
Months 12-18
0.0162
(0.00592 to 0.0264)
0.0285
(0.0124 to 0.0445)
X2= 1.61,
P = 0.21
Months 18-24
0.0122
(0.000 to 0.0250)
0.0414
(0.0142 to 0.0686)
X2 =3.61,
P = 0.057
Table 5: Results of meta-analyses of rates of myocardial infarction while
receiving either dual-anti platelet therapy or control.
All time intervals are from Eisenstein, 2007 [7].
Since the test for heterogeneity was not found, the random effects model reduces to
the fixed effect model (i.e., the estimated rate for the Fixed and Random effects
models are equal.
Abbreviations: Cl = Confidence Intervals; D = Dual-Antiplatelet Therapy; C = Control;
IV = Inverse Variance; DL = DerSimonian and Laird.
Method
Estimated rate (95% CI)
Test for
heterogeneity
Months 6-12, months 1218, month 18-24
Fixed effect (IV)
Random effects (DL)
0.0134 (0.00754 to 0.0193)
X2
Eisenstein, C (month 612, month 12-18, month
18-24)
Fixed effect (IV)
Random effects (DL)
0.0243 (0.0150 to 0.0336)
0.0254 (0.0140 to 0.0368)
X2 =2.71, P = 0.26
Table 6: Calculated efficacy of
dual-antiplatelet therapy.
All time intervals are from Eisenstein,
2007 [7].
Six-month time
interval within study
Efficacy
Months 6-12
0.33
Months 12-18
0.43
Months 18-24
0.70
Overall
0.47
=
0.41, P = 0.82
Table 7: Base-case values. Panel A, event
probabilities.
Values are average annual except where noted.
Abbreviations: MI = Myocardial Infarction; ICH =
Intracranial Hemorrhage; GIH = Gastrointestinal
Hemorrhage; CDC = Centers for Disease Control
and Prevention.
0.013
Hemorrhage
ICH
0.00040
GIH
0.0010
Systemic (relative risk)
1
Mortality, long-term (>30 days)
Baseline (age, sex)
CDC Life Table
0.017
MI
Hemorrhage
ICH
0.094
GIH
0.0010
Mortality, short-term (<30 days)
MI
0.26
Hemorrhage
ICH
0.20
GIH
0.13
Table 7 (continued): Base-Case Values. Panel B,
medication risk and efficacy.
Abbreviations: MI = Myocardial Infarction; ICH =
Intracranial Hemorrhage; GIH = Gastrointestinal
Hemorrhage; CDC = Centers for Disease Control and
Prevention.
Aspirin
Risk
ICH
1.7
GIH
2.7
Efficacy
0.20
Clopidogrel
Risk
ICH
1.2
GIH
1.9
Efficacy
0.20
Dual Antiplatelet Therapy
Risk
ICH
2.0
GIH
5.0
Efficacy
0.40
Table 8: Base-Case Analysis.
Abbreviations: Dual-Rx = Dual Antiplatelet Therapy; LE = Life Expectancy; APT =
Antiplatelet Therapy.
Strategy
LE in years
Difference in LE in years (months in
parentheses) compared to
Placebo
Aspirin indefinitely
Dual-Rx indefinitely
13.48
0.12 (1.44)
0.06 (0.72)
Clopidogrel indefinitely
13.45
0.09 (1.08)
0.03 (0.36)
Dual-Rx for one year then
aspirin indefinitely
13.42
0.06 (0.72)
0
Aspirin indefinitely
13.42
0.06 (0.72)
Clopidogrel for one year
then aspirin indefinitely
13.42
0.06 (0.72)
No APT
13.36
-0.06 (-0.72)
Table 9: Ischemic heart disease cube measures. From U.S. Department of Veterans
Affairs [47].
eDescription
IHD Patient Count
Count of patients in the cohort.
Patients With Lipid Panel
Within 2 Years and LDL <
100
Count of patients that received a full lipid panel
within the last twenty-four months and the most
recent direct or calculated LDL value was less
than 100.
Percent Lipid Panel Within 2
Years and LDL < 100
Percent of patients that received a full lipid
panel within the last twenty-four months and
the most recent direct or calculated LDL value
was less than 100.
Target Lipid Panel Within 2
Years and LDL < 100
EPRP target for percent of patients that
received a full lipid panel within the last
twenty-four months and the most recent direct
or calculated LDL value that was less than 120.
Patients With LDL Done
(LDL > 120)
Count of patients with either a direct or
calculated LDL within the last twenty-four
months with a value greater then 120.
Percent With LDL Done
(LDL > 120)
Percent of patients with either a direct or
calculated LDL within the last twenty-four
months with a value greater then 120.
Target LDL >= 120
EPRP target for percent of patients that
received a direct or calculated LDL value that
was greater then 120.
Patients With Lipid Panel
Within 2 Years and LDL >=
100
Count of patients that received a full lipid panel
within the last twenty-four months and the most
recent direct or calculated LDL value was
greater then or equal to 100.
Percent Lipid Panel Within 2
Years and LDL >= 100
Percent of patients that received a full lipid
panel within the last twenty-four months and
the most recent direct or calculated LDL value
was greater then or equal to 100.
Patients No Lipid Panel Last
2 Years
Count of patients that did not received a full
lipid panel within the last twenty-four months.
Percent No Lipid Panel Last
2 Years
Percent of patients that did not received a full
lipid panel within the last twenty-four months.
Patients With LDL Done
(LDL < 100)
Count of patients with either a direct or
calculated LDL within the last twenty-four
months with a value less than 100.
Percent With LDL Done
(LDL < 100)
Percent of patients with either a direct or
calculated LDL within the last twenty-four
months with a value less than 100.
Patients With LDL Done
Count of patients with either a direct or
(LDL > = 100 and LDL <
calculated LDL within the last twenty-four
120)
months with a value greater then or equal to
100 and less then 120.
Percent With LDL Done
Percent of patients with either a direct or
(LDL > = 100 and LDL <
calculated LDL within the last twenty-four
120)
months with a value greater then or equal to
100 and less then 120.
Patients With LDL Not Done Count of patients with no direct or calculated
LDL within the last twenty-four months.
Percent With LDL Not Done
Percent of patients with no direct or calculated
LDL within the last twenty-four months.
Last LDL Value
Result of the last LDL taken either a direct or
calculated.
Date Last LDL Resulted
Date last LDL taken either a direct or
calculated.
1st Previous LDL Value
The first prior LDL (direct or calculated)
resulted after the patients last LDL (direct or
calculated) was taken.
Date 1't Previous LDL
Date first prior LDL (direct or calculated) was
Resulted
resulted.
2nd Previous LDL Value
The second prior LDL (direct or calculated)
resulted after the patients last LDL (direct or
calculated) was taken.
Date 2nd Previous LDL
Resulted
Date second prior LDL-Cholesterol was
resulted.
Last Outside LDL Value
Result of last LDL (direct or calculated) taken
off site. The outside lab result is taken from the
related LDL Health Factor at each site. If the
outside result is not entered into the Health
Factor as 'number.number' then the result value
is ignored.
Date Last Outside LDL
Value
Date last outside LDL (direct or calculated) was
resulted.
Patients With Aspirin Rx
(CN103)
Count of patients with Aspirin prescriptions
from the (CN103) drug class the patient had
within a twenty four time period.
Percent With Aspirin Rx
(CN103)
Percent of patients with Aspirin prescriptions
from the (CN103) drug class the patient had
within a twenty four time period.
Patients With Lipid Agents
Rx (CV350,TN300,VT103)
Count of patients with Lipid Agent
prescriptions from the (CV350, TN300,
VT103) drug class the patient had within a
twenty four month time period.
Percent With Lipid Agents
Rx (CV350,TN300,VT103)
Percent of patients with Lipid Agent
prescriptions from the (CV3 50,TN300,VT 103)
drug class the patient had within a twenty four
month time period.
Patients With Ace Inhibitor
Rx (CV800)
Count of patients with Ace Inhibitor
prescriptions from the (CV800) drug class the
patient had within a twenty four month time
period.
Percent of patients with Ace Inhibitor
prescriptions from the (CV800) drug class the
patient had within a twenty four month time
period.
Percent With Ace Inhibitor
Rx (CV800)
.1
Patients With Beta Blocker
Rx (CV100)
Count of patients with Beta Blocker
prescriptions from the (CV 100) drug class the
patient had within a twenty four month time
period.
Percent With Beta Blocker
Rx (CV 100)
Percent of patients with Beta Blocker
prescriptions from the (CV 100) drug class the
patient had within a twenty four month time
period.
Patients Received
Pneumococcal Vaccine
Count of patients that received at anytime the
Pneumococcal Vaccine.
Percent Received
Pneumococcal Vaccine
Percent of patients that received at anytime the
Pneumococcal Vaccine.
Patients Received Flu
Vaccine
Count of patients that received a flu
immunization within a twelve-month time
period.
Percent Received Flu
Vaccine
Percent of patients that received a flu
immunization within a twelve-month time
period.
7.5. Appendix E: Figures
Figure 1: Analysis of myocardial infarction according to the drug-eluting stent
type. From Schomig et al. [2].
No. of events / Total N4c.of patients
i rial
SES grotp
14/264
1:37
BASKET
Cervinka et al.
CORPAL
Di Lorenzo el al.
ISAR-DESIRE
ISAR-DIABETES
ISAR-SMART 3S
LONG-DES 'I
Petrcnio at ai.
PROSIT
REALFTY
SIRTAX
SORT-OUT I
TAXI
1I/1WI
21/250
1150
3/164
401684
18/503
P2=0%p PA
51/669
26:1C65
25/509
2111033
5/102
7/100
(1246
9/203
Zhang t at
Overall
19/281
1/33
2"321
3/90
3/206
4/100
4/125
7/1A0
27/250
1/50
3/151
4'90
2/210
3/100
6/125
Han at al.
--
178/4391 205/430'
PY
..
08 4 (c89,
=Dag9
0.o9
-4R
0 81(%% CL
Qz 1.02)
-
STolmus-eluung sient
Paclitaxeeltting stert
it
Months After Raxdorrization
2783
2033
2400
2185
2779
2590
2443
2145
3)
10)
Hazard Ratio
P"0.07
Patlortoa
SES
PES
Favors Favas
SES PES
PES group
24
30
1095
1634
65)
613
anaysis wf rMyocardaa intarcton
According to the Drug-Eluting Stent Type
(A) Absolute numbers ot palieits experiencing niyocardial infarcicn asso:isted
with SES versus 'ES for individual trials anc pooled population. The., HRs are
shown on, a
togathmic scale. The sizte uf tie squae is poportional to the
weight of 'he individual studies, neasured as the inverse of the estimated variance of the og FR. (B) Kaplan-Meier curves of myocardial infarction in eac& of
the stent groups for tie pooled population. Abbrevlat ons as In Figure 1.
Figure 2: Markov state transition model. Each circle represents a health state.
Health states are characterized by events which may occur over the course of the
modeling. The possible health states are status-post drug-eluting stent (S/P DES)
myocardial infarction (MI), intracranial hemorrhage (ICH), gastrointestinal hemorrhage
(GIH), any combination of MI, ICH and/or GIH (e.g. MI ICH) or death (DEAD). The solid
arrows (-) represent potential transitions from one health state to another health state,
depending on what events occur. For example, a patient who, during the course of
modeling, has already had an MI, and therefore in the health state MI may then have an
ICH, resulting in a transition the health state MI to the health state Ml ICH. If a patient
does not have event, then s/he remains in the same health state. The block arrow (J)
means patients in any other health state may die.
DEAD
Figure 3: One-way sensitivity analysis varying the value of the variable efficacy of
clopidogrel to prevent myocardial infarction.
Baseline= 0.20
13,5
1349t
Dual-Rx Indefinitely (D)
13-47
Aspirin Indefinitely (A)
13.46
Threshold= 0.09 (A,D)
2 13.454
------
- -----
_
.-
13.43
L 13.41
13.4
--
13.317
13.36 1
-___ -------
I...
0.0001)
9.0?
.4
0.04
..
...........
----------
0(.0h
0(.00
1
0.1
.
0.12
0.14
0.16
Efficacy of Clopidogrel to Prevent Myocardial Infarction
.18
0.18
0----22
0.2
[95% C.I. (0.12-0.027)]
03
Figure 4: One-way sensitivity analysis varying the value of the variable clopidogrel
risk associated with severe gastrointestinal hemorrhage.
Baseline= 2.01
13.495
-j
13.49
'
13.48
13.47
13.46
E0
13.44
C 13.43
0. 13.42
x
wj
!9
13.41
13.39
13.38
13.37
1.8000
2
2.2
2.4
2.6
2.8
3
3.2
Relative Risk of Severe Gastrointestinal Hemorrhage with Clopidogrel
3.4
3.6
3.80
[95% C.I. (1.00-3.97)]