Clinical Rehabilitation
advertisement

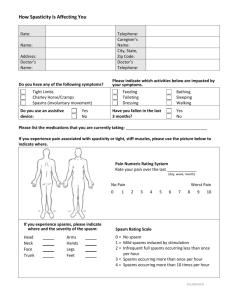
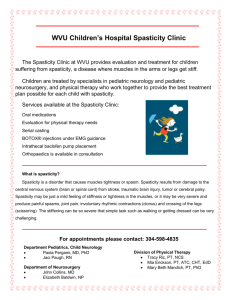
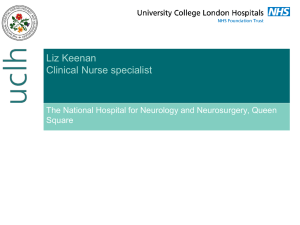
Clinical Rehabilitation http://cre.sagepub.com/ The Tardieu Scale differentiates contracture from spasticity whereas the Ashworth Scale is confounded by it Emily Patrick and Louise Ada Clin Rehabil 2006 20: 173 DOI: 10.1191/0269215506cr922oa The online version of this article can be found at: http://cre.sagepub.com/content/20/2/173 Published by: http://www.sagepublications.com Additional services and information for Clinical Rehabilitation can be found at: Email Alerts: http://cre.sagepub.com/cgi/alerts Subscriptions: http://cre.sagepub.com/subscriptions Reprints: http://www.sagepub.com/journalsReprints.nav Permissions: http://www.sagepub.com/journalsPermissions.nav Citations: http://cre.sagepub.com/content/20/2/173.refs.html Downloaded from cre.sagepub.com at UNIV OF DELAWARE LIB on March 1, 2011 Clinical Rehabilitation 2006; 20: 173-182 The Tardieu Scale differentiates contracture from spasticity whereas the Ashworth Scale is confounded by it Emily Patrick and Louise Ada School of Physiotherapy, The University of Sydney, Sydney, Australia Received 5th January 2005; returned for revisions 21 st February 2005; revised manuscript accepted 20th June 2005. Objective: To compare the Tardieu Scale as a clinical measure of spasticity after stroke with the Ashworth Scale. Design: Cross-sectional study. Participants: Sixteen people, living in the community three years after their stroke. Main measures: The Ashworth Scale and Tardieu Scale as well as laboratory measures of spasticity (stretch-induced electromyographic (EMG) activity) and contracture (maximum passive joint excursion) were collected from the affected elbow flexors and extensors and ankle plantarflexors and dorsiflexors by three examiners who were blinded to the results of the other measures. Results: The percentage exact agreement (PEA) between the Tardieu Scale and a laboratory measure of spasticity was 100% for both the elbow flexors and ankle plantarflexors. This was significantly (P= 0.02) greater than the PEA of 63% for both muscles between the Ashworth Scale and the same laboratory measure of spasticity. For contracture, the PEA between the Tardieu Scale and a laboratory measure was 94% for both the elbow flexors and the ankle plantarflexors. Pearson correlation coefficients between the Tardieu Scale and laboratory measures of spasticity were 0.86 for the elbow flexors and 0.62 for the ankle plantarflexors and between the Tardieu Scale and laboratory measures of contracture were 0.89 for the elbow flexors and 0.84 for the ankle plantarflexors. Conclusion: In all cases that spasticity was overestimated by the Ashworth Scale, participants had a contracture. These findings suggest that the Tardieu Scale differentiates spasticity from contracture whereas the Ashworth Scale is confounded by it. Introduction Spasticity, defined as 'a motor disorder characterised by a velocity-dependent increase in tonic stretch reflexes ("muscle tone") with exaggerated tendon jerks, resulting from hyperexcitability of Address for correspondence: Louise Ada, School of Physiotherapy, Faculty of Health Sciences, The University of Sydney, PO Box 170, Lidcombe NSW 1825, Australia. e-mail: L.Ada(fhs.usyd.edu.au (C 2006 Edward Arnold (Publishers) the stretch reflex' (ref. 1, p. 485), is one of the impairments of an upper motor neuron lesion. It is important for clinicians to be able to measure spasticity so that it can be accurately identified and the effectiveness of interventions aimed at reducing it can be evaluated. Currently, the Ashworth Scale2 or the modified Ashworth Scale3 are the most commonly used clinical measure of spasticity.4 However, the validity of the Ashworth Scales has been challenged. Pandyan et al.S concluded that Ltd Downloaded from cre.sagepub.com at UNIV OF DELAWARE LIB on March 1, 2011 10.1 191/0269215506cr922oa 174 E Patrick and L Ada confusion exists regarding the characteristics of the Ashworth Scale as a measure of spasticity. In addition, doubts have been raised about the validity of the Ashworth Scale after finding that it was not comparable to laboratory measures of spasticity. 6-9 The Ashworth Scale grades the resistance to movement but it appears unable to differentiate whether the cause of abnormal resistance is neural or peripheral.8- 11 Based on clinical and physiological observations, Tardieu12,13 proposed a method of measuring spasticity, from which a quantifiable scale was constructed by Held and Pierrot-Deseilligny'4 and this has been translated by Gracies et al.15 (see Appendix). The broad aim of this study was to investigate the validity of the Tardieu Scale as a clinical measure of spasticity after stroke by testing its content validity and comparing it with the Ashworth Scale. The specific research questions were: 1.3, range 1.2-5), consisting of 11 men and 5 women, and 7 right and 8 left hemiplegics were recruited. The procedures were approved by the institutional ethics committee and all participants gave informed consent prior to data collection. Design A cross-sectional, analytical study was undertaken, in which clinical scales were compared with laboratory measures of spasticity and contracture, with the latter used as the reference standard. Measurements were performed on the affected elbow flexors and extensors and the affected ankle plantarflexors and dorsiflexors of each participant. Prior to each measure, the joints were moved slowly and passively through range to precondition them. The participants were measured by one examiner using the Ashworth Scale, a different examiner using the Tardieu Scale and a third examiner collected the laboratory measures. 1) Does the Tardieu Scale identify the presence The three examiners were blinded to the results of of spasticity more effectively than the Ash- the other measures. The order of the measures was worth Scale after stroke? random and all testing procedures were completed 2) Does the Tardieu Scale reflect the severity of in a single session. spasticity more effectively than the Ashworth Scale after stroke? Clinical scales 3) Does the Tardieu Scale identify the presence of contracture after stroke? Scale 4) Does the Tardieu Scale reflect the severity of Ashworth sat on a bed with their legs extended Participants contracture after stroke? and their arms resting by their side. The trunk was with the head in a neutral position. Our hypothesis was that the Tardieu Scale would supported were instructed to completely relax Participants be able to differentiate contracture from spasticity while their affected elbows and ankles were pasand therefore be the more valid clinical measure of sively moved throughout range in both directions spasticity. by the examiner. Spasticity was quantified according to the Ashworth Scale using the criteria for grades 0-4 outlined by Ashworth.2 Method Participants Individuals who had had one stroke resulting in hemiplegia were recruited for this study. Patients were excluded from the study only if they were younger than 45 or older than 85 years, or if they had severe cognitive or language deficits hat would interfere with the comprehension of instructions required to participate in the study. Sixteen participants, aged 63 years old (SD 7, range 51-77), three years since stroke (SD Tardieu Scale Participants sat in the same standardized position as described for the Ashworth Scale. The affected limbs were passively moved through range at two velocities - first, 'as slow as possible' (VI) and then 'as fast as possible' (V3), as described by Held and Deseilligny14 and interpreted by the examiner. At both velocities, the quality of the muscle reaction to stretch (X) was assessed for each muscle group and the angle at which the muscle reaction occurred (Y) was measured with a Downloaded from cre.sagepub.com at UNIV OF DELAWARE LIB on March 1, 2011 Clinical measurement of spasticity after stroke 175 hand-held goniometer after the cessation of the movement. Contracture was quantified by recording the angle at which the muscle reaction occurred during the slow velocity stretch (V1). This velocity is considered to be too slow to excite abnormal reflex activity following stroke, therefore, the angle recorded represents the end of range.'5 Spasticity was quantified according to the criteria of muscle reaction for grades 0-4 during the fast velocity of stretch (V3). The velocity of the limb segment falling under gravity (i.e., V2) was not used in this study since it is not practical for most muscle groups. Laboratory measures The same experimental set-up was used for measurement of both contracture and spasticity (Figure 1). First, participants sat at an adjustable table in a high-backed chair, with their affected arm in 90 degrees of shoulder flexion and the forearm secured in a horizontal arm frame which constrained movement to flexion and extension at the elbow (Figure la). A potentiometer at the axis of rotation of the arm frame measured joint angle while a load cell (capacity 250 N; Applied Measurement, Sydney, Australia) fixed to a handle measured applied torque. Then, participants were positioned in long sitting with the affected foot secured in a foot frame that constrained movement to plantarflexion and dorsiflexion at the ankle (Figure lb). A potentiometer at the axis of rotation of the arm frame measured joint angle while a load cell (capacity 450 N) fixed to a handle measured applied torque. Muscle activity was measured using bipolar silver-silver chloride surface electrodes. Electrodes were positioned according to Basmajan and Blumenstein.'6 The electrode impedance was kept below 5 kQ by thorough abrading and cleaning of the skin and the experiment proceeded only when a satisfactorily low level of background noise was achieved (less than 10 ptV). Contracture Maximum passive joint excursion was measured. Participants were asked to relax with the affected limb positioned in the frame and the electromyograph (EMG) recording was displayed on the computer screen to ensure that participants remained relaxed. The relaxed limb was slowly moved to the end of range by applying 2 Nm to the upper limb and 10 Nm to the lower limb and this was held for 5 s. Spasticity Stretch-induced muscle activity was measured. Participants were asked to relax with the affected limb positioned in the frame and, prior to stretching, the EMG recording was displayed on the computer screen to ensure that muscles were (b) Figure 1 Set-up for the laboratory measures for the (a) upper and (b) lower limb. Three signals were collected: a potentiometer measured joint angle, a load cell measured applied torque and electrodes measured muscle activity. Downloaded from cre.sagepub.com at UNIV OF DELAWARE LIB on March 1, 2011 176 E Patrick and L Ada electrically silent. The muscles were then stretched by moving the limbs passively through range at two velocities - fast and slow. Five ramp stretches were recorded for each velocity in each muscle group. In order to remove any 50 Hz line frequency interference or low-frequency movement artefact, the EMG was high-pass filtered (digital eighthorder Butterworth) at 80 Hz. Normally, no EMG activity is observed when the relaxed muscles of a neurologically normal person are stretched in this manner. ,18 Therefore, any stretch-induced EMG activity observed was considered to be abnormal and indicative of spasticity. ' Figure 2 presents data from two participants, one with spasticity and one without. Even in the presence of severe spasticity (Figure 2d), no evidence of stretch reflex activity was apparent during the slow ramp stretch (Figure 2c), confirming that the slow velocities of stretch did not excite the stretch reflex response in stroke. flexion, < 130 degrees elbow flexion, or elbow extension was > 5 degrees off a straight elbow. Data extraction Measurement yielded five variables for each muscle group. There were three variables for spasticity: fast stretch-induced EMG activity, Tardieu score and Ashworth score. For the clinical scales, spasticity was operationally defined as being present when the scores reflected a neural event, such as a catch occurring at a precise angle. Therefore, spasticity was considered present in a muscle group if the score was . 1 on the Ashworth Scale and if the muscle reaction grade (X) during the fast velocity stretch (V3) was . 2 on the Tardieu Scale. For the laboratory measure, spasticity was considered to be present if, on visual examination, a clear burst of EMG was timelocked to the maximum velocity of ramp stretch (Figure 2d) in at least three of the five trials. In order to quantify the severity of the spasticity in the laboratory measure, the EMG was rectified and integrated, and the average peak stretchinduced activity across trials was determined. There were two variables for contracture: maximum passive joint excursion and Tardieu score (Y at VI). Contracture was operationally defined as being present if the angle at the end of range was 5 -10 degrees less than full range. Therefore, for both clinical and laboratory measures, contracture was present if end-of-range was: < 10 degrees ankle dorsiflexion; < 25 degrees ankle plantar- Results Statistical analysis In order to examine the ability of the Ashworth and Tardieu Scales to identify the presence of spasticity and/or contracture, the percentage exact agreement (PEA) between laboratory and clinical measures was calculated. The significance of the differences in PEA was determined using Fisher's exact P-value of the chi-square statistic to account for small numbers in some cells. In order to examine the ability of the Tardieu Scale to reflect the severity of spasticity and contracture, the ordinal clinical measures of spasticity and interval measures of contracture were correlated with the interval laboratory measures of spasticity and contracture using the Pearson correlation coefficient. Spectrum of participants For each muscle group, participants were placed into one of four categories based on the presence or absence of spasticity and contracture as determined by the laboratory measures (Table 1). Only two of the four muscle groups (elbow flexors and ankle plantarflexors) displayed each combination of spasticity and contracture. Therefore, only these muscle groups were subsequently analysed. Does the Tardieu Scale identify the presence of spasticity more effectively than the Ashworth Scale after stroke? In identifying the presence or absence of spasticity in the elbow flexors, there was 100% exact agreement between the Tardieu Scale and the laboratory measure of spasticity (chancecorrected agreement statistic kappa = 1.0). In contrast, there was 63% exact agreement between the Ashworth Scale and the laboratory measure of spasticity (kappa = 0.24), showing a significantly poorer ability of this scale to correctly identify spasticity in the elbow flexors (P = 0.02). The percentage exact agreement between the Tardieu Scale and the laboratory measure of spasticity in the ankle plantarflexors was also Downloaded from cre.sagepub.com at UNIV OF DELAWARE LIB on March 1, 2011 Clinical measurement of spasticity after stroke 177 (a) (b) 20 20 -oC) 0) C c U) c - -30 -30 250 250 CD=LL w c: E a) CD CD -250 (c) -250 L (d) 20 20 0) w U) a) CD -0) co ._l c -30 ,250 250 r 0'25 a) (I) li JLJL 11 IIv 7 -1 (U C20 Ct -30 i1 s -250 Figure 2 Muscle activity (lower traces) in response to (a) slow and (b) fast ramp stretches (upper traces) in a participant with no spasticity. Muscle activity (lower traces) in response to (c) slow and (d) fast ramp stretches (upper traces) in a participant with spasticity. Note the absence of reflex reaction to the slow stretch (c) even when a large reflex reaction and clonus is present during fast stretch (d). 100% (kappa = 1.0). In contrast, the percentage exact agreement between the Ashworth Scale and the laboratory measure was 63% (kappa = 0.25), showing a significantly poorer ability of this scale to correctly identify spasticity in the ankle plantarflexors (P = 0.02). Does the Tardieu Scale reflect the severity of spasticity more effectively than the Ashworth Scale after stroke? Figure 3(a and b) illustrates the relationship between the clinical and laboratory measures of spasticity. In the elbow flexors, there was a strong, Downloaded from cre.sagepub.com at UNIV OF DELAWARE LIB on March 1, 2011 178 E Patrick and L Ada Table 1 Spectrum of spasticity and contracture Spasticity Elbow flexors Contracture Y N Elbow extensors Ankle plantarflexors Ankle dorsiflexors Y N Y N Y N Y N 4 3 5 4 0 8 0 8 4 4 3 5 0 0 0 16 significant relationship between the grade of muscle reaction (X) during the fast stretch (V3) using the Tardieu Scale and peak stretch-induced EMG activity (r = 0.86, P = 0.001). In addition, there was a significant but moderate relationship between the Tardieu Scale and the laboratory measure of spasticity in the ankle plantarflexors (r = 0.62, P = 0.01). In contrast, there was little relationship between the Ashworth Scale and the - Spas(A) = 0.1 Spas(Lab) + 0.3 Spas(T) = 0.2 Spas(Lab) + 0.3 (D 8- W 64 Spas(A) = 0.01 Spas(Lab) + 0.5 Spas(T) = 0.1 Spas(Lab) + 1 50 O > 1210 - a) Does the Tardieu Scale identify the presence of contracture after stroke? In identifying the presence or absence of contracture in the elbow flexors, there was 94% exact agreement between the Tardieu Scale and the (b) (a) 12 laboratory measure of spasticity in either the elbow flexors (r = 0.33, P = 0.21) or ankle plantarflexors (r=J0.15, P =0.59). 40 O 8 o, 30 0, O 20 - 10 2 S 0 _S___ 0 0 2 1 4 3 1 0 2 3 4 Clinical scale score (0-4) (c) (d) cm 35 25 Cont(T) = 0.3 Cont(Lab) + 0.8 230 Cont(T) = Cont(Lab) + 2 20 a) C) 25 15 c L- 20 a) .' 15 cZQ. 10 X co *~~~~~/ 10 . 0 5 5 0 -5 0 2 4 6 8 10 12 -5 Tardieu Scale score 5 - 15 25 (deg) Figure 3 Relations between the Tardieu score and laboratory measure (closed circles and solid line) and Ashworth score and laboratory measure (open circle and dotted line) for (a) elbow flexor spasticity, (b) plantarflexor spasticity, (c) elbow flexor contracture, and (d) plantarflexor contracture. Equations of the relations are included where T = Tardieu score, A = Ashworth scores, and Lab = laboratory measures. Downloaded from cre.sagepub.com at UNIV OF DELAWARE LIB on March 1, 2011 Clinical measurement of spasticity after stroke 179 laboratory measure of contracture (kappa = 0.88). The percentage exact agreement between the Tardieu Scale and the laboratory measure of contracture in the ankle plantarflexors was also 94% (kappa = 0.88). Does the Tardieu Scale reflect the severity of contracture after stroke? Figure 3(c and d) presents the relationship between the clinical and laboratory measures of contracture. There was a strong, significant relationship between the angle of muscle reaction (Y) during the slow stretch (Vi) using the Tardieu Scale and the laboratory measure of contracture in both the elbow flexors (r = 0.89, P = 0.00 1) and ankle plantarflexors (r = 0.84, P = 0.001). Discussion This is the first study to compare the Tardieu Scale with the Ashworth Scale in people after stroke. The results indicate that the Tardieu Scale is able to identify the presence of spasticity more effectively than the Ashworth Scale in both an upper and lower limb muscle. There have been many previous suggestions that the Ashworth Scale is not adequate as a measure of spasticity.5- 1l The moderate percentage exact agreement between the Ashworth Scale and laboratory measures of spasticity found in this study is in line with previous studies examining the validity of the Ashworth Scale by comparing it with other clinical19'20 and laboratory6-1 measures. The only study showing a significant relationship between the Ashworth Scale and laboratory measures21 used markedly higher stretching velocities than the current study in a group of spinal cord-injured patients. The lack of agreement between the Ashworth Scale and laboratory measures of spasticity in the current study may be because the Ashworth Scale does not exclusively measure spasticity. Experimental evidence suggests that increased resistance to movement is not exclusively dependent on stretch reflex activity but is also due to increased stiffness as a result of contracture.9,22-24 Therefore, by quantifying the resistance to passive movement, the Ashworth Scale measures a combination of neural and peripheral factors (i.e., it does not differentiate spasticity from contracture). Spasticity was overestimated by the Ashworth Scale 15% of the time when compared with the laboratory measures of stretch-induced EMG activity, in line with a previous study.6 In 100% of these cases, participants had a contracture compared with only 14% of the cases when spasticity was underestimated by the Ashworth Scale. This suggests that the Ashworth Scale is confounded by contracture. Not only was the Tardieu Scale able to identify the presence of spasticity, but it was also able to identify the presence of contracture. This is most likely because the Tardieu Scale takes into account the main factor to which the stretch reflex is known to be sensitive - the velocity of stretch. This velocity-dependence of the stretch reflex has been well established (e.g., refs 1, 24 and 25] with several studies reporting no stretch reflex during slow passive movements23 24262' and evidence of a threshold velocity of stretch below which no EMG response was elicited.28'29 In the current study, the slow stretch did not result in stretch-induced EMG activity in any participant in either muscle group, so that the end of the stretch accurately reflected the end of range. This suggests, therefore, that contracture can be validly measured in the clinic, even in the presence of spasticity, by moving the limb very slowly so as to not excite hyperactive reflexes. On the other hand, during the fast stretch, nearly half the participants exhibited stretch-induced EMG activity in both muscle groups which was strongly related to the grade of the muscle reaction (X) during V3 using the Tardieu Scale. Some researchers have proposed that the angle of muscle reaction (Y) recorded during V3 be used to measure the amount of spasticity present in a muscle rather than the grade of muscle reaction (X). 15,30 However, in the current study, the relationship between the angle of muscle reaction at V3 was only significantly related to the angle at which fast stretch-induced EMG activity occurred in the elbow flexors (r = 0.78, P = 0.04), not in the ankle plantarflexors (r = - 0.57, P = 0.14). This suggests that the grade of muscle reaction (X) during the fast velocity stretch (V3) is the most appropriate measure of spasticity from the Tardieu Scale. Taken together, these findings suggest that the Tardieu Scale appears to be the more valid Downloaded from cre.sagepub.com at UNIV OF DELAWARE LIB on March 1, 2011 180 E Patrick and L Ada Clinical * * messages Spasticity measured by the Ashworth Scale is confounded by contracture. The Tardieu Scale differentiates spasticity from contracture, therefore, it is the more valid clinical tool. clinical tool for the measurement of spasticity after stroke because it can differentiate spasticity from contracture. Nevertheless, one of the limitations of the present study was that the examiners only measured the participants using one measure. Although this meant that the examiners were blinded to the results of the other measures, it also means that the results could have been confounded by examiner experience. However, the examiners standardized the procedures beforehand and the examiner using the Ashworth Scale had more clinical experience than the examiner using the Tardieu Scale. Even though the Tardieu Scale takes slightly longer to apply, it is suggested that it be used to measure spasticity in clinical practice, since distinguishing between the neural and peripheral contributions to movement resistance after stroke enables intervention to be accurately directed at the underlying impairments. Acknowledgements We are grateful to Anchalee Foongchomcheay for being the third blinded measurer in this study and Roger Adams for his help with the statistical analysis. References Lance JW Symposium synopsis. In Feldman RG, Young RR, Koella WP eds. Spasticity: disordered motor control. Year Book Medical Publishers, 1980: 485-94. 2 Ashworth B. Preliminary trial of carisoprodal in multiple sclerosis. The Practitioner 1964; 192: 540-42. 3 Bohannon RW, Smith M. Interrater reliability of a Modified Ashworth Scale of muscle spasticity. Phys Ther 1987; 67: 206-207. 1 4 Van Wijck FM, Pandyan AD, Johnson GR, Barnes MP. Assessing motor deficits in neurological rehabilitation: patterns of instrument usage. Neurorehabil Neural Repair 2001; 15: 23-30. 5 Pandyan A, Johnson G, Price C, Curless R, Barnes M, Rodgers H. A review of the properties and limitations of the Ashworth and modified Ashworth Scales as measures of spasticity. Clin Rehabil 1999; 13: 373-83. 6 Nielsen JF, Sinkjaer T. A comparison of clinical and laboratory measures of spasticity. Multiple Sclerosis 1996; 1: 296-301. 7 Priebe M, Sherwood A, Thornby J, Kharas N, Marlowski J. Clinical assessment of spasticity in spinal cord injury: a multidimensional problem. Arch Phys Med Rehabil 1996; 77: 713-16. 8 Vattanasilp W, Ada L. The relationship between clinical and laboratory measures of spasticity. Aust J Physiother 1999; 45: 135-39. 9 Vattanasilp W, Ada L, Crosbie J. Contribution of thixotropy, spasticity, and contracture to ankle stiffness after stroke. J Neurol Neurosurg Psychiatry 2000; 69: 34-39. 10 Bakheit AMO, Maynard VA, Curnow J, Hudson N, Kodapala S. The relation between Ashworth scale scores and the excitability of the alpha motor neurones in patients with post-stroke muscle spasticity. J Neurol Neurosurg Psychiatry 2003; 74: 646-48. 11 Pandyan A, Price C, Barnes M, Johnson G. A biomechanical investigation into the validity of the modified Ashworth Scale as a measure of elbow spasticity. Clin Rehabil 2003; 17: 290-93. 12 Tardieu G, Shentoub S, Delarue R. A la recherche d'une technique de mesure de la spasticite. Rev Neurol 1954; 91: 143-44. 13 Tardieu G, Rondont 0, Mensch J, Dalloz J-C, Monfraix C, Tabary J-C. Responses electromyographiques a l'etirement musculaire chez l'homme normal. Rev Neurol 1957; 97: 60-61. 14 Held J, Pierrot-Deseilligny E. Reeducation motrice des affections neurologiques. J B Bailliere, 1969: 3142. 15 Gracies J-M, Marosszeky J, Renton R, Sandaman J, Gandevia S, Burke D. Short-term effects of dynamic lycra splints on upper limb in hemiplegia patients. Arch Phys Med Rehabil 2000; 81: 1547- 55. 16 Basmajan JV, Blumenstein R. Electrode placement in EMG biofeedback. Williams and Wilkins, 1980. 17 Ibrahim IK, Berger W, Trippel M, Dietz V. Stretchinduced electromyographic activity and torque in spastic elbow muscles. Differential modulation of reflex activity in passive and active motor tasks. Brain 1993; 116: 971-89. Downloaded from cre.sagepub.com at UNIV OF DELAWARE LIB on March 1, 2011 Clinical measurement of spasticity after stroke 181 18 Yeo W, Ada L, O'Dwyer NJ, Neilson PD. Tonic stretch reflexes in older able-bodied people. Electromyogr Clin Neurophysiol 1998; 38: 273-78. 19 Katz RT, Rovai GP, Brait C, Rymer WZ. Objective quantification of spastic hypertonia: correlation with clinical findings. Arch Phys Rehabil Med 1992; 73: 339-47. 20 Leslie GC, Muir K, Part NJ, Roberts RC. A comparison of the assessment of spasticity by the Wartenberg pendulum test and the Ashworth grading scale in patients with multiple sclerosis. Clin Rehabil 1992; 6: 41-48. 21 Skold C, Harms-Ringdahl K, Hulting C, Levi R, Seiger A. Simultaneous Ashworth measurements and electromyographic recordings in tetraplegic patients. Arch Phys Med Rehabil 1998; 79: 959-65. 22 O'Dwyer NJ, Ada L, Neilson PD. Spasticity and muscle contracture following stroke. Brain 1996; 119: 1737-49. 23 Hufschmidt A, Mauritz K-H. Chronic transformation of muscle in spasticity: a peripheral contribution to increased tone. J Neurol Neurosurg Psychiatry 1985; 48: 676 85. 24 Thilmann AF, Fellows SJ, Ross HE Biomechanical changes at the ankle joint after stroke. J NAeurol Neurosurg Psychiatry 1991; 54: 134-39. 25 Meyer M, Adorjani C. Tonic stretch reflex for quantification of pathological muscle tone. In Feldman RG, Young RR, Koella WP eds. Spasticity: disordered motor control. Symposia Specialists, 1980: 315-31. 26 Ashby P, Burke D. Stretch reflexes in the upper limb of spastic man. J Neurol Neurosurg Psychiatry 1971; 34: 765-71. 27 Lehmann JF, Price R, deLateur BJ, Hinderer S, Traynor C. Spasticity: quantitative measurements as a basis for assessing effectiveness of therapeutic intervention. Arch Phys Med Rehabil 1989; 70: 6-15. 28 Ashby P, Mailis A, Hunter J. The evaluation of "spasticity". Can J Neurol Sci 1987; 14: 497-500. 29 Lin J-P, Brown JK, Brotherstone R. Assessment of spasticity in hemiplegic cerebral palsy. II: distal lower-limb reflex excitability and function. Dev Med Child Neurol 1994; 36: 290-303. 30 Boyd RN, Graham HK. Objective measurement of clinical findings in the use of botulinum toxin type A for the management of children with cerebral palsy. Eur J Neurol 1994; 6 (suppl 4): S23-S35. Appendix - Tardieu Scale Grading is always performed at the same time of day, in a constant position of the body for a given limb. Other joints, particularly the neck, must also remain in a constant position throughout the test and between tests. For each muscle group, reaction to stretch is rated at a specified stretch velocity with two parameters, X and Y Velocity of stretch Vi: As slow as possible (minimizing stretch reflex). V2: Speed of the limb segment falling under gravity. V3: As fast as possible (faster than the rate of the natural drop of the limb segment under gravity). Vl is used to measure the passive range of motion. Only V2 or V3 are used to measure spasticity. Quality of the muscle reaction (X) 0: No resistance through the course of the passive movement. 1: Slight resistance throughout the course of the passive movement with no clear catch at a precise angle. 2: Clear catch at a precise angle, interrupting the passive movement, followed by release. 3: Fatigable clonus (<10 s when maintaining pressure) occurring at a precise angle. 4: Unfatigable clonus ( >10 s when maintaining pressure) occurring at a precise angle. Downloaded from cre.sagepub.com at UNIV OF DELAWARE LIB on March 1, 2011 182 E Patrick and L Ada Angle of muscle reaction (Y) Measured relative to the position of minimal stretch of the muscle (corresponding to angle 0) for all joints except hip, where it is relative to the resting anatomic position. Adapted from Tardieu12'13 by Held and Pierrot-Deseilligny14 and translated by Gracies et al.'5 Downloaded from cre.sagepub.com at UNIV OF DELAWARE LIB on March 1, 2011