Enterprise Architecture Processes: Comparing EA and CLIOS in
the Veterans Health Administration
ARCHIVES
by
Chunguang Wang
-
Bachelor of Science in Computer Science,
Dordt College, May 2000
Submitted to the System Design and Management Program in partial fulfillment of the
requirements for the degree of Master of Science in Engineering and Management
at the
Massachusetts Institute of Technology
August 2011
0 2011 Chunguang Wang
All rights reserved
The author hereby grants to MIT permission to reproduce and to distribute publicly paper and electronic
copies of this thesis document in whole or in part in any medium now known or hereafter created.
Signature of Author:
'
(
Chunguang Wang
System Designnd Management Program
A
Certified by:
A
0ebora$Nightingale
Professor of the Practice, Aeronautics & Astronautics and Engineering System Division
Thesis Supervisor
Certified by:
I-m
Joseph
Accepted by:
Patrick Hale
Director, System Design and Management Program
This page has been intentionally left blank.
Page 2 of 94
Enterprise Architecture Processes: Comparing EA and CLIOS in
the Veterans Health Administration
Chunguang Wang
ABSTRACT
There are numerous frameworks for abstracting an enterprise complex system into a
model for purposes of analysis and design. Examples of such frameworks include the
Complex Large-scale Interconnected Open Social-technical System (CLIOS) process for
handling enterprise system architecture, the Enterprise Architecture eight views (EA) for
diagnosing and improving overall enterprise performance, and the Enterprise Strategic
Analysis for Transformation (ESAT). In addition to helping identify and manage
complexity, emergent behavior and the requirements of many stakeholders, all of these
frameworks help identify enterprise-wide processes, bringing value-added flow between
enterprises and their stakeholders. This thesis evaluates the applicability of integrating
these frameworks into a hybrid process in ongoing programs and to determine if a
standard process can be generated through an integrative, interdisciplinary approach
using the above models and frameworks.
Enterprise Architecture eight views framework as developed at MIT is designed to create
enterprise-level transformations in large, complex socio-technical enterprises. In the past
15 years of research at LAI, these enterprise developments have been applied and
validated in the govemment and in other industries including aerospace, transportation,
healthcare case, defense acquisition and logistics.
The CLIOS process, also developed at MIT, is designed to work with Complex, Largescale, Integrated, Open, Socio-technical systems, creating strategies for stakeholders to
reach goals through enterprise development. This process has been used heavily in
transportation systems, energy distribution, and regional strategic transportation planning.
Page 3 of 94
This thesis will apply both of these frameworks to the case of Veterans Affairs health
care enterprise to evaluate its effectiveness. Based on insights from self-assessments and
the organization's strategy, a transformation plan will be generated for the Veterans
Affairs organization's current state and preferred future state. These outcomes will help
to identify the strengths of the merged methodology.
Thesis Supervisor:
Deborah J.Nightingale
Title:
Professor of the Practice
Aeronautics and Astronautics and Engineering Systems Division
Thesis Advisor:
Joseph Sussman
Title:
JR East Professor
Professor of Civil and Environmental Engineering and Engineering
Systems
Thesis Advisor:
Donna Rhodes
Title:
Senior Lecturer, Engineering Systems
Principal Research Scientist, Systems Engineering Advancement
Research Initiative and Lean Advancement Initiative
Page 4 of 94
This page has been intentionally left blank.
Page 5 of 94
Dedication
For my family
Page 6 of 94
Acknowledgements
There are many individuals who have contributed to and supported my pursuit of a
graduate degree, including mentors, teachers, friends and family. I would like to
apologize in advance for any unintentional omissions.
Coming to study in the United States began with an opportunity in the late 1990s. I am
thankful for meeting this group of American teachers, which include Marilyn Van
Driesen, Betty & Bill Saltzman and others, who encouraged me to pursue studying
overseas; this ultimately led me to my own "Journey to the West". Little did I know then
that this journey would change and impact my life significantly. Dordt College gave me
the opportunity for me to begin my studies in the United States with a fully funded grants
and scholarships. Thank you to Dr. Curtis Taylor for helping me with this transition,
which allowed me to meet my lifelong friends Maria Philipson, Tricia Van Dyk and
many other students who helped me with my English and my adaptation to American
culture.
During my 10 years in the Pacific Northwest, several people gave me tremendous help
and treated me like family. I would like to thank Jacy Yu for always being there for me
and for making me feel at home. You are like a sister to me. Jack & Sue Bishop, Mark &
Sandra Spee, and many others are now as dear to me as my own family.
I would also like to thank the System Design and Management faculty and staff for
giving me advice. A special thanks to Pat Hale, Dave chultz, Chris Bates, Ed Crowly and
Tom Allen for your kindness. You are excellent professors, mentors and friends.
Thank you to all of my classmates in SDM 09, SDM10 and SDM1 1. Thank you for
sharing your diverse backgrounds, experiences, cultures and perspectives in such a
special community.
Page 7 of 94
Over the course of two semesters working on the VA case, I worked with numerous
individuals at both the VA and MIT. I would to thank them for all their efforts and
support. Specifically, I would like to thank our project sponsor, Mr. Mark Lyons, who
currently leads this effort at the VHA and serves as the VIRS Coordinator in VISN 20. In
addition, I received excellent support from individual VISN facilities, including Ms.
Lynne Cannavo at the West Roxbury facility in VISN 1 and Dr. Kathleen Gibson in
Tucscon (VISN 18). Our project mentor Jordan Peck provided superb support throughout
the semester and helped focus our efforts. This case would not have been completed
without this great team: Dan Marticello, Cody Kamin, Andrea Ippolito, Ariadne Smith,
and Andrea Gentiletti. Finally, our TA Jorge Oliveira, Professor Deborah Nightingale and
Dr. Rhodes guided us and provided significant education on the ESAT, EA and
Transformation process.
Thank you to my advisors, Debbie Nightingale, Joephen Sussman and Donna Rhodes,
who took the time to show me how to think through the differences between conceptual
and practical analysis through cases. Thank you for giving me this opportunity to do
research on the health case and to apply all my knowledge and experience towards such
an enterprise.
Finally, I would like to acknowledge my family for being the greatest inspiration for my
personal interests and ambitions. To my sister, Hui, thank you for your endless
encouragement and conversation whenever I want to talk. To my father, Yongxing, you
always believe in what I could do and taught me the importance of individual, family and
life values. To my mother, Shuzhen, you are my role model. You taught me how to face
challenges with a big smile. You shared your wisdom to help me "dream big". To my
husband, Zhiyong, you are truly my soulmate, knowing my thoughts before I even open
my mouth. You are so patient and supportive with my ups and downs. How grateful and
blessed that I am able to have you all in my life.
Page 8 of 94
In memory of GuiYing Shao, a loving grandmother
Page 9 of 94
This page has been intentionally left blank
Page 10 of 94
Contents
.....................
A BSTRACT .....................................................................................................................D ED ICATIO N ...........................................................................
..............................
A CKNOW LED GEM ENTS ..............................................................................
ENTERPRISE ARCHITECTURE ........................................................
-- 6
-.......................
-.................. 7
-.............
.......................
13
-..................................
13
CURRENT FRAM EW ORKS ..................................................................................
1.0
3
1.1
Introduction of EnterpriseArchitectures (EA).....................................................................
1.2
Sum m ary....................................................................................................................................................19
17
LEAN ADVANCEMENT INITIATIVE (LAI) TOOLS.............................20
2.0
20
2.1
Introduction of Lean Advancement Initiative Tools..........................................................
2.2
X-M atrix......................................................................................................................................................20
2.3
Lean EnterpriseSelf-Assessm ent Tool (LESAT)..................................................................
22
2.4
Sum m ary of LAI Tools ..........................................................................................................................
23
3.0
CLIO S PROCESS..................................................................................
..................
.............
3.1
Introductionof the CLIOS...................................................................................................................25
3.2
CLIOS Process...........................................................................................................................................25
4.0
...- 34
A NALYSIS...................................................................................................................----
34
COMPARISON BETWEEN EA AND CLIOS PROCESS ............................
5.0
M ERGING PROCESS ....................................................
25
...........................................................
36
5.1
StrategicPlanningStage....................................................................................................................
36
5.2
Planning& Transformation Stage..............................................................................................
38
5.3
Execution Stage.......................................................................................................................................40
5.4
Sum m ary....................................................................................................................................................41
APPLICATION: VETERANS AFFAIRS CASE STUDY (WANG, ET AL. 2010,2011).............43
6.0
INTRODUCTION ..............................................................................
7.0
T HE ENTERPRISE TODAY ..........................
...........................
.................................................
........... 43
..................
44
7.1
Stakeholders.............................................................................................................................................44
7.2
Metrics and Costs (for strategic alternativesin performanceimprovements)...........52
7.3
X-M atrix......................................................................................................................................................53
7.4
CLIOS...........................................................................................................................................................59
7.4.1
Stage 1: Representation...................................................................................................................59
7.4.2
Stage 2: Design, Evaluation and Selection...........................................................................
Page 11 of 94
62
Stage 3: Im plementation .................................................................................................................
65
7.5
EnterpriseArchitecture Framework (8 Views).....................................................................
68
7.6
Merging EA & CLIOS Design, Evaluation and SelectionError!
Bookmark
not
7.4.3
defined.
7.7
FinalImplem entation...........................................................................................................................78
CO N CLUSIO N .........................................................................................................................................
APPEN D ICES .............................................................................................................................
80
1........81
APPENDIX A: STAKEHOLDER GROUP SURVEY QUESTIONS...............................................................81
APPENDIX B: TAILORED LESAT TABLES ....................................................................................
R E FERE N C E .........................................................................................................................
Page 12 of 94
84
92
9............
Current Frameworks
Enterprise development depends on fundamental architecture frameworks. In order to
evaluate enterprise structure and development, a good framework needs to provide a clear
outline to follow and needs to identify the necessary improvements for the enterprise to
reach its goals.
1.0 Enterprise Architecture
Lean Advancement Initiative (LAI) at the Massachusetts Institute of Technology (MIT)
has developed a framework for enterprise-level transformations in large complex sociotechnical enterprises. In the past 15 years of research at LAI, these Enterprise
Architecture ("EA") developments have been applied and validated in both government
and industries including aerospace, transportation, healthcare cases, defense acquisition
and logistics.
Enterprise Architecture's research focuses on providing effective strategies for successful
enterprise transformation. At LAI, enterprise transformation and architecting is being
taught in two graduate level courses: "Integrating the Lean Enterprise" and "Enterprise
Architecting." In these courses, students are able to apply enterprise principles and
transformation methodologies through case studies. A transformation plan entails
considering various self-assessments and corporate strategy in order to bring a close to
the current state and sketch out the preferred future state (Nightingale, 2009).
The EA framework for transformation consists of a set of interdependent methodologies,
tools and enterprise principles that support holistic enterprise transformation, including
the following five elements:
1. Key Principles of Enterprise Thinking
2. Enterprise Transformation Roadmap
3. Lean Enterprise Self Assessment Tool (LESAT)
Page 13 of 94
4. Enterprise Strategic Analysis for Transformation (ESAT)
5. Enterprise Architecting Framework: provide enterprise systems analysis and
design of various industry and governmental organizations
In Figure 1, there are seven principles of system thinking, which are fundamental
concepts for enterprise development.
1.
2.
Adopt a holistic
approach to
enterprise
transformation.
Identify relevant
stakeholders and
determine their
value propositions.
Focus on
enterprise
effectiveness
before efficiency.
4.
5.
6.
7.
Address internal
and external
enterprise
interdependencies.
Ensure stability
and flow within
and across the
enterprise.
Cultivate
leadership to
support and drive
enterprise
behaviors.
Emphasize
organizational
learning.
Figure 1
Principles of System Thinking (Nighingale, 2009)
The Enterprise Transformation Roadmap shown in Figure 2 provides guidance for
making decisions that consider cultural, organizational and change management in the
strategic analysis and transformation of enterprises. It is also considered as an enterprise
leadership path. The roadmap consists of three cycles:
1. Strategic Cycle: Business case for transformation and leadership's engagement
are coherently moving together.
2. Planning Cycle: Section combined with analysis on the current state and future
state; create a transformation plan to achieve the future vision.
3. Execution Cycle: Execute the transformation plan. Enterprise leaders have
thoroughly considered the quality of thinking on enterprise transformation issues
Page 14 of 94
and have provided guidance for increasing value delivery for the maximum
benefit of the entire enterprise.
(Nightingale, 2009)
LAI@ Enterprise Transformation Roadmap
Figure 2
Enterprise Transformation Roadmap (Nightingale, 2009)
Most enterprises consider some of the key issues and questions in enterprise
transformation along with the methodologies and tools that aid in conceptualizing and
executing transformation in an integrated and holistic fashion. Figure 3 shows the
connection between transformation issues and enterprise methodology.
Page 15 of 94
Enterprise
Methodology
Transformation
Issue
7 Principles of Lean
Enterprise TNndng
How do I motivate and sustain
enterprise transformation?
How do I transform my
enterprise?
How do I assess my
progress?
What analytical tools can I
use to support ny decision
making?
How do I design my future
enterprise?
Figure 3
U.
Enterprise
Transformation Roadmap
Lean Enterprise Self
Assessment Tool (LESAT)
Enterprise Strategic
Analysis and
Transformation (ESAT)
Enterprise Architecing
Framework
Framework for Enterprise Transformation (Nightingale, 2009)
The Enterprise Strategic Analysis for Transformation through eight views sets up a
platform for the current state, creates a vision for the future state and develops an action
plan for prioritized transformation. LESAT and the EA views are used in concert with
ESAT to analyze and assess both the current and future states (Nightingale, 2009). The
interrelationship of these five enterprise methodologies is depicted in Figure 4.
Page 16 of 94
Enterprise Transformation Roadmap
Norte e
Low EnUnderaksan
castents100EA
pnt" a coordinae
Transforsadon Ptn
Envn
gn
Crt Tranfr oFtniPa
LESAT and
Framework
Assessment of
Current State and
Design of
State
ESAT
Methodology for Developing
Transformation Plan
Figure 4
Enterprise Transformation Framework (Nightingale, 2009)
1.1 Introduction of Enterprise Architectures (EA)
The Enterprise Architecture contains an eight views framework (Nightingale/Rhodes,
2004, Nightingale 2009). By evaluating organizations through multiple views, EA
presents organizations with a special emphasis on each one's particular attributes.
This framework has been extensively used in class projects for enterprises.
The eight views of Enterprise Architectures are: Strategy, Policy/Extemal Environment,
Process, Organization, Knowledge, Information Technology, Products and Services. The
following table describes each view of the enterprise and related operational
characteristics.
Page 17 of 94
Strategic goals, vision and direction of the enterprise including the business model;
:nterprise metrics and objectives
Policy/External The external regulatory, political and societal environments in which the enterprise
Environment
operates
Process
creates value for
Core leadership, lifecycle and enabling processes by which the enterprise
its stakeholders
The organizational structure of the enterprise as well as relationships, culture, behaviors
and boundaries between individuals, teams and organizations
The implicit and tacit knowledge, capabilities, and intellectual property resident in the
enterprise
Information
as the systems
Information needs of the enterprise, including flows of information as well
and technologies needed to ensure information availability
Product
Product(s) developed by the enterprise; key platforms; modular vs. integral architectures,
:tc.
Services
Services(s) delivered and or supplied by the enterprise, including in support of products
Table 1:
EA 8 views definitions (Nightingale, 2009)
The views are organized in a relational sense based on a generic enterprise, as shown in
Figure 5. In general, Strategy can influence Policy/External Factors as well as be
influenced by Policy/External Factors. Dashed lines indicate loose relationships that may
exist between views. Each view will be described within the appropriate section
(Mantorio, 2010).
Page 18 of 94
Figure 5
EA Eight Views (Nightingale, 2009)
1.2 Summary
The Enterprise Architecture Framework provides an integrated set of methodologies and
concepts that make these key enterprise principles executable. Elements of this
framework have been successfully utilized by a large cross-section of industries in their
enterprise transformations and research has shown them to be both domain independent
and scalable (Nightingale, 2009).
Page 19 of 94
2.0 Lean Advancement Initiative (LAI) Tools
The tools developed by the Lean Advancement Initiative were designed for organizations
to integrate lean practices to achieve high efficiency and eliminate waste. The concept of
lean enterprise was created first in the automobile industry but has since expanded to
many other industries.
MIT LAI defines a lean enterprise as "an integrated entity that efficiently and effectively
creates value for its multiple stakeholders by employing lean principles and practices"
(Nightingale, 2009). Implementation of lean methods requires a well-defined
examination of the enterprise's current state in order to create an effective transformation
plan.
2.1 Introduction of Lean Advancement Initiative Tools
LAI Tools contains an X-Matrix (Nightingale, Stanke, Bryan, 2008) and a Lean
Enterprise Self-Assessment Tool (Nightingale and Mize, 2002). LAI Tools reference
information can be found at http://lean.mit.edu
2.2 X-Matrix
An X-Matrix gives an overview of each factor's relationship with other factors. There are
strong, weak and none degree choices of alignment for the four axes of the tool: Strategic
Objectives, Stakeholder Values, Key Processes and Metrics.
The X-Matrix tool helps enterprises identify which the correlations between each factor.
Figure 6 is an X-Matrix template. The organization will fill in the corresponding number
based on each area's current state.
Page 20 of 94
Figure 6
X-Matrix Template
In Figure 7, the correlation between elements is shown as follows: blue
correlated, yellow
=
moderately correlated and white = little to no correlation.
anMMMM.
MMMM
Figure 7
Example of X-Matrix
Page 21 of 94
MM-
=
highly
Metric considerations enable enterprise transformation when systematically executed as
part of a transformation roadmap (Blackburn, 2009).
2.3 Lean Enterprise Self-Assessment Tool (LESAT)
The Lean Enterprise Self-Assessment Tool combines three sections for analysis with a
five level maturity index. These three sections are Lean Transformation/Leadership, Life
Cycle Processes, and Enabling Infrastructure Processes. The assessment includes
evaluation across 54 practices (28 in section 1, 18 in section 2, and 8 in section 3).
Level
Description
5
Exceptional, well-defined, innovative approach is fully deployed across the extended enterprise
(across internal and external value strems); recognized as best practice.
On-going refinement and continuous improvement across the enterprise; improvement gains
are sustained.
A systematic approach/methodology deployed in varying stages across most areas; facilitated
with metrics; good sustainment.
General awareness; informal approach deployed in a few areas with varying degrees of
effectiveness and sustainment.
Some awareness of this practice; sporadic improvement activities may be underway in a few
areas.
4
3
1
Table 2:
LEAST Maturity Level (LAI)
Page 22 of 94
Section I - Lean Transformation/Leadership
I.A Enterprise Strategic Planning (3 Lean practices)
I.B Adopt Lean Paradigm (4 Lean practices)
I.C Focus on the Value Stream (4 Lean practices)
I.D Develop Lean Structure and Behavior (7 Lean practices)
I.E Create and Refine Transformation Plan (3 Lean practices)
I.F Implement Lean Initiatives (2 Lean practices)
I.G Focus on Continuous Improvement (5 Lean practices)
Section II - Life-Cycle Processes
II.A Business Acquisition and Program Management (4 Lean practices)
II.B Requirements Definition (2 Lean practices)
II.C Develop Product and Process (3 Lean practices)
II.D Manage Supply Chain (3 Lean practices)
II.E Produce Product (2 Lean practice)
II.F Distribute and Service Product (4 Lean practices)
Section III - Enabling Infrastructure
III.A Lean Organizational Enablers (5 Lean Practices)
III.B Lean Process Enablers (3 Lean Practices)
Figure 8
Organization of LESAT Maturity Matrices (LAI)
2.4 Summary of LAI Tools
The LAI LESAT Development Team solicited input from a wide variety of LAI
consortium members to determine the set of factors considered the most important in
Page 23 of 94
transitioning to a lean enterprise. Figure 9 shows an overarching organizing structure for
the LESAT matrices consisting of three major sections (See Figure 9).
SediinI
Sectionil
Life Cyde Proses
Figure 9
LESAT Architecture (LAI)
This architecture combines the following three elements:
e
Lean Transformation/Leadership - the processes and leadership attributes
nurturing the transformation to lean principles and practices
e
Life Cycle Processes - the processes responsible for the product from conception
to post delivery support
* Enabling Infrastructure - the processes that provide and manage the resources
enabling enterprise operations
Page 24 of 94
3.0 CLIOS Process
3.1 Introduction of the CLIOS
The CLIOS acronym stands for Complex, Large-scale, Interconnected, Open, Sociotechnical systems; there are a class of engineering systems which are sociotechnical in
nature with wide-ranging social impact and have wide technology as a important
component. Professor J. Sussman led a CLIOS process team at MIT, applying this
framework to enterprise-level transportation systems. The CLIOS process was created
with the intention of using it to solve a wide variety of problems in which technical
systems interact with social and policy systems, based on Dodder et al, 2005. The CLIOS
Process can be used as an organizing mechanism for understanding a CLIOS System's
underlying structure and behavior, identifying and deploying strategic alternatives for
improving the system's performance, and monitoring the performance of those strategic
alternatives (Sussman et al. 2005).
Sussman's work on Complex, Large-Scale, Interconnected, Social-technical (CLIOS)
Systems stresses nested complexity, where physical systems such as transportation
systems are "nested" within an institutional architecture (e.g., Sussman et al., 2009).
Often the design of the institutional architecture specifies which individuals or agencies
have intermediate and final authority for making strategic decisions, and the jurisdiction
over which they can exercise that authority. (Dunn, 2010)
3.2 CLIOS Process
Sussman, et al. (2009) introduced the notion of CLIOS systems, which are characterized
by several types of complexity, including the structural and behavioral complexity
stressed by Simon, and by evaluative and nested complexity, which have been tested
through various transportation case studies.
Researchers from the Massachusetts Institute of Technology have been applying the
CLIOS process to analyze a broad range of engineering systems. Systems that the CLIOS
process has been used to evaluate include supply chain modeling, transportation
Page 25 of 94
planning, energy distribution, air combat, and telecommunications (Sussman, Sgouridis,
and Ward, 2005).
An enterprise's ability to describe, analyze, or improve CLIOS systems using traditional
analytical approaches is limited by its complexity. Moses (2004) observed that
"Engineering Systems are systems designed by humans having some purpose and are
composed of interacting components." A CLIOS System is an engineering system, but its
social component makes it more broadly applicable than other general engineering
systems. Though the CLIOS framework has been used widely in transportation systems,
per Sussman team's research, it can be applied to other areas.
The CLIOS process is an approach for representing, evaluating, and implementing
changes to CLIOS systems and has been applied in a number of contexts, including
transportation systems. Although the CLIOS Process provides a framework for capturing
various types of complexity, it does not suggest any specific qualitative or quantitative
approaches. Instead, it allows for the construction of a unique methodological approach
for representing and evaluating systems (Dunn, 2010).
The CLIOS Process consists of three stages:
-
Representation of the CLIOS System structure and behavior,
e
Design, Evaluation and Selection of CLIOS System strategic alternatives, and
-
Implementation of the selected strategic alternatives.
The CLIOS process is represented conceptually (Sussman, 2006) as a Christmas tree and
its ornaments. Using this mental model, the tree represents the overall process and the
ornaments represent the specific tools (e.g. benefit-cost analysis, probabilistic risk
assessment, system simulations, stakeholder analysis, scenario planning, design structure
matrices, etc.) that one can use for specific steps in the overall process. No matter what
system is being analyzed, the steps
in the process remain the same and
process(ornaments) are selected for the particular CLIOS System being considered.
Page 26 of 94
The Figure 10, Figure 11 and Figure 12 present the CLIOS process in 12 steps divided
into three phases. For detailed information, see the CLIOS Process User Guide (Sussman
at el. 2009).
PHASES
STEPS
REPRESENTATION
1. Describe CLIOS System:
Checklists & Preliminary
Goal Identification
2. Identify Subsystems in
Physical Domain & Groups
on institutional Sphere
3. Populate the Physical
Domain & Institutional
Sphere
4A. Describe Components
4B. Describe Links
5. Transition from Descriptive to
Prescriptive Treatment of System
Figure 10 The Twelve Steps of CLIOS Processes (Sussman, at el, 2009)
Page 27 of 94
1. Describe CLIOS System:
Checklists & Preliminary
Goal Identification
A
B
e
2. Identify Subsystems in
Physical Domain & Groups
on Institutional Sphere
3. Populate the Physical
Domain & Institutional
Sphere
4.Desenibe Components
4B. Describe Links
6.Transition from Descriptive to
Prescriptive Treatment of System
Figure 11 Iteration of CLIOS Steps (Sussman, at el 2009)
A typical CLIOS System has the following characteristics:
Complex: "A system is "complex" when it is composed of a group of interrelated
units... for which the degree and nature of the relationships is imperfectly known"
(Sussman et al., 2009).
Page 28 of 94
e
Large-scale:The effects of the system are large in magnitude or the system itself is
large (Ward, 2005).
e
Interconnected: Subsystems are inter-connected to each other, usually including
feedback loops, rather than existing as independently operating entities. As an
example, one could point to the relationships between transportation systems,
energy systems and the global climate system (Sussman et al., 2009).
* Open: The system has important political, social, engineering, and economic
aspects.
e
Socio-technical: The system interacts between social and technical components
* System: A group of related elements making up a whole (Ward, 2005). It is a
platform to present layers of relationships among elements.
Figure 12 The CLIOS Process and Metaphor (Source: Sussman, Sgouridis, and
Ward 2005)
Page 29 of 94
3.2.1
Stage 1: Representation
The representation stage is primarily diagrammatic in nature. Diagrams are used to
represent the structure and behavior of the CLIOS System by graphically illustrating the
system components and interactions in the physical domain, on the institutional sphere,
and between them. Accompanying text describing and explaining the CLIOS System
diagrams can improve comprehension. This allows the users of the CLIOS Process to
understand the CLIOS System and establishes the basis for completing the second and
third stages of the CLIOS Process.
I
__
_
__-__
__
_|_
_
1. Describe System: Issue Checklist and
Goal Identification
I
--> 2. Identify Major Subsystems of the
Physical Domain and Major Actor Groups
on the Institutional Sphere
3. Populate the Physical Domain and the
Institutional Sphere on the CLIOS Diagram
I
4A. Describe Components on
the Physical Domain and
Organizations on the
Institutional Sphere
4b. Describe Links Among
Components And Organizations
5. Seek Insights about System
\I,
Behavior
Figure 13 CLIOS Representation Stage (Ward, 2005)
3.2.2
Stage 2: Design, Evaluation and Selection
Having considered the CLIOS System from the standpoint of its structure and behavior
during the Representation stage, the next stage focuses on the design, evaluation, and
selection aspects of the CLIOS Process. We therefore begin to consider in greater depth
the evaluative complexity of the CLIOS System, in order to identify opportunities for
improving both the physical domain and the institutional sphere. This culminates in the
Page 30 of 94
development of a robust bundle of strategic alternatives. Among these strategic
alternatives are organizational and institutional changes that may be necessary to meeting
the CLIOS System goals (defined in Step 1, and to be reconsidered in Step 6).
As part of Stage 2, we can also proceed with using the appropriate (quantitative) models,
including refined system goals and identified performance measures, as guidance for
model scope and scale. These models should be validated to evaluate the current state of
the system; they will subsequently serve as a basis for comparing strategic alternatives.
The models can be the quantitative analog of the qualitative representation built in the
representation stage, or they can be constructed from scratch simply by using insights
from the qualitative representation. Two basic model categories can be used: casespecific (i.e., models that track limited facets of the CLIOS System on the component or
subsystem level; in transportation a traffic simulation would be such a model) and
system-wide (i.e., models that aim to describe interactions at the CLIOS system level,
such as a system dynamics simulation that combines economic, environmental and
transportation interactions). Ideally, the system-wide models should integrate inputs from
the independent models in a system representation consistent with the qualitative insights
that are gained from Stage 1.
Z
0
0
>
6. Identify Performance Measures,
Refine System Goals, and Build
Quantitative Model
7. Identify and Design
Strategic Alternatives for
Performance Improvements
8. Flag Important Areas of
Uncertainty
9. Evaluate Strategic Alternatives And Select Robust
Bundles That Perform "Best" Across Uncertainties
Figure 14 CLIOS Design, Evaluation and Selection Stage(Ward, 2005)
Page 31 of 94
3.2.3
Stage 3: Implementation
Once a bundle of promising strategic alternatives is selected, the next crucial action is to
design a plan for implementation. Many analyses come to an end at Step 9 with a list of
recommendations, but with little guidance as to what obstacles might arise in the
implementation of the recommended actions, and little information as to how the political
realities will affect the actual deployment.
10. Design Strategy
for Implementation in the
Physical Domain and Implement
11. Design Strategy
for implementation in the
Institutional Sphere and
Implement
12. Post-Implementation Evaluation
and Modification
Figure 15 CLIOS Implementation Stage (Ward, 2005)
Table 3 presents the overview of the three stages and key outputs.
Stage
Key Ideas
Representation
Design, Evaluation,
.
utputs
-
Understanding and visualizing
the structure and behavior
Establishing preliminary goals
e
Refining goals aimed at
0
improvement of the CLIOS
System
Developing bundles of strategic
alternatives
and Selection
ystem description, issue identification,
oal identification, and structural
oareientation
epresentation
Identification of performance measures,
identification and design of strategic
alternatives, evaluation of bundles of
tegic alternatives, and selection of the
est performing bundle(s).
Implementation
Implementing budles of strategic
mplementation strategy for strategic
alternativs;
ternatives in the physical domain and
allowing-through-changing and
e institutional sphere, actual
monitoring the performance of the CLIOS mplementation of alternatives, and postSystem
mplementation evaluation.
Table 3:
Summary of CLIOS Three Stages (CLIOS Process User Guide, 2009)
Page 32 of 94
3.2.4
InstitutionalOrganization
Institutional organization refers to the organizations that oversee the physical
transportation infrastructure system and their relationships with one another.
Based on the characterization of nested complexity by Sussman et al. (2005), institutional
organization can be considered as a sphere surrounding the physical transportation. It can
be categorized with the subsystems of the physical domain. Though Institutional Sphere
is the only layer. There are more layers under physical domain existing in the sub
systems. (see Figure 16).
'p Institutional
CLIOS System
Sphere
boundary
-
oPhysical
Domain
Component -
Figure 16 Physical Domain in CLIOS System embedded in an institutional sphere
(Adapted from Sussman, et al., 2005)
Page 33 of 94
4.0 Analysis
Comparison between EA and CLIOS Process
Both EA and CLIOS frameworks are built for complex enterprise systems and can be
successfully applied in a variety of contexts. The EA 8 views framework has built a
richer understanding of the enterprise through the various perspectives as well as
developed future state enterprise architecture options (Montoya, 2010). The CLIOS
process has helped transportation planning organizations with its capability to design and
implement sustainable transformation systems and provide guidance on how these
institutions can be developed (Zakaria, 2004). Between regional strategic transformation
planning and regional planning architecture protocol, the CLIOS process has widely been
used in transportation systems.
A comparison of the two methods is shown in the following table.
ystem
tructure
CLIOS
EA
Engineering systems with wide-ranging Enterprise-level transformations
social and environmental impacts.
in large complex socio-technical
_nterpnses
Process
Presence of "Nested Complexity",
onsist of a set of
which results when a physical domain nterdependent methodologies,
is nested within and interacts with an
ools and enterprise principles
nstitutional sphere, where both are
at support holistic enterprise
complex;
transformation
Designed to be a modular process that
be customized and expanded as
needed
Page 34 of 94
Stages
1. Representation of the CLIOS
System structure and behavior
2. Design, Evaluation and
1. Strategic Cycle
2. Planning Cycle
3. Execution Cycle
Selection of CLIOS System
8 views: Strategic, Information
Technology, Knowledge, Policy,
3. Implementation of the selected Product, Services, Organization
and Process
strategic alternatives
Strategic altemnatives
Intention
1. Provide a structure for
undertaking the analysis
onduct the enterprise systems
analysis and design of various
industry and governmental
2. Increase the amount of rigor and organizations;
validity in the analysis
3. Facilitate the identification of
povide transformation plan to
bring enterprise to future state
alternatives that are relevant to
the actors on the institutional
sphere
Complexity
Basic
Structures
1. Behavioral
1. Behavioral
2. Internal
2. Internal
3. Evaluative
3. Evaluative
4. Nested
4. Nested
3 Stages: Presentation; Design,
Evaluation and Selection;
Implementation and adaptation
12 Steps
Table 4:
5 Principles of Enterprise
Thinking
Enterprise Transformation
Roadmap Lean Enterprise Self
Assessment Tool (LESAT)
nterprise Strategic Analysis for
Transformation (ESAT)
Enterprise Architecting
Framework
Comparison between EA and CLIOS
Page 35 of 94
5.0 Merging Process
5.1 Strategic Planning Stage
In CLIOS, before the system can be represented, the system needs to be identified at step
1, which includes setting up boundaries for the system before analysis can proceed,
creating a vision of the system and understanding stakeholder issues. This step involves
iterative processes to help stakeholders reframe concerns and to adjust system
boundaries. Often in the middle of the process, stakeholders see the need to modify the
scope and update the questions. Step 1 is the critical place to gather all this information.
After formalizing the scope of the system, step 2 of the CLIOS process is to identify the
subsystems. This level of identification of subsystem could be by technical discipline,
function, logical or sequential arrangement. As can be seen from several students' theses
applying the CLIOS process in transportation (e.g. in Mexico City and Puerto Rico),
there are many common subsystems: railway subsystem, ferry subsystem, air subsystem
and highway subsystem.
Step 3 starts with basic development to create presentation of the system. Extension of
Step 2 identifies subsystems to build up the institutional sphere.
Step 4 contains two elements: Step 4A is to describe components. In the CLIOS system
definition, a component can be one of three possibilities: a plain component, a policy
lever, or a common driver. A policy lever is a connection that an institution can use to
drive the system, which provides a way for policymakers to manage the system. A
common driver is a component that is shared across multiple subsystems and may be
exogenous to the system (Ward, 2005). Step 4B is to describe links among components
and organizations, which can involve describing the characteristics of the link, its
direction, timeline, or uncertainty in the relationship.
Step 5 in the representation phase is to seek insight about system behavior. The CLIOS
Process User Guide mentions that many insights will be made just through the act of
Page 36 of 94
creating the representation, and provides questions that can guide the practitioner towards
gaining greater insight (Sussman et al., 2009).
In sum, step 1, 2 and 3 constitute structure presentation. Steps 4 and 5 constitute behavior
presentation.
On the EA transformation roadmap, the business case for transformation and leadership
engagement are part of the strategic cycle (Nightingale, 2009). In EA eight view process,
before analyzing any views of the organization, the enterprise should be processed
through the strategic cycle in the enterprise transformation map. In the strategic cycle, the
enterprise will bring leadership on board, determine strategic imperatives in order to
understand enterprise transformation scope, identify stakeholder value and leverage
transformation gains. In the strategic cycle, it is very important to not only engage
leadership from very beginning, but to also let leadership understand the long-term
challenges for the enterprise and the impact of the leadership's commitment to the plan.
As we can see in Figure 15, there is a connection between CLIOS Process Step 1 and the
"engage leadership in transformation" section, which will set up the scope and agreement
with leadership. This will help out later on in the process. Between CLIOS Process Step 2
and the "determine strategic imperative" section, there is a focus on identifying
stakeholder values and identifying objectives. CLIOS Process Step 3, 4 and 5 are very
similar to EA's Planning Cycle.
Page 37 of 94
LA
Oan Enterprise Transformation Roadmap
Determine
Strategic
Imperative
Articulate the CaseforTrawsforno .
&Cowey"Urncy
Focuson SuioinerValue
*LeverageeTrmufornan ins
Thinfg
Engage Leadership* Cuimate Enterprise
inTransfonnation * ObtainExecutie Buy-In
*EstatAish Executive Transtannation
Counci
CLIOS Process
1. Decri~eCSSsifi
J
4-+
Planning CyclE
Planning stage: both framework gathering requirements to outline goals/visions;
prepare for the enterprise transformation; utilize representation stage
to set the groundwork
Figure 17 CLIOS and EA merging step - Strategic Planning Stage
(After Nightingale, 2009 and Sussman, et al. 2009)
5.2 Planning & Transformation Stage
CLIOS Stage 2 develops a set of strategic alternatives that can be used on the system to
meet system goals that are grounded in the reality of how the system works, rather than
alternatives based on ideological grounds (Ward, 2005). These alternatives are also
evaluated considering performance, uncertainty, political feasibilities and other factors. It
resembles EA eight views in that it too identifies the current state, then creates multiple
enterprise architectures before evaluating and selecting the most feasible or suitable one.
Step 6 in Stage 2 is parallel with Step 1 in Stage 1, which includes negotiation with
stakeholders on how to measure system performance; this focus on evaluation metrics is
similar to LESAT methods. It may not be easy to reach an agreement on the best
performance measurement, but this is a step towards creating measurements which will
eventually help to define and reach system goals. Step 7 develops alternatives for those
Page 38 of 94
goals. The CLIOS Process User Guide identifies two approaches for alternatives:
"outside in" and "inside out" methods. In parallel with Step 7, Step 8 identifies the
uncertainty that may stem from common drivers, unclear interactions or political factors.
Step 9 requires stakeholders to select the best option considering alternatives from Step 7
and uncertainties from Step 8. This step is exactly like the EA framework since it selects
the best fit EA after evaluating the current state, lists multiple EA options and chooses the
"best" one.
In EA there is a planning cycle during which both the current state and future state are
analyzed and defined, and a transformation plan to achieve the future vision is conceived
(Nightingale, 2009). After completing the strategic cycle, stakeholders will work in
multiple areas in planning cycles: understanding the current state; creating the future state
vision & future enterprise; aligning structures and behaviors, and creating a
transformation plan.
In this stage, there are a few similar steps in the CLIOS process and EA frameworks
which can conveniently be merged. CLIOS process Steps 3,4, 5 and 6 analyze the
existing enterprise environment, similar to the EA current state analysis. Steps 7, 8 and 9
align with EA requirements alignment and transformation plan. Meanwhile, there are
more detailed EA transformation steps than CLIOS steps, such as the identification of
improvement focus areas and the synchronization of a detailed implementation plan.
There are no equivalents between EA and CLIOS process, though there are different
approaches for some steps and we can understand how they can work together.
Page 39 of 94
Step 2 of 3
Identification, design and create plan for transformation
CLIOS Process
F.A Exe c u ti or, Cycle
Figure 18 CLIOS and EA merging step - Planning and Transformation Stage
(After Nightingale, 2009 and Sussman, et al. 2009)
5.3 Execution Stage
This section shows the optimal meshing of EA and CLIOS frameworks in order to
execute and implement a final plan, which has the most similar process and may
synchronize information with previous steps to obtain a feasible plan.
The CLIOS process chooses a strategy for implementing the selected alternatives and
feeds the results back into the process (Sussman et al. 2009). By this final phase, there are
enough loops to keep stakeholders and leaders engaged and in agreement with the final
selected alternatives, which is clearly based on effectiveness of Step 9. Step 9 shares
similarities with the EA planning cycle, which selects the alternative EA after evaluating
all options.
Step 10 in CLIOS focuses on the strategy design for the physical domain, which can be
quantitative. Step 11 develops a strategy for the institutional sphere in order to improve
system outcomes (Sussman et al., 2009).
Page 40 of 94
In the EA framework definition, an execution cycle will put the plan into practice. It has
been employed by enterprise leaders to enhance the quality of thinking on enterprise
transformation issues and has provided guidance for increasing value delivery for the
maximum benefit of the entire enterprise.
Lng-Tam
Nurture
CAncdn
Transformation
& Embed
Enterprise Thwnng
Implement &
Coordinate
Tranf3oation
plan
EA Planning Cydle
man
g
9flTam
Cooftewe
This section is the best mesh-up for
Two framework as transformation
Plan(EA) and CLIOS Implementation
Are for the same process, synchronize
Information with previous steps to obtain
the feasible plan.
Step 3 of 3
CLIOS Process
Design and Implement Plan for:
10. Physical Domain/Subsystems
11, Institutional Sphere
Alte rnatives for CLOS Systemi
Figure 19 CLIOS and EA merging step - Execution Stage
(After Nightingale, 2009 and Sussman, et al. 2009)
5.4 Summary
Based on the previous analysis, there are strong correlations between the CLIOS and EA
processes that promote their harmonization. In the strategic planning stage (EA) and the
planning & transformation stage (CLIOS), we see a few repetitive steps in both
frameworks. Also, we see the mutual benefits for both frameworks. CLIOS specifically
provides a step to design the physical domain, which could help EA to implement its
framework in physical architecture, such as green architecture design and urban planning,
Page 41 of 94
transportation systems and energy related areas. If merged with EA, the CLIOS
framework could take advantage of the detailed transformation roadmap, LESAT and the
strategic focus on enterprise development.
There are a few areas where merging is likely to be less successful. CLIOS has been
validated in and successfully applied to transportation systems. The EA framework as
well as the transformation roadmap and LESAT have been presented as a whole package
through enterprise development. There are unique characteristics in each framework. A
forceful merging attempt that does not consider the strength of individual processes will
not provide the best outcomes but instead generate enterprise waste.
Page 42 of 94
Application: Veterans Affairs Case Study (Wang, et al.
2010, 2011)
6.0 Introduction
The Veterans Health Administration (VHA) is a federal government entity within the
Department of Veterans' Affairs and is one of the largest healthcare providing networks
operating in the United States. The purpose of the VHA is to provide healthcare to
American veterans and qualified members of their families. The administration operates
over 1,400 sites nationwide providing treatment to over 5 million veterans.
Approximately 240,000 people are employed by the VHA which has an annual budget of
$3.1 billion.
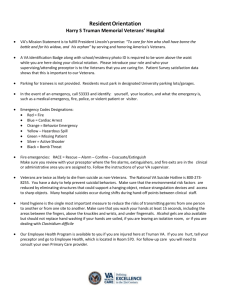
The administration is divided geographically into 23 Veteran Integrated Service
Networks (VISNs). Veterans typically receive care at a facility within the VISN where
their primary residence is located. However in instances when veterans are away their
primary home location, they are entitled to receive care within the VISN where they are
located.
20*
RI
15
DC
H22
Philippine Islands
Guam
Virgin Islands
A-I
Amrican
Figure 20 VISN Map
Veterans travel outside their primary VISN's coverage for extended timeframes for a
multitude of reasons. Some veterans are "snowbirds" and migrate to warmer climates for
the winter months. Others travel and remain with friends or family members for extended
times. Still others travel extensively as part of their jobs (ex truck drivers) while some
veterans are homeless and travel from place to place on a frequent basis. Traveling
veterans from within each of these categories often require care ranging from emergency
services to routine prescription refills and blood tests.
The VHA recognizes the need to assist veterans requesting health care while traveling
away from home. In a directive issued in 2007, the VHA stressed the need to "maximize
continuity and consistent, appropriate, and safe care for traveling veterans." (Department of
Veterans Affairs, 2007).
Page 43 of 94
This project is the result of a continuing interaction between the VHA and the
Massachusetts Institute of Technology (MIT) in an effort to use to improve VHA
operations. Project topics are provided by the Veterans Engineering Resource Center
(VERC). A previous project looked to improve inter-hospital transportation operations
within VISN 1. While this project applies to traveling veterans across all VISNs, Mr.
Mark Lyons, RN, BSN (VISN 20 VIRS Coordinator) served as the sponsor and primary
conduit for information and support. Face-to-face research was conducted within VISN 1
facilities since they operate where MIT is located. Ms. Lynne Cannavo (VISN 1)
provided the team with access to data and personnel in order to increase understanding on
the issues surrounding providing care to traveling veterans.
7.0 The Enterprise Today
7.1 Stakeholders
7.1.1 Stakeholder Identification
A key component of the Enterprise Strategic Analysis and Transformation (ESAT)
methodology is identification of an enterprise's stakeholders. The following table
categorizes each of the primary stakeholder groups. (See Appendix C)
End User
The end users of the enterprise are the veterans and their families that seek out and
receive care while away from their home VA medical facility and provider. As discussed
in the introduction, veterans need care while away from home for a number of reasons.
Sometimes the need is driven by a recurring care requirement while other times the need
is due to a mishap or unforeseen circumstance.
Suppliers
Suppliers within the traveling veteran enterprise are primarily employees of the VHA
including the care providers (doctors, nurses, pharmacists, and assistants) as well as
administrative staff members such as eligibility clerks. Two very important stakeholder
groups within the supplier category are the referral case managers and the primary care
providers. Both play crucial roles in ensuring quality care is delivered to veterans and
their families while away from their home facilities.
Leadership
Leadership stakeholders within the enterprise exist at all levels from the clinic/facility
level to the entire department of Veterans Affairs. VISN-level leadership are the
stakeholders best positioned to lead change across the traveling veteran enterprise.
External Stakeholders
While the traveling veteran enterprise is only a subset of the larger VHA enterprise, it
shares the same external shareholders who hold significant sway and authority over the
organization. These include the taxpayers who provide the funding for the enterprise as
well as the unions who work to safeguard the interests of their members.
Page 44 of 94
7.1.2 Stakeholder Value Exchange
Stakeholder analysis provides an opportunity to examine the value exchange between
stakeholder groups and the enterprise. This is useful because it provides a method to
explore the performance of the enterprise against what is important to the participants. In
addition to identifying misalignments, understanding the core values of the stakeholders
is important when proposing potential corrective actions and changes. Prior to exploring
stakeholder value exchanges, the roles and responsibilities of Care Providers (Doctors,
Nurses, Nurse Practitioners, and Physician's Assistants), Traveling Veterans (patients),
Eligibility Clerks, Primary Care Managers, and Referral Case Managers were examined.
The following tables provide a summary of the roles and responsibilities of each of these
stakeholder groups as well as the individual value exchanges that occur with the
enterprise.
Data on value exchange within the current state of the enterprise was obtained through
the use of a survey (included as Appendix A). There were 87 respondents with responses
coming from each of the stakeholder focus groups.
MCare Provider - Doctor
ECare Provider - Nurse
OCare Provider - Nurse Practioner
OCare Provider - Physician's Assistant
OReferral Case Manager
2.7%
OPCMM Coordinator
OVISN-level employee
2.7% 4.0%
0Other
Figure 21 Stakeholder Group Survey Participation (87 total respondents)
The survey asked respondents from each stakeholder group to rank a set of values based
on the following two questions:
* Please rank the following aspects in providing or facilitating care to traveling
veterans across VISNs? (1 = not that important to you, 5 = critical part of your
job)
* When handling traveling veterans across VISNs, please rank how effective the
VA currently is in the following aspects (1 = not effective, 5 = very effective).
Page 45 of 94
Using the feedback provided via the survey, each value was ranked from highest to
lowest with a value of 1 representing the highest priority and 13 as the least. Ties in
rankings were given the same value. The focus of the gap value analysis was on
Physicians, Nurses, RCMs, and PCMs because they are the 4 primary stakeholders
groups (in addition to patients) within the Traveling Patient Enterprise. (See Appendix E
for a synopsis of the results across the four stakeholder groups.)
High
0U
C.
E
C
0
Low
Relative Importance of the Stakeholder to the Enterprise
High
Figure 22 Current State Value Delivery by the Enterprise to Key Stakeholders
To further depict the current state of stakeholders within the traveling veterans enterprise,
a waterdrop model was created. In this visualization, each stakeholder is shown as an
ellipse. The key below highlights the degree of collaboration among the stakeholder
groups. In the stakeholder value elicitation, effective communication was an area
mentioned by all stakeholder groups where the current state enterprise was not meeting
stakeholder needs.
7.1.3 Process Description
There are two primary processes within the Veterans Health Administration Traveling
Veteran Enterprise. The key criteria for which process a traveling veteran follows is
whether the veteran's travel to a new location is permanent (A) or temporary (B). We will
describe each of these two primary processes below, including how each process
identifies and verifies eligibility, transfer medical records, assigns veterans to a Primary
Care Provider, provides patient care, and updates the veteran's medical records.
7.1.4
Process Analysis
Permanent Transfer Process
Page 46 of 94
When a veteran's travel culminates in a permanent transfer to a new location, the process
includes the following steps:
* Identification and verification of eligibility
" Transfer of electronic medical record from previous home facility to current
facility
* Assignment of the veteran to a primary care provider
* Patient care
* Update and maintenance of electronic medical record
Identificationand verificationof eligibility
Upon arrival at a new facility, a veteran's identification and eligibility for care are
verified. If the veteran has previously contact with the VHA system, this step in the
process can be completed very quickly with a cursory review of identification and a
lookup of the veteran's social security number. In cases where the veteran has not
previously engaged the VHA system, this process can take longer involving the review of
the veteran's DD Form 214 Certificate of Release or Discharge from Active Duty. This
document is issued upon a military service member's retirement, separation or discharge
from active-duty military and includes information necessary to initially determine
eligibility for VA services. The determination of eligibility is conducted by an eligibility
clerk. Completion of this step can be delayed by insufficient identification or
documentation. In such cases, the eligibility clerk will work with the veteran to validate
eligibility which sometimes entails the request of documentation from third parties such
as the Department of Defense. In summary, our research indicates that this step in the
process is typically performed very quickly in a manner of minutes, but in cases where an
individual is new to the VHA system and/or has not provided sufficient documentation,
the time to complete this step may stretch into hours and days. The stakeholders we
interacted with indicated very few problems stemming from this step in the process. It is
important to note that no veteran is ever denied urgent or emergency care while eligibility
is being verified. The medical well-being of the veteran takes precedent while eligibility
is confirmed.
Transfer of electronicmedical recordfrom previous home facilityto currentfacility
Medical records within the VHA system are electronically stored. Electronic records are
usually only accessible to providers within VISN where the veteran's home facility is
located. When a veteran travels and permanently transfers to a new facility within a
different VISN, the electronic record must also be transferred within the database system.
This transfer is typically done by either the referral case manager or a member of the new
facilities administrative staff via an electronic request known as a HINC or a PDX. Our
research found the following description the of the PDX process step:
Authorized users of PDX can request a patient's data from specified sites.
The request-receiving site can elect to answer the request automatically,
or to review it manually prior to responding. Demographic and eligibility
data can be uploaded into the requesting site's VistA system. Other PDX
information, such as prescriptions, cannot be integrated into the
Page 47 of 94
requesting site's VistA system and is typically printed out for review. An
unsolicited "push" of data between sites is also possible. Data "push" is
useful when patients notify their current medical center of their plans to
move their care to another site. PDX response time varies from minutes to
weeks. Long delays can occur when the manual request review process is
delayed. (Steven H. Brown, 2003)
In contrast to the above description, the stakeholders we interviewed indicated that this
process normally takes only minutes to hours. Once a record has been transferred, it is
visible to care providers within the new facility and surrounding VISN.
Issues involved within this process step center around the formatting of the information
within the electronic record. A VISN 1 physician indicated that different regions and
facilities record information differently which slows the review of the medical record by
a care provider unfamiliar with the differing format. This observation was confirmed by
the stakeholder survey results.
Assignment of the veteran to a primary care provider
When a veteran permanently transfers from a facility in one VISN to a facility in another
VISN, they are assigned a new primary care provider at the new facility. The assignment
of the veteran to a primary care provider's panel is accomplished by a PCMM
coordinator. This assignment is sometimes facilitated by referral case manager on both
ends of the transfer to ensure continuity of care when the veteran's intent to transfer is
known in advance. Unless they obtain approval, each veteran can only have one Primary
Care Provider (PCP) at a time, so they are formally turned over to this new PCP.
Patient care
This process step is where the veteran receives the medical care that he or she requires. In
the case of a permanently transferring veteran, this care is provided in the same manner
as care is provided to all veterans within the VISN. Although there are issues with
efficient resource allocation among facilities internal to a single VISN, this issue is not
within the scope of this analysis. Since this is the step which embodies the mission of the
VHA, it has the most personnel involved to include care providers and administrative
support staff.
Update and maintenance of electronicmedical record
As with any patient, once care is provided the veteran's electronic medical record is
updated by the care provider and/or the administrative support staff. It appears that there
is no detailed standard on where information is placed within a record and the format in
which it is recorded. The documentation standards that do exist appear to exist at the
facility level and are promulgated via word of mouth.
Temporary Care Process
When a veteran's travel culminates in a temporary transfer to a new location, the process
includes the following steps:
Page 48 of 94
*
Identification and verification of eligibility
Access electronic medical record
e
Assignment of the veteran to a care provider
e
Patient care
* Update electronic medical record
e
Notification of primary care provider at home facility
e
Identificationand verificationof eligibility
This process step differs little from the corresponding process step within the permanent
transfer process scenario. One difference is that there may be more communication
between the facilities in different facilities to ensure an effective hand-off of the veteran.
This is done by either the referral case manager or social workers enlisted to help by the
referral case managers.
Access electronicmedical record
As in the permanent transfer case, an electronic medical record is only viewable within a
veteran's home VISN until a request is made by the facility providing temporary care for
access. This is also done via the PDX process. In contrast to the permanent transfer case,
the record is not "transferred" to the new facility. The record's attributes are changed
allowing it to be viewed and updated by personnel within both regions. As in the
permanent transfer process, an issue within this process step is the formatting and
placement of the information within the electronic record which is not consistent across
facilities and regions. Another issue is access to information that resides outside the VHA
electronic medical record. This information may be in the form of records held by a
outside health care provider/facility or background information within the home
location's primary care provider's personal memory. Extemal communication methods
such as encrypted e-mail and faxes are often utilized to provide this information to the
care provider who is supporting the veteran in the temporary location. Often, it is the
referral case manager that facilitates this transfer of information.
Patient Care
As with in the permanent transfer process, this process step is where the veteran receives
the medical care that he or she requires. Care provided to travelers who are seeking
temporary care while away from their home facilities can be categorized into four
scenarios as shown in the repeated chart below.
Page 49 of 94
Scenario
Example
Pecntage of cases
Care / Services
IProvided
Specifi; Tme-Limited,
Simpl Needs
INR, Medicattn
30
*
Specifi; Time-Limited,
Complex. Cannot Wait
Cancer-care, Follow-up
to Aortt Aieur ysm
40
Specifi; Not Tim
imited. Complex, Cannot
wait
Diabetes, Congestie
Heart Failure, COPD
20
- Appointment
- Back & Forth
Consultattns 4 IM
- Record review
* Dual enrollment
* Managed care
General, Not TimeLimited, Not Complex
Routie amnual exams,
consults
10
Table 5:
Consult
-Lab Order
* Appointment
- Record review
- Consultatins
*Appointment
Care Scenarios
In contrast to the permanent transfer case, the allocation of medical resources is more
complicated due to the temporary nature of the veteran's visit.
Specific, Time-limited Simple Needs
In this scenario, the traveling veteran's care needs are straight-forward. Typically the
veteran is looking to have a prescription renewed or a test conducted that cannot wait
until he/she returns to her home facility. However, this scenario can pose issues since
most care providers will not agree to provide care without first conducting at least a
review of the veteran's medical record. Due to the traveling veteran not having a primary
care provider in the facility, the question of who will provide the care arises. Solutions
implemented in the current state range from the very inefficient (use of the Emergency
Department) to a much more efficient "snowbird" window that provides basic care needs
specifically for veterans seeking temporary care. For instance, one pharmacist from VISN
18 described the following best practice for receiving medications:
"Asfar as pharmacy goes, a traveling veteran policy was created where
approved clinical pharmacists can provide up to a 2 week supply of
home medications if a patient needs a bridge while visiting and will be
returning home within that time frame. We also have points of contact
set up for triage and providers if pharmacy is unable to complete the
request by the patient"
However, this has not been deployed effectively across all VISNs. Of all temporary
traveling veteran cases, these are typically 30% of the total although they can be a much
larger portion in areas that experience significant seasonal migrations such as Florida and
Aizona.
Specific, Time-limited, Complex, Cannot Wait
This scenario often arises as a result of a veteran moving in with relatives or friends
during a recovery period following cancer care, or cardiac procedures. In contrast with
Page 50 of 94
the first case where care provided is commonly a single-shot event with little care
provider interaction, this scenario is likely to result in the need for recurring visits as well
as communication between home facility and temporary facility care providers and
referral case managers during the recovery period. A group of referral case managers
estimated this scenario to be roughly 40% of all traveling veteran cases.
Specific, Not time-limited, Complex, Cannot Wait
This scenario is one where the veteran's health is not under control forcing him/her to
seek immediate care in the temporary location where they reside for long periods of time.
One example would be a veteran who spends 5 months in a summer home location who
has diabetes that is not under control. In this scenario, the veteran requires longer-term
complex care and care management that will span over a longer time period. Continuity
of care in the temporary location is very important due to the chronic nature of the
ailment. In order to provide this continuity of care, a veteran in this circumstance is
sometime placed upon a primary care provider's panel at the temporary location. This has
the effect of "dual-enrolling" the veteran with respect to primary care providers. This
solution is not optimal since placing a temporary veteran onto a panel takes up a panel
slot that would have been utilized by a local veteran. This has been recognized by the
VHA which has sought to minimize dual enrollment:
Veterans sometimessplit their principal residence between two locations and
spend significant amounts of time at each. If such patients have complicated
care requiring close on-going care management, it may be appropriate to
have an identified PCP at VHA health care facilities in each of the two
geographically separated residences. However, this practice should be
minimized. (Department of Veterans Affairs, 2007)
This same group of referral case managers estimated that this type of case represents
about 20% of temporary care traveling veteran scenarios.
General, Not time-limited, Not complex
This last scenario is the least common among traveling veterans; approximately 10%. It
involves care that could often reasonably be delayed until a veteran has returned to his
home location. However, since veterans have definitely eamed the right to care at any
VA facility, they are accommodated in this case as well. An example scenario is an
individual who is seeking a check-up or a consultation while away from home. While this
scenario lacks urgency from a clinical perspective, an excessive delay in providing care
will result in a negative experience for the veteran.
Update electronic medical record
Once patient care has been provided to the traveling veteran, the electronic medical
record is updated. This is usually not an issue since the record has already been made
available for review at the visiting location prior to care being rendered.
Notification of primary care provider at home facility
In the current process, the notification to the veteran's primary care provider that care has
been provided to a traveling veteran is largely manual. In cases where consultation with
Page 51 of 94
the PCM was not necessary to render care, it is up to the care provider or his staff at the
visiting location to alert the PCM either via a flag in the medical record, a phone call or a
secure e-mail. This process step is often unsuccessful due to the workload at both the
visiting and home locations. This step is important nonetheless since the PCM is
responsible for managing the veteran's care.
Process Insights
Between the two primary processes within the traveling veteran enterprise, the temporary
care process presents more opportunities for improvement. Categorizing veterans within
the temporary care process and understanding the differences is the first step in better
tailoring process to serve each type.
7.2 Metrics and Costs (for strategic alternatives in performance improvements)
The most challenging aspect of assessing the current performance of the traveling veteran
enterprise was obtaining insight into metrics and associated costs. Efforts to identify
quantitative metrics were unsuccessful. While the VHA collects a myriad amount of data
concerning patient care, none of this information is being used on a recurring basis to
measure how well the enterprise is providing care specifically to traveling veterans.
Therefore the information collected concerning performance of the traveling veteran
enterprise is largely anecdotal. VISNs that experience a large influx of traveling veterans
on a seasonal basis are more aware of the magnitude of the enterprise via anecdotal
measures such as an increase in demand for services and resulting overloaded care
provider schedules. Additionally, another measure of current performance has been
feedback, sometimes in the form of complaints, by veterans who have sought care while
in a traveling status.
Since the boundaries of the traveling veteran enterprise largely exist only in abstract
across the entire VHA system, it is difficult to extract costs specifically tied to the
enterprise. The only personnel resources currently dedicated to this enterprise are the
referral case managers who also facilitate intra-VISN patient transfers. In interviews with
VHA personnel, areas where traveling veteran enterprise costs are incurred include:
Emergency room visits-Traveling veterans are sometimes directed to the
emergency department for care when outside their VISN. This is an expensive
resource to draw upon for routine events such as prescription refills.
* Care providers-While doctors and nurses provide care for traveling veterans,
they do so inefficiently due to issues with communication and medical history
review. A lack of continuity may also generate increased additional cost due to a
recurring need to familiarize a care provider with a patient's medical history.
* Redundant tests, procedures, prescription refills, and imaging services - Because
information in the medical record is order to hard to locate or understand, there is
e
Page 52 of 94
an excessive amount of redundant tasks occurring within the traveling patient
enterprise. These will be further described in the Enterprise Waste section.
What can be nearly unequivocally stated is that in the aggregate, the VHA is very
efficient from a cost perspective in comparison with other large medical endeavors.
According to the VA's Health Economics Resource Center (HERC), the VHA is much
more efficient than Medicare:
The most thorough study comparing the relative cost of VA provided care
was an HSR&D study that compared actual VA costs at six VA medical
centers to the hypothetical fee-for-service payments for the same services
that would have been paid by Medicare. The final report (Nugent, 2004)
found that VA was providing care at a lower cost. Details from this study
appeared as a series of papers in a special supplement of Medical Care in
2003. The overview paper for the papers in this supplement is cited below
(Nugent, 2003). The supplement includes papers with detailed
comparisons for difference services, including acute hospital stays,
outpatient care, nursing home, and other types of care.
Furthermore, according to the HERC, the VHA's pharmacy costs are also substantially
lower than those of Medicare as well as private pharmacy benefit programs:
It has been estimated that VA's Pharmacy Benefits Management (PBM)
program saved VA $1.5 billion between 1995 and 1999 (Sales, 2005). VA
prices for 20 medications commonly used by seniors are lower even than
those negotiated by private PBM companies for the Medicare Prescription
Drug Plan (Families USA, 2005).
7.3 X-Matrix
An X-Matrix was used to analyze the interdependencies between stakeholder values,
enterprise processes, enterprise strategic goals and enterprise metrics. Each of the four
quadrants of the matrix describes the interactions between two of the process dimensions.
Such interactions are classified as Strong (blue), Weak (yellow) and None (white). The
results, represented by the number of blues and yellows in each row and column, provide
high-level insight into the nature of interaction. Through the review of the matrix, it is
possible to identify the aspects of the enterprise worth improving in order to cover the
gaps.
7.3.1
X-Matrix Inputs
Page 53 of 94
Strategic objectives
As defined above, the strategic objectives of the Veterans Health Administration
Traveling Veteran Enterprise as follows:
e
e
e
Provide timely and appropriate care
Streamline eligibility verification
Efficiently allocate care provider resources
Metrics
Given the absence of well-defined performance measures within the traveling veteran
enterprise, what is presented in this section are the anecdotal measures discussed above:
e
e
e
Anecdotal evidence of increased demand for appointments
Anecdotal evidence of overloaded doctor schedules
Information about transfer process in national patient feedback
Key processes
The X-matrix combined the processes of permanent and temporary transfer together,
integrating each step when appropriate and specifying whether each step is part of the
temporary transfer process, the permanent transfer process or both. The resulting list is as
follows:
*
o
e
*
*
e
*
e
e
Identification and verification of eligibility (permanent and temporary transfer)
Transfer of electronic medical record (permanent)
Access electronic medical record (temporary)
Assignment of the veteran to a primary care provider (permanent)
Assignment of the veteran to a care provider (temporary)
Patient care (permanent and temporary)
Update and maintenance of electronic medical record (permanent)
Update the electronic medical record (temporary)
Notification of primary care provider at home facility (temporary)
Stakeholder values
We listed the values of all stakeholders, consolidating the ones that were very similar:
"
-
Continuity and consistency of care
Receive care
Ability to access information within the medical record
Effective communication
Ability to locate information within the medical record
Accurate information within medical record
Ability to communicate with the Veteran
Page 54 of 94
-
Ability to
Ability to
Ability to
Ability to
-
Timely verification of eligibility
*
*
Ability to communicate with consultant provider at receiving VA
Ability to contact and communicate with home primary care provider
Advanced notice of traveling veteran's arrival
Ability to place traveling veteran on a panel
7.3.2
place information in the medical record
provide tests, imaging services, etc., to traveling veterans
provide consults with a provider to traveling veterans
provide pharmacy services to traveling veterans
Analysisof the X-Matrix
The figure below represents the filled X-Matrix for the current state of the Veterans
Health Administration Traveling Veteran Enterprise.
~t "0
.f-I~f
I' W
2
2
' 11
g
2
3
3
3
3
2
1
1
1
3
2
2
3
2
0
2
0o
1
1
1
I
I
toaly arid
Provide
161
appo
ra e
1 11
Steamlie
egbiiidvveriton
Efficinyallale erarprovider
I N
AI -7
Strategic
Objectives
C~*1
Metrics
1 111
I
I-N
K.
l
~.
.=-
i
6
CrI
Stakeholder
Values
at
II
Key Processes
TWefarofMferWnCmredriairecord
'pemanarit)
Assignment
oftheveteran
toaprimary
ca
Prnieranenert)
Asaigimert
ofte veteran
to acare
~re
care(permanient
andtemporary)
Patient
Update
andmaintenance
ofeleeronic
mnedical
record
(penoarerd)
fthelectroric
medicatlecr
Update
fleoaori oprimary
careprovider
at
__homefaahity
8
3
2
~
5
2'-
2
45
3
'
3
3
1
Y7 5
0
Figure 23 Traveling Veteran Enterprise Current State X-Matrix
A review of the matrix reveals several high level issues within the enterprise. There are
no strong correlations between Metrics and Strategic Objectives and between Metrics and
Processes. This is due to the fact that the metrics are anecdotal and have not been
intentionally designed to provide insight into what is occurring within the enterprise and
have not been designed with the intent of providing insight into process performance, nor
of satisfying the objectives of the enterprise.
Page 55 of 94
Strategic Objectives vs. Metrics
1
2
0
Provide timely and appropriate care
0 0
Streamline eligibility verification
Efficiently allocate care provider
mresources
-
-
Strategic
Objectives
M~
0
CX
8
0
0
Metrics
Stakeholder
aes
e P5
rocsse
0.2
4) Z)
0~e)
--
0 MC0)
,
Key Processes
Figure 24 Objectives vs. Metrics Quadrant
The upper left quadrant represents how well the enterprises' metrics are aligned with the
strategic objectives. In other words, how much an improvement or decline of the metrics
can translate into a progress or regress in the path towards the obtainment of the goals. As
previously mentioned, there are no strong correlations. This indicates that any alignment
between objectives and metrics is weak. This is due to the lack of quantitative metrics. In
particular, overtasked physicians may be representative of an insufficient allocation of
care providers as well as delays in the care process. Improving this metric may improve
timeliness of care as well as resource efficiency. Patients may relate their experience in a
customer survey and express an opinion about the timeliness and appropriateness of the
care they received. However, the increase in the demand for appointments may not be
entirely due to loads imposed by traveling veterans. While providing a baseline of need
for care, this metric does not provide any link to the actual progress towards the
enterprise's goals.In addition, the goal of streamlining the eligibility verification process
is not connected with any of the metrics, therefore, any effort influencing the obtainment
of such goal through metrics improvement is likely to be fortuitous as opposed to
planned.In conclusion, the current metrics appear to be insufficient for driving progress
towards the objectives.
Page 56 of 94
Metrics vs. Key Processes
Strategic
Objectives
0
0
06
0
C
Metn cs
.0
00
fc
oo
6
Key Processes
UCUtII(..dlLI dtilOlVC[IIVi(dUfFUI OHeligUllIEY
0
(permanent and temporary transfer)
Transfer of electronic medical record
7
I
(permanent)
7
Access electronic medical
record(temporary)
Assignment of the veteran to a primary
care provider(permanent)
Assignment of the veteran to a care
provider(temporary)
I
7
I
7
r
2
Stakeholder
Values
pr
~6 F7 r 0
@~
Patient care (permanent and temporary)
Update and maintenance of electronic
medical record (permanent)
Update the electronic medical record
(temporary)
Notification of primary care provider at
home facility
71 0
Figure 25 Metrics vs. Key Processes Quadrant
The lower left quadrant depicts how much the metrics provide an indication of the
performance of the processes. Schedule overload and negative patient feedback are
potentially the result of process inefficiencies. For instance, a delay in any step of the
process may result in negative feedback from a patient. However, the reliability of
feedback as a comprehensive performance estimator is weak, i.e. not all inefficiencies or
successes will result in feedback.
Analogously, a heavy, non-standardized assignment and update process may result in
care provider schedule overload, but some inefficiencies will not be reflected in this
metric. Once again, the increase in the number of appointments, does not provide any
indication of the actual health of the process, as it addresses the conditions of operation
and not the efficiency and effectiveness of the process in dealing with such conditions.
Page 57 of 94
Key Processes vs. Stakeholder Values
8
3
2
5
4
2
2
5
3
3
3
1
7
5
0
2
Figure 26 Processes vs. Values Quadrant
The lower right quadrant provides an overview of how well the processes are satisfying
the stakeholders' values. It is evident that the processes that provide the most value, or
value to most of the stakeholders, are the ones pertaining to the update and retrieval of
patient information within the electronic medical record system. If those processes are
ineffective, not only patient transfer actions, but also care will be compromised.
Notifying the primary care provider at home facility also has an impact on most values,
albeit not always as strong. The identification and verification of eligibility of the patient
influences most values, because it is a pre-requisite for receiving care. However, the
eligibility verification process itself does not directly produce value for the primary
stakeholders, therefore the links are weak in most cases.
Page 58 of 94
Stakeholder Values vs. Strategic Objectives
o
0 V-0 , 0
1
~1
Providetimel and
1
2
1'2
3
3
3
3
3
3
3
3
'0#
o"o
1
1
1
1'1
2
2
-8
O r'0
1
3
3
0
2
2
3
3
2
2
16
ate care
6
eligibility
verification
Streamline
Efficiently
afocate careprovider
reoes
2
2
,
7
n
1-
Figure 27 Values vs. Objectives Quadrant
The upper right quadrant illustrates the alignment of stakeholder values to the strategic
objectives of the enterprise. For the traveling veteran enterprise, these are well aligned.
There is strong alignment between stakeholder values and providing quality care to
traveling veterans. Resource allocation is also in line with most stakeholder values. The
values also point towards a streamlining of the eligibility process.
7.3.3 X-Matrix Conclusions
As demonstrated above, the X-matrix provides a visual understanding of alignment
between the current enterprise processes, metrics, values and objectives. Within the
current state, there is good alignment between stakeholder values and objectives as well
as between processes and values. The primary weak point is metrics which are anecdotal
and weakly aligned with the processes and objectives. This result confirmed our initial
intuition based on interviews with VHA personnel and lays the foundation for
improvement.
7.4 CLIOS Process
7.4.1 Stage 1: Representation
In the current VA case, there are structure and behavior related characteristics within the
system. The existing structure system contains natures of system, subsystems and
connections between sussystems of Physical Domain (Hospitals and Clinics) and
groups(various stakeholders) on the institutional sphere.
Describe System: Issue Checklist and Goal Identification
Page 59 of 94
VHA carris two missions: provide high quality health care to a growing number of
American veterans, facing time of war, and rising health care costs as well as economic
crisis and political turmoil.
In the face of these challenges, the actions the VHA has taken to ensure realization of its
strategic vision center around 6 objectives: Quality, Access, Satisfaction, Function,
Community health, Cost-effectiveness.
Traveling Veteran Enterprise Vision:
* Take care of travelingveterans
* Provide timely and appropriatecare
" Streamline eligibility verification
* Efficiently allocate care providerresources
While the objectives and core values described above at the VHA level apply to traveling
veterans, the vision of the enterprise appropriately focuses on taking care of veterans
while also recognizing that resources must be efficiently utilized. When a veteran seeks
care at a facility in another VISN away from home, there are a number of issues that may
arise.
In summary, the strategic vision of the enterprise is well matched with the challenges it
encounters while serving traveling veterans. Those challenges are:
* Barriers to timely care
o Eligibility verification delays
o Timely assignment of a care provider
e
Appropriate level of care
o Continuity of care for conditions requiring multiple visits
* Efficient allocation of resources
o Matching care required to appropriate level of care provider
Identify Major Subsystems of Physical Domain and Major Actor Groups on the
Institutional Sphere
Considering VA system, the physical domain invovles healthcare physical VISN location
and facilities. Based on Chapter 3 definition, in VA system, CLIOS system boundry is
entire healthcare services for Veterans. The institutional sphere referes to the Veterans
Health Administration (VHA), a federal government entity within the Department of
Veterans' Affairs and one of the largest healthcare providing networks operating in the
United States. The physical domain is the 23 Veteran Integrated Service Networks
(VISNs). Veterans typically receive care at a facility within the VISN where their
primary residence is located. However in instances when veterans are away from their
primary home location, they are entitled to receive care within the VISN where they are
located. Each VISN is individual subsystem, considering 23 subsystems in institional
sphere. The major actor groups are referral case managers, doctors, registered nurses and
vetrans.
Page 60 of 94
Populate the Physical Domain and the Institutional Sphere on the CLIOS Diagram
Entire Veterans
Health Services
Veterans Health
Administration
(VHA)
Primary
23 Veterans
Integrated
Service
Networks
(VISNs)
/
Care
Providers
Figure 28 VA CLIOS Diagram
Like Figure 28, CLIOS diagram in VA has reflected relationships within subsystems with
physical domain as well as institional sphere.
Describe Components on the Physical Domain and Organizations on the Institutional
Sphere
Health care provided by the VHA is nearly comprehensive. The Department of Veterans
Affairs characterizes the care it provides as that required to promote good health,
preserve current health and restore better health. The majority of care is dispensed via
153 medical centers and over 800 community based outpatient clinics (CBOCs). VHA
Medical Centers offer a wide range of services including traditional hospital-based
services such as surgery, critical care, mental health, orthopedics, pharmacy, radiology
and physical therapy as well as additional medical and surgical specialty services
including audiology & speech pathology, dermatology, dental, geriatrics, neurology,
oncology, podiatry, prosthetics, urology, and vision care. Some medical centers also offer
advanced services such as organ transplants and plastic surgery. CBOCs provide veterans
with additional access to care and provide the most common outpatient services,
including health and wellness visits. The VHA continues to expand the number of
CBOCs especially in rural areas.
Page 61 of 94
Veteran care is most often coordinated via a primary care provider model to ensure
continuity of care. Veterans are assigned to a primary care provider's panel at their home
facility.
There are multiple components on subsystems. Mainly, these are Primary care providers
(PCPs), including physicians, physician assistants and nurse practitioners. All PCPs
provide both care and determine when to refer veterans to other providers for specialty
care.
Describe Links Among Components and Organizations
Since this is healthcare service center for ventrans, links connecting components and each
different care groups are the process based on patients' needs. Generally for veterans
within VISN, patients' primary cares are links among compents such as bone surgery,
links are blood inquiry, medicine, surgery preparation and facility to connect doctors,
nurses, therapists groups.
There are two primary processes within the Veterans Health Administration Traveling
Veteran Enterprise. The key criteria for which process a traveling veteran follows is
whether the veteran's travel to a new location is permanent (A) or temporary (B). As each
process identifies and verifies eligibility, transfer medical records, assigns veterans to a
Primary Care Provider, links will need to connect to other subsystem's patient care, and
updates the veteran's medical records.
Seek Insights about System Behavior
Veterans travel outside their primary VISN's coverage for extended timeframes for a
multitude of reasons. Some veterans are "snowbirds" and migrate to warmer climates for
the winter months. Others travel and remain with friends or family members for extended
times. Still others travel extensively as part of their jobs (for example, truck drivers)
while some veterans are homeless and travel from place to place on a frequent basis.
Traveling veterans from within each of these categories often require care ranging from
emergency services to routine prescription refills and blood tests.
7.4.2 Stage 2: Design, Evaluation and Selection
Identify Performance Measures, Refine System Goals, and Build Quantitative Model
Current travling vetran enterprise does not have clear metrics and associated costs. After
multiple attempts of interviews, visits and documents review, it was unsuccessful to
identify quantitative metrics. Despite xa large amount of data relating with patient care,
none of this information can be used on a recurring basis to measure how well the
enterprise is providing care specifically to traveling veterans. Therefore the information
collected concerning performance of the traveling veteran enterprise is largely anecdotal.
Page 62 of 94
This becomes one of challenges in the project. VISNs fully understand of current
enterprise via anecdotal measures such as an increase in demand for services and
resulting overloaded care provider schedules. Another measure of current performance
has been feedback through filling out the forms. Most times these forms become the form
of complaints, by veterans who have sought care while in a traveling status.
Obviously, travling veteran enterprise largely across the entire VHA system. It is difficult
to extract costs specifically tied to the enterprise. By now, the dedicated resource in this
enterprise is limited. Referral Case Managers are the only personnel resources, who
facilitate intra-VISN patient transfers.
Based on interviews with VHA personel, costs related areas in traveling veteran
enterprise are following:
Cost factors
Emergency room visits
CurrentStage
Traveling veterans are
sometimes directed to the
emergency department for
care when outside their
Expense level
Expense resource
Especially for routine
events such as prescription
refills.
VISN.
Care providers
While doctors and nurses
provide care for traveling
veterans, they do so
inefficiently due to issues
with communication and
medical history review.
Redundant tests,
procedures, prescription
refills, and imaging services
Because information in the
medical record is order to
hard to locate or
understand, there is an
excessive amount of
Varied due to inefficiency.
A lack of continuity may
also generate increased
additional cost due to a
recurring need to
familiarize a care provider
with a patient's medical
history.
Considered as "Enterprise
Waste"
redundant tasks occurring
within the traveling patient
enterprise.
Pharmacy cost
Though cost is low, the
process takes longer for
traveling vetrans as most of
time clinic need to verify
status and contact another
Lower than those of
and
private
medicare
pharmacy benefit programs.
VISON.
System goals align with enterprise vision, to provide proper medical service for traveling
vetrans. Without accurate measurement and costs, it is difficult to evaluate enterprise.
Due to complex nature, seveal attempts for creating quatitative model do not work
Page 63 of 94
through all 23 VISNs due to each VISN's unique situation. The better target is to better
utilize its information technology system.
Identify and Design Strategic Alternatives for Performance Improvements
One of alternatives consideration is to create a central information system across all VA
facilities. It is better utilize existing Information technology system, connecting data
sources with each VISN.
Currently, the VA has one of the most advanced information systems to share electronic
medical records. Providers can easily access patient medical records within their own
VISN. However, when a patient travels to another VISN, providers must access the
veteran's record through a system called "VistA web", which draws information from the
patient's record in their home VISN. The provider then inputs information based on the
patient's visit into VistA web, which then does not get placed in the patient's record in
their home VISN. Therefore, the patient's providers in their home VISN are forced to go
into the VistA web system to receive notes and information from the visit (which often
does not take place). Therefore, this consideration focuses on creating a "reflective"
central information system to leverage across all VISNs.
Flag Important Areas of Uncertainty
Through our surveys and visits with various stakeholders within the VHA, it became
clear there is a lack of process standardization associated with delivering care to veterans
traveling within different VISNs. This lack of standardization of processes makes it
difficult to effectively use metrics to assess the performance of their patient transfer
network. This fosters a cycle alternating between a lack of information that yields
inefficient and disjointed processes and the results of those processes, which fail to
provide adequate feedback necessary to create meaningful process improvements.
A lack of standardization across all processes between VISNs
* A lack of education for veterans, care providers, and other VHA staff
* A need for effective communication across the traveling veteran enterprise
" A need for clearer roles and responsibilities for staff dealing with traveling
veterans
e
A need for increased knowledge-sharing with regard to best practices and areas of
improvement across the organization
e
Evaluate Strategic Alternatives and Select Robust Bundles that Perform "Best" Across
Uncertainties
In order to better utilize existing information technology system, it is necessary to have
performance tracking metrics after metrics and processes are implemented.
For the traveling veteran enterprise, it would not make sense to implement a performance
measurement system before future state processes are put into operation. Once that has
been accomplished, metrics can be developed and applied. In order to develop a set of
Page 64 of 94
metrics for the VA, our team examined the stakeholder survey to identify issues in the
traveling veteran processes. Solutions were then identified for each of the issues and
metrics were developed for the proposed solutions. The targets for the proposed metrics
are taken as one year after metrics and processes are implemented. One of the first
priority goals of the metrics will be to identify a list of facilities with a high density of
traveling patients. In addition, these metrics will be used to demonstrate the efficiency
and effectiveness of the new processes traveling patient enterprise. From there,
management can identify areas of improvement and potential areas for cost savings to
drive business value. One quick win for the transformation section would be to quantify
specific non-valued added processes with the current enteprises (i.e. redundant test
orders) and show how our plan help reduce these costs. Even though most of our future
state processes requires funding, if we are able to cut down on these non-value added
wastes, the resources required to launch this plan will be justified. In general, these
efforts will help further integrate the enterprise to drive business value to meet
stakeholder needs in the long term.
7.4.3 Stage 3: Implementation
0
10. Design Strategy
for Implementation in the
Physical Domain and Implement
11. Design Strategy
for implementation in the
Institutional Sphere and
Implement
12. Post-huplementation Evaluation
and Modification
Design Strategy for Implementation in the Physical Domain and Implement
Physical Domain contains entire 23 VISNs, directly handling traveling veterans visits
cross VISNs. Since they come in as temporary care while traveling, comparing with their
primary care visits in their home location. When a veteran's travel culminates in a
temporary transfer to a new location, the process includes the following steps:
*
Identification and verification of eligibility
Access electronic medical record
e
Assignment of the veteran to a care provider
* Patient care
e
Update electronic medical record
e
Notification of primary care provider at home facility
e
Page 65 of 94
To efficient identify and verify veterans eligility, it is the corresponding process step
when a permanent transfer process scenario occurs. One difference is that there may be
more communication between the facilities in different facilities to ensure an effective
hand-off of the veteran. This is done by either the referral case manager or social
workers enlisted to help by the referral case managers.
Information within an electronic medical record created in one VISN is read-only within
other VISNs. A local record within the visting VISN must be created in order to add
information to the veteran's electronic medical history. An issue with this process is the
formatting and placement of the information within the electronic record. Placement is
not consistent across facilities and regions. Another issue is access to information that
resides outside the VHA electronic medical record. This information may be in the
form of records held by a outside health care provider/facility or background information
within the home location's primary care provider's personal memory. Extemal
communication methods such as encrypted e-mail and faxes are often utilized to provide
this information to the care provider who is supporting the veteran in the temporary
location. Often, it is the referral case manager that facilitates this transfer of information.
Patient care is where the veteran receives the medical care that he or she requires. Care
provided to travelers who are seeking temporary care while away from their home
facilities can be categorized into four scenarios as shown in the repeated chart below.
Scenario
ExmpePer
Specific, Tme-Limited,
Simple Needs
INR, Medication
centage of cases
30
Care / Services
-Consult
- Lab Order
- Appointment
Specific, Time-Limited,
Comolex..Cannot Wait
Cancer-care, Follow-up
to Aortic Aneurysm
40
- Appointment
- Back & Forth
Consultations w/ RCMs
Specific, NotTimeLimited. Complex,-Cannot
wait
Diabetes, Congestive
Heart Failurei COPD
20
-Record review
-Dual enrollment
- Managed care
General, Not TimeLimited, Not Comglex
Routine annual exams,
consults
10
- Record review
- Consultations
- Appointment
Care Scenarios
Design Strategy for Implementation inthe Institutional Sphere and Implement
The institional sphere is entire VHA, the administration handling veterans affairs.
Besides handling information system as main implmentation focus, policy, process and
organization are also very important. The information systems highlights that the
VistA/CPRS system will be visible and alterable across all VISNs. Therefore, the VistA
Page 66 of 94
Remote view functionality web system will no longer be needed. The Office of the Chief
Information Officer for the VA will drive this transformation effort and develop the
national level strategy. Policies and processes will be developed to help drive inputting
information into the medical record in a standard format, including using similar
terminology across all VISNs and inputing the right information in the right place (a
frequent compliant of providers within the current information system because it is very
difficult to find information in the record with traveling veterans because providers often
put it into different locations across the VISNs). Also patients will be empowered to
notify their home VISN that they will be traveling through the "My Healthy Vet" online
portal. This system, which already exists today, could be further linked with this
reflective central information system and patients can then book their appointment while
they are traveling through this system.
Post-implementation Evaluation and Modification
Importance of this implementation:
" Central Information System will allow easy access for all providers and staff
across the system
" Relevant stakeholders will see the same record and not just information pulled
from the home record into VistA
* Standard processes for inputting information into the record will prevent "waste"
because providers won't have to search around the record for information and
redundant tests will not be ordered because they will know where to find this
information in the current record.
Difficulty of this implementation
Creation of a centralized information system is a very expensive process and will
require significant time and resources to develop and transition into operation
It is necessary to do post-evaluation in one year and two years timeline after all policies
and processes are implmentation. There are concems on system redesign conflict,
considering to moving the entire electronic health record system into a single "cloudbased" information system. This should be discussed further with various stakeholders
regarding to the timeline and cost.
Page 67 of 94
7.5 Enterprise Architecture Framework (8 Views)
Based on VA case, here are the analysis on 8 views with stakeholder interactions, key
view relationship with other views, strength/weakness and threat/opportunities.
During the case study, VA enterprise represents a typical enterprise organization what
challenges they need to face. Figure 15 presents how 8 views collaborate supporting VA
operation. Considering strategy as input of Veterans Health Administration, VA have
policies and processes parallel supporting each other. Information System is the
"blackbox" containing all the information of traveling veteran enterprise in order to
support and generate services for the customer, which also take the feedback as
knowledge based to feed in information system. The entire transformation is under
organization's view, handling internal and external changes.
Figure 29 Travelling Veteran Enterprise in VA Case Stuly
7.5.1
Strategy
Strategy is to create strategic goals, vision and direction of the enterprise including the
business model, enterprise metrics and objectives. Strategy helps enterprise to understand
how the current enterprise strives to care for traveling veterans.
Currently the strategy is to provide care using existing resources with the addition of a
Referral Case Manager at each facility acting as "point of contact for assisting veterans and
medical center staff in scheduling appointments, transferring non-electronic records,
arranging provider-to-provider contact, if necessary, and generally facilitating the care needs
of traveling veterans seeking care at non-preferred VA medical centers." This strategy was
Page 68 of 94
articulated at the national level in the form of the 2007 VHA Directive 2007-016
Coordinated Care Policy for Traveling Veterans. The directive also serves as the primary
nexus between the strategy, policy and process views. While making clear that traveling
veterans receive care, it also includes stipulates policies and processes for VISN and
medical center leadership to respectively adhere to and carry out.
Stakeholder Interactions
Strategy is one of critical view in VA case. It provides leadership to coordinate and align
long-term plan across VISNs. VA's RCMs own the travelling veteran process. Strategy is
to have VA act as "provider" to provide services to the travelling patients.
Key View Relationship with Other Views
Strategy - Information Technology
Electronic medical record infrastructure
Strategy -- Policy
*
Dictates the link between processes and IT
Strategy -- Organization
0 Determines which stakeholders are involved
Strategy -- Processes
Strategy focuses the processes surrounding PRS/VistA system
Strength/Weakness
- Strategic planning group in place with in VHA
- Huge need within the enterprise to develop strategies to improve the travelling
veteran enterprise
- Large, bureaucratic government organization can delay implementation of
strategies
Threat/Opportunities
- Increasing veteran population making it difficult to provide high level care
without large increases in cost
- Increasing health care costs
Traveling veteran dissatisfaction
7.5.2
Process
Process is to present Core leadership, lifecycle and enabling processes by which the
enterprise creates value for its stakeholders.
Current Veterans Affairs organization has provided good stewardship among various
programs. Its process for traveling veterans has provided healthcare products and services
for all eligible veterans, able to transfer patients' information across VISNs. In current
process, there are processes in place for healthcare providers and employees to access
transfer and temporary patient data, trying to enhance communication.
Page 69 of 94
Among the relationships with other views, Veterans Affairs utilizes CPRS/Vista for its
information exchange. CPRS/Vista are closely tied with process and need to evolve
together through each step. VA's strategy directly determines which stakeholders are
involved. The first step of VA process is to verify patient eligibility.
I
Update or
Patient Recod
Figure 30 VA Case Current State Process
Current processes provide accurate steps for transferring patient medical cross visions
and exchange electronic medical record internally. But it is not standardized process,
despite of having all the data. With increasing veteran population and health care costs,
we see the needs to improve the processes starting with standardization in place and
provide high-rated satisfaction from traveling veterans.
7.5.3 Organization
Organization refers to the organizational structure of the enterprise as well as
relationships, culture, behaviors and boundaries between individuals, teams and
organizations.
The Veterans Health Administration (VHA) is a federal government entity within the
Department of Veterans' Affairs and is one of the largest healthcare providing networks
operating in the United States. The administration operates over 1,400 sites nationwide
providing treatment to over 5 million veterans. Approximately 240,000 people are
Page 70 of 94
employed by the VHA which has an annual budget of $3.1 billion. With Geographical 23
Veteran Integrated Service Networks (VISNs). Veterans typically receive care at a
facility within the VISN where their primary residence is located. However in instances
when veterans are away their primary home location, they are entitled to receive care
within the VISN where they are located.
Veterans travel outside their primary VISN's coverage for extended timeframes for a
multitude of reasons. Some veterans are "snowbirds" and migrate to warmer climates for
the winter months. Traveling veterans from within each of these categories often require
care ranging from emergency services to routine prescription refills and blood tests.
The organization stressed the need to "maximize continuity and consistent, appropriate,
and safe care for traveling veterans". It heavily depends on existing process and
information technology to process travel patients data and provide healthcare.
While the objectives and core values at the VHA level apply to traveling veterans, the
vision of the enterprise appropriately focuses on taking care of veterans while also
recognizing that resources must be efficiently utilized. When a veteran seeks care at a
facility in another VISN away from home, there are a number of issues that may arise.
VHA directive 2007-016 established guidelines for coordinating care of traveling
veterans and articulated the following issues in doing so:
"Currently, traveling patients who seek routine care and arrive at distant
facilitieswithout priornotice may face barriersto timely care. If not registeredin
the facility's Veterans Integrated System Technology Architecture (VistA), these
veterans must first register at the medical center's eligibility office, or at other
sites performing this function. Prior to obtaining temporary supplies of routine
medications, traveling veterans are evaluated by providers at non-preferred
facilities who write prescriptions anew, a cumbersome process that may take
hours to days to complete. Similarly, traveling veterans seeking routine blood
tests need to register at the distantfacility and be evaluatedby a provider.
Accommodating unanticipatedmedical needs of traveling patients also stresses
individual facilities. While clinicians may view and enter orders on the
Computerized Patient Record System (CPRS) at the same facility where an
individual patient has registered, read-only limitations of the VHA-wide
informatics system prohibit cliniciansfrom making electronic orders that will be
recognized at distant VHA facilities. As a result, clinicians spend valuable time
reviewing patients' records in order to provide temporary supplies of routine
medication. Similarly, clinicians at the preferred site cannot easily monitor
routine blood work for their travelingpatients; providers at non-preferred sites
must evaluate the patients anew and order the tests. "
Page 71 of 94
7.5.4
Knowledge
Knowledge refers the implicit and tacit knowledge, capabilities, and intellectual property
resident in the enterprise. From VA VistA/CPRS System, "All information and
knowledge needed to perform the enterprise business operations and the relationships
among that information. Comment on areas of disconnect across the views and
opportunities for improvement."
Capturing and sharing knowledge is an important aspect of fostering continual
improvement in any enterprise. Within an enterprise there are many sources of
knowledge, and the method for best capturing and sharing this knowledge varies with
each stakeholder group. For instance, the type of knowledge relevant to helping doctors
improve patient care is different from that needed to help RCMs coordinate care across
VISNs. A doctor might look to external professional organizations or publications for
new insights while one RCM might look to another for insights.
For the travelling veterans enterprise, there were two recurring themes that appeared in
the survey results obtained from staff:
1) a lack of knowledge-sharing or best practice forum
2) a lack of standardization.
The first theme represents a shared frustration among different stakeholders that their
ideas for improvement were going unheeded with regards to the VistA/CPRS systems
and processes for handling veterans travelling across VISNs. The second theme
represents the confusion and frustration that results from essentially having 23 different
systems (with different processes) with which to coordinate.
These complaints suggest a system that is not learning, and their broader effects can be
understood by mapping them onto a framework developed by Nonaka, et al. (SeeFigure
31 and Figure 32). This framework represents the process that transforms knowledge at
the individual level to knowledge at the organizational level. The process is summarized
as follows: first, individuals share their tacit knowledge with other individuals; second,
groups of individuals then articulate this tacit knowledge into explicit knowledge (e.g.
procedural manual); third, this new expression of explicit knowledge is disseminated to a
broader audience; and, finally, this explicit information is internalized back into tacit
information by individuals through 'leaming by doing' creating a new platform for the
next round of the process (Nonaka, et al. 2000).
Figure 31 represents the first theme from the survey - the lack of a forum for sharing best
practices. Individuals at the local level may socialized ideas amongst themselves, but the
lack of a forum prevents them from ever converting these ideas into a clearly articulated
document. Without this, there can be no disseminating of the knowledge to a larger
audience, and the local ideas will unlikely be adopted elsewhere. This problem is
magnified because individuals at the local level will always be frustrated by the same
problem preventing them from turning their attention to secondary and tertiary problems.
Page 72 of 94
*
Tacit
Tacit
Soci
*IL
Internalizing
Disseminating
Explicit
Explicit
Figure 31 Nonaka, et al. framework for lack of best practices forum
Figure 32 represents the second theme from the survey - the lack of standardization
across VISNs. In this case, individuals at the local level may be able to convert their tacit
knowledge and express it in an explicit form, but there are barriers that prevent the
broader dissemination of this knowledge. (This could be the result of structural
misalignment in the organization. i.e. a group may be able to articulate their ideas, but it
is another group's job to set policy, and they happen to disagree.) The same problem
results as in the first example.
Tacit
Tacit
.a
Soci
culating
[-
Inten
-L
,
2
Ec
FxplIicit
init
Figure 32 Nonaka, et al. framework for lack of standardization
Page 73 of 94
7.5.5
Information Technology
Information Technology is to contain Information needs of the enterprise, including flows
of information as well as the systems and technologies needed to ensure information
availability.
Stakeholder Interactions
Information Technology is IT "owners" to oversee CPRS/VistA system. Since RCMs
own the travelling veteran process and input information into VistA and CPRS. As
providers, Information Technology provides services to the travelling patient and input
information into VistA and CPRS
Key View Relationship with Other Views
Information technology -- Policy
-
CPRS/VistA is governed and standardized by policy. HIPAA regulations control
security issues with the IT system.
Information Technology - Processes
CPRS/Vista are closely tied with process and need to evolve together
Information Technology -Knowledge
Patient information captured with CPRS/VistA
Strength/Weakness
- Reduces medical errors
- Accessible across all VISNs, but requires a request to access record
- Information placement in the record and terminology is not standardized across
VISNs
- Although accessible, requires a secure link which sometimes drives users to send
information over email (needs to be secure or violates HIPAA)
Threat/Opportunities
e VA is respected externally for their information technology
e New information technologies surrounding EMRs are continually being
developed
* Standard practices and guidelines (ex: meaningful use) are being defined due to
government incentives
* Government debt is growing resulting in less $ from government
7.5.6 Policy/ExternalEnvironment
Policy/External Environment is the environment with the external regulatory, political
and societal environments in which the enterprise operates.
The travelling veterans enterprise is housed in the larger Veterans Administration. The
very existence of this larger organization is the result of an external policy - specifically a
congressional mandate. This external policy, or mandate, sets requirements that the VA
Page 74 of 94
must meet, but the VA is largely left to set its own internal policy about how to best meet
these requirements. From time to time these external requirements are refined or changed
causing the VA to alter its internal policy in order to meet these new requirements.
As a broad example, the VA's congressional mandate requires it to provide health care to
all veterans and qualified members of their family. This led the VA to set an internal
policy establishing a branch within itself known as the Veteran's Health Administration
(VHA). The VHA then set an internal policy dividing the country geographically into 23
VISNs in order to best allocate resources. This division was not directly the result of an
external policy, but the decision was certainly affected by such.
This particular policy decision created other policy problems. For instance, the external
policy simply states that veterans and qualified family members are entitled to health
care. The implication, though, is that they are entitled to this regardless of where they are
in the country. Now, most veterans typically receive care at a facility within the VISN
where their primary residence is located. However, in instances where veterans are
travelling away from their primary home location, they are entitled to receive care within
the VISN in which they are located. So, even though the VHA has decided to allocate
resources by region it still must be flexible enough to handle cases where veterans are
travelling across VISNs.
This tension between external and internal polices led the VHA to set another internal
policy in order to "maximize continuity and consistent, appropriate, and safe care for
traveling veterans" (Department of Veterans Affairs, 2007). The primary function of this
directive was to set guidelines, or best practices, for personnel handling these types of
situations. The policy touched on all aspects of care. For instance, one pharmacist from
VISN 18 described the following best practice for receiving medications:
"As far as pharmacy goes, a traveling veteran policy was created where approved clinical
pharmacists can provide up to a 2 week supply of home medications if a patient needs a
bridge while visiting and will be returning home within that time frame. We also have
points of contact set up for triage and providers if pharmacy is unable to complete the
request by the patient." (Department of Veterans Affairs, 2007)
However, this aspect of the policy has not been deployed effectively across all VISNs. Of
all temporary traveling veteran cases, requests for pharmaceuticals typically make up
about 30% of all cases although they can make up a much larger percentage in areas that
experience significant seasonal migrations such as Florida and Arizona.
This highlights an important aspect of the VHA. Its large size creates the potential to take
best practices developed locally and implement them on a large scale through
organization-wide policy. However, the large size of the organization can also be selfdefeating in that it becomes more and more difficult to enforce compliance to these
policies. Each of the various sub-groups has unique characteristics, and non-compliance
can result from misaligned organizational structure a lack of sufficient knowledge for
Page 75 of 94
implementation. This is why it is very important to consider this view in relation to the
organization, knowledge, and process views.
7.5.7 Product & Services
Product includes Product(s) developed by the enterprise; key platforms; modular vs.
integral architectures, etc. Services include Services(s) delivered and or supplied by the
enterprise, including in support of products. In VA case, product and services are bundled
together based on its healthcare characteristics.
e
e
*
e
e
e
*
*
e
*
e
e
Enterprise provides healthcare to traveling veterans
Main purpose of the enterprise-care for veterans
In the form of products (medicine, medical equipment, treatments etc)
In the form of services (diagnoses, physical therapy, etc)
Enterprise provides information, scheduling and tools to physicians and other care
providers (nurses, PTs, etc)
Medical information in the form of electronic medical records and lab results
Scheduling in the form of care panels and appointments
Tools are provided to care providers (operating rooms, machines, etc)
Enterprise provides value to tax payers
Provides cost-effective way to care for veterans who have served society
Serves as a good steward of tax payer funds
Ensures only those eligible for services receive them
Enterprise provides value to Referral Case Managers
Ability to communicate and coordinate care across VISNs
Key Relationships for Product & Services with other views:
Products/Services and Information
e
Electronic medical record and IT infrastructure are critical to providing good
products and services
* Accurate and available veteran medical information
Metrics-allows analysis of patient movements to better allocate resources
s
Products/Services and Policy
- Policy determines how medical products and services are provided by the
enterprise
- Optimize resource allocation through policies (traveling care panel, super doc,
etc)
- Provides structure to minimize wasted time (standardize records, etc)
Products/Services and Organization
- Organization determines how products and services are provided
Currently organized around home location (primary care provider)
e
Page 76 of 94
* Organization could be tailored to better serve traveling veterans (Traveling Patient
Window, TCPs, super docs)
Page 77 of 94
7.6 Final Implementation
The first dimension involves actions categorized for each of the three primary levels:
national, VISN level and facility level. The second dimension is defined by time and is
also broken into three categories: immediate, near-to mid-term and long term.
National Level Transformation
At the national level, transformation will begin immediately with the development of
national policies that will be promulgated to the VISN and local levels. In order to
facilitate the creation of these policies, a traveling patient council should be established.
This council will have ownership and be empowered to author policies for subsequent
implementation. Implementation of the four national policy recommendations discussed
in the "To Be" section will be put into motion. Data collection will be initiated in order to
classify VISNs and facilities as high traveling or low traveling veteran locations.
Additional Guidance on RCM qualifications and training will be developed.
Development of training plans and policies to be promulgated across the VHA will begin
and a directive enforcing the "scrubbing" of patient databases on a quarterly basis will be
issued.
In the near- to mid-term, selected facilities will be directed to begin pilot programs in
order to validate the utility of predictive traveling veteran metrics and verify the efficacy
of the implementation tools developed during the previous semester's effort (TPW, TCP,
"super doc", etc). A national community of practice will be established to capture and
exchange information concerning what was effective and what wasn't. It is expected that
the majority of participants will be RCMs but care providers and IT professionals are
expected to participate as well.
In the long term, managers at the national level will monitor and enforce policy directives
across the VHA. Process and metric effectiveness will be reviewed in accordance with
continuous improvement principles and changes such as tool updating will be made as
necessary in an evolutionary manner.
VISN and Local Level Transformation
In the immediate timeframe, VISN and local leadership will support data collection in
order to categorize high and low traveling veteran facilities. Leadership will also be
expected to support the establishment of the national level traveling patient council as
well as provide input into the development of the national policy directives. Best
practices already in place will be provided to the council so that they may be examined
for potential implementation across the system within the initial set of pilot programs.
VISN and local leadership will be earnest in their support of near- to mid-term pilot
programs and strive to ensure good data is obtained on what works and what does not.
Data collection will continue conceming traveling patient flows in order to identify
deeper trends and prepare for the next iteration. RCMs will join the community of
practice and will begin training of facility staff on how to provide care to traveling
veterans within their own local context.
Page 78 of 94
Over the long term, VISN and local level managers and RCMs will continue to monitor
the efficacy of traveling veteran processes and make changes as appropriate in a
continuous improvement manner. Information on changes in demographics and patient
flows will be up channeled via the CoP and the traveling patient council.
Page 79 of 94
Conclusion
This chapter is a summary and reflection on the enterprise framework evaluation between
EA and CLIOS, and insights gained throughout the VA case study. Clearly there are
some steps from EA and CLIOS that can be combined, while some cannot. Based on
theoretical analysis and case study, it seems likely that CLIOS and EA could be
effectively merged. However, because this strategy has not been proven, and because the
two methods draw from experience in different industries, there is some uncertainty in
this approach. In the EA strategic planning stage and CLIOS planning & transformation
stage, we see similar steps that can be harmonized. Also, we see that the different
approaches the two frameworks adopt can be mutually beneficial. CLIOS specifically
provides a step to design the physical domain, which could help EA implement its
framework in physical architecture, such as green architecture design and urban planning,
transportation systems and energy related area. Merging with EA, CLIOS framework
could take advantage of detailed transformation roadmap, LESAT and strategic focus in
enterprise development.
There are a few areas where a merged hybrid methodology is less likely to be successful.
CLIOS has been applied successfully in transportation systems. The EA framework, as
well as transformation roadmap and LESAT methods, have been presented as a whole
package for comprehensive enterprise development. There are unique characteristics in
each framework. By considering the strengths of the individual processes, a merged
methodology will provide an optimal outcome while reducing the chance of generating
wastes across the enterprise.
Page 80 of 94
Appendices
Appendix A: Stakeholder Group Survey Questions
1. What is your current role within the VA organization?
2. What VISN do you currently work in?
3. What are the main tasks you perform with regard to providing or facilitating care for
traveling veterans across VISNs?
Care Provider - Doctor
e
Care Provider - Nurse
* Care Provider - Nurse Practitioner
e
Care Provider - Physician's Assistant
* Referral Case Manager
" PCMM Coordinator
* Eligibility Clerk
e
VISN-level employee
e
Other (please specify)
4. Please rank the following aspects in providing or facilitating care to traveling veterans
across VISNs? (1 = not that important to you, 5 = critical part of your job)
e
Effective communication
e
Advanced notice of traveling veteran's arrival
-
Ability to access information within the medical record
e
Ability to locate information within the medical record
e
Ability to place information in the medical record
e
Accurate information within medical record
e
Ability to contact and communicate with home primary care provider
e
Ability to provide pharmacy services to traveling veterans
-
Ability to provide consults with a provider to traveling veterans
Page 81 of 94
e
Ability to provide tests, imaging services, etc., to traveling veterans
e
Ability to place traveling veteran on a panel
* Timely verification of eligibility
e
Ability to communicate with consultant provider at receiving VA.
" Ability to communicate with the Veteran
e
Other (please specify)
5. When handling traveling veterans across VISNs, please rank how effective the VA
currently is in the following aspects (1 = not effective, 5 = very effective).
* Effective communication
* Advanced notice of traveling veteran's arrival
e
Ability to access information within the medical record
* Ability to locate information within the medical record
* Ability to place information in the medical record
* Accurate information within medical record
* Ability to contact and communicate with home primary care provider
" Ability to provide pharmacy services to traveling veterans
* Ability to provide consults with a provider to traveling veterans
e
Ability to provide tests, imaging services, etc., to traveling veterans
* Ability to place traveling veteran on a panel
* Timely verification of eligibility
e
Ability to communicate with consultant provider at receiving VA.
* Ability to communicate with the Veteran
* Other (please specify)
6. Please answer the following questions:
(Disagree / Somewhat Disagree / Neutral / Slightly Agree / Agree / N/A)
I understand the processes taking place within other VISNs
Page 82 of 94
e
I understand who I need to contact in the other VISNs when I need to transfer a
patient across VISNs
" VISNs collaborate effectively when dealing with transferring patients across
VISNs
" I have the opportunity to meet and discuss best practices with members of other
VISNs
7. What personnel within the VA organization do you interact with when dealing with
traveling veterans across VISNs?
(Note: Don't list out specific names of people. Please list out their role within the VA
organization).
8. Are there any aspects of providing care to traveling veterans that you find wasteful?
(i.e. extra paperwork, redundant steps, delays, communication, etc)
9. What could the VA organization provide you that you would make your job easier
when dealing with traveling veterans across VISNs?
10. Has your facility found a way to make the process of facilitating traveling veterans
across VISNS easier?
11. Do you have any other feedback for us regarding transferring traveling veterans
across VISNs?
Page 83 of 94
Appendix B: Tailored LESAT Tables
Process
Enterprise Practice
Enterprise Characteristic
Section I - Lean Transformation/Leadership
I.A. Enterprise
I.A. 1 - Integration of process Lean impacts growth, profitability
Strategic Planning improvement in strategic
and market penetration
planning process
I.A.2 - Focus on customer
The enterprise value stream is
value
patient-centered
I.A.3 - Leveraging the extended Value stream extends throughout the
enterprise
extended enterprise, providing
continuity of care
I.B.1 - Leaming and education
in Lean for enterprise leaders
I.B.2 - Senior management
commitment
I.B.3 - Lean enterprise vision
I.B.4 - A sense of urgency
I.C. Focus on the 1.C.1 - Understanding current
Value Stream
value stream
I.C.2 - Enterprise flow
I.B. Adopt
Enterprise_
Paradigm
"Unlearning" the old, learning the
ew
enior management leading it
ersonally
New mental model of the enterprise
The primary driving force for Lean
How we now deliver value to
customers
"Single piece flow" of materials and
information
I.C.3 - Designing future value Value stream to meet the enterprise
stream
vision
I.C.4 - Performance Measures Performance measures drive
enterprise behavior
I.D. Develop
Enterprise
Structure and
I.D.1 - Enterprise
Organize to support value delivery
organizational orientation
I.D.2 - Relationships based on "Win-win" vs. "we-they"
Behavior
mutual trust
I.E. Create &
Refine
I.D.3 - Open and timely
communications
I.D.4 - Employee
empowerment
I.D.5 - Incentive alignment
I.D.6 - Innovation
encouragement
nformation flows freely to support
nformed decision making
Multi-disciplinary teams share
responsibility
Reward the behavior you want
From placing blame to creative
problem solving
I.D.7 - Lean change agents
The inspiration and drivers of change
I.E. 1 - Enterprise-level Lean
transformation plan
Charting the course across the
extended enterprise
Page 84 of 94
Process
Transformation
Plan
Enterprise Practice
I.E.2 - Commit resources for
Enterprise Characteristic
Resource provision for lean
ean improvements
.E.3 - Provide education and
Just-in-time learning
training
I.F. Implement
Enterprise
.F.2 - Tracking detailed
implementation
Assessing actual outcomes against
goals
1.G. 1 - Structured continuous
Uniformity in how we get better
Improvement
Initiatives
I.G. Focus on
ontinuous
Improvement
improvement processes
I.G.2 - Monitoring lean
progress
I.G.3 - Nurturing the process
I.G.4 - Capturing lessons
learned
Assessing progress toward achieving
enterprise objectives
Assure executive level involvement
Ensuring that successes lead to more
successes
TTL Link
Lean Practice
II.A. Business
II.A. 1 Leverage Lean capability for Exploiting new business
Lean Characteristic
cquisition and business growth
opportunities arising from lean
Program
Management
enabled capabilities
II.A.2 Optimize the capability and
Lean enables business growth
utilization of assets
through the redeployment of
assets
II.A.3 Provide capability to manage Success follows effective risk
risk, cost, schedule and performance management
II.A.4 Allocate resources for
Teaming for success
program development efforts
II.B.
I.B. 1 Establish a requirements
Stakeholder pull vs.
Requirements
efinition process to optimize
technology/product push
efinition
lifecycle value
Page 85 of 94
II.B.2 Utilize data from the extended Closed loop processes are in place
II.C. Develop
roduct and
Process
enterprise to optimize future
to capture operational
requirement definitions
performance data
II.C.1 Incorporate customer value
Understanding customer value
into design of products and
allows continuous improvement
processes
of product and process
II.C.2 Incorporate downstream
Understanding downstream
stakeholder values into products and stakeholders allows value to flow
seanlessly to customer
processes
I.C.3 Integrate product and process Breaking down of functional silos
enables seamless communication
development
and value flow
II.D. Manage
II.D. 1 Define and develop supplier
Core competencies aligned across
Supply Chain
network
supplier network
II.D.2 Optimize network-wide
Partnering with key suppliers and
performance
optimizing processes to
II.D.3 Foster Innovation and
Incentivizing innovation &
knowledge sharing throughout the
technology transfer
supplier network
II.E. Produce
II.E.1 Utilize production knowledge Strategic leveraging of
Product
and capabilities
manufacturing capability
II.E.2 Establish and maintain a lean Defect free production pulled by
II.F. Distribute
d Service
Product
production system
the customer
I.F. 1 Align sales and marketing to
Matching demand and capabilities
production
II.F.2 Distribute product in a lean
Right product, right quantity at
fashion
the right time
II.F.3 Enhance value of delivered
products and services to customers
and the enterprise
Page 86 of 94
esponding to the voice of the
customer
II.F.4 Provide post-delivery service, Providing customer solutions
support, and sustainability
III.A. Lean
II.A.1. Financial system
Lean requires appropriate
Organizational
supports lean transformation
inancial data
Enablers
III.A.2. Enterprise stakeholders Data on demand
pull required financial
information
III.A.3. Promulgate the learning Learning organizations create a
organization
flexible workforce
III.A.4. Enable the lean
Facilitate the flow of information
enterprise with information
and knowledge
systems and tools
II.A.5. Integration of
"Cleaner, healthier, safer"
environmental protection, heath
and safety into the business
III.B. Lean Process
II.B.l. Process standardization
Strive for consistency and re-use
Enablers
II.B.2. Common tools and
Assuring compatibility, reducing
systems
:osts
III.B.3. Variation reduction
Reduce uncertainty by reducing
variation
Notes:
Reinstituted performance measures to see if stakeholders recognize that there is a lack of
metrics.
Removed IF1, as traveling patient enterprise has not instituted any lean transformation
plans.
Removed IG2, IG3, IG5 as enterprise leaders have not instituted lean, or attempted to.
Page 87 of 94
Appendix C: Stakeholder Categories within the Traveling Patient Enterprise
End User
*
Patients (Veterans, Families)
Suppliers
e
Providers (Physician, Nurse, Nurse Practitioner, Physician Assistants)
*
Primary Care Managers (PCM)
*
Referral Case Managers (RCM)
*
Eligibility Clerk (EC)
*
Pharmacists
*
VISN-levels employees
e
VISN Leadership
*
VHA Leadership
*
VA Leadership
e
Tax payers, unions
Leadership
External stakeholders
Page 88 of 94
Appendix D: Roles & Responsibilities of Stakeholders within the Traveling
Patient Enterprise
Physician
Nurse
*
Medical care for acute and chronic problems
*
Primary care
*
Refill and renew prescriptions
*
Reviewing records
*
Follow-up care
*
Emergency room care
*
Eye exams
*
Dental care
e
Providing in-patient nursing care
*
Communicate with other facilities and arrange travel as needed
*
Coordinate care
*
Consult Management
*
Providing names and addresses of other VA facilities
*
Assist with transitioning care from diagnosis locally to treatment at tertiary care
facility
*
Follow-up care
*
Assist with medication renewals
*
Continue to monitor vet at receiving site
*
Education of Veterans to tell them how they need to communicate with home VA
prior to traveling
*
Providing in-patient nursing care
*
Enter in orders
*
Communicate with other facilities and arrange travel as needed
*
Review remote data and document in CPRS
*
Provide telehealth services
*
Phone triage
Page 89 of 94
RCM
*
Coordinate the sending of notes and films
*
Obtaining appointments
*
Setup travel and lodging
*
Arranging consults
*
Care coordination
*
Contacting eligibility clerks to load patient into the system
*
Review remote notes
*
Confer with RCM at the other facility
*
Contact the patient for any clarification/info needed
*
Initiate orders through the screening clinic provider for labwork, consults,
equipment, etc.
PCM
*
Facilitate scheduling appointments
*
Send requests to Chief PCP to review patients for dual enrollment, if appropriate
*
Coordinate with specialty services
e
Assigning veterans to their primary care providers and looking for duplicate
assignments at facilities
*
Patient transfer coordinator
*
PCP assignments
*
Ensuring provider is approving dual care based on medical need, then assign or
leave unassigned based on provider's desire
EC
*
Determines Eligibility of veterans and their families to receive care
*
Communicates with Referral Case Manager regarding Eligibility
Page 90 of 94
Appendix E: Value Elicitations
Effective communication
Advanced notice of traveling veteran's
arrival
13/11
Ability to access information within the
medical record
1/4
10/11
6/13
10/11
4/2
1/2
1/2
3/5
3/4
1/2
5/1
6/8
4/2
1/5
3/2
1/2
10/5
11/11
10/11
Ability to provide pharmacy services tc
traveling veterans
7/1
6/8
11/8
6/11
Ability to provide consults
provider to traveling veterans
9/11
1/4
6/7
7/8
6/4
6/7
13/13
11/8
6/7
Timely verification of eligibility
12/7
Ability to communicate with consultant
provider at receiving VA.
9/7
7/4
6/11
1/1
12/8
3/4
10/11
Ability to communicate with the Veteran S/5
3/2
6/1
k/6
Ability to locate information within the
medical record
1/7
Ability to place information in the
medical record
3/1
Accurate information within medica
record
4/5
Ability to contact and communicate with
home primary care provider
11/13
with
10/11
Ability to provide tests, imaging services,
etc., to traveling veterans
7/1
Ability to place traveling veteran on a
panel
13/13
*Note: Each Value was ranked from 1-13, where 1 is the top priority, 13 is the least
priority. Green-shaded boxes were the values identified as areas where the enterprise is
performing well, while yellow-shaded boxes are values in which the current system is not
delivering
Page 91 of 94
Reference
Amano, Y.D. (2004), "Measuring Congestion and Emissions: a Metwork Model for
Mexico City", Thesis, Cambridge, MA, MIT
Blackburn, C.D. (2009), "Metrics for Enterprise Transformation", Thesis, Cambridge,
MA, MIT
Department of Veterans Affairs. (2007, May 9). VHA Directive 2007-016 Coordinated
Care Policy for Traveling Veterans.
Dodder, Rebecca, et al. "The Concept of the "CLIOS Process": Intergrating the Study of
Physical and Institutional Systems Using Mexico City as an Example." Unpublished
Manuscript. January 26,2005.
Dunn, T.P. (2010), "The Geography of Strategy: An Exploration of Alternative
Frameworks
for Transportation
Infrastructure
Strategy
Development",
Thesis,
Cambridge, MA, MIT
Montoya, M.J., (2010), "On Developing Business Architectures: A Multi-Framework
Evaluation of an Early-Stage Enterprise", Thesis, Cambridge, MA, MIT
Moses, Joel. "Foundational Issues in Engineering Systems" A Framing Paper"
Engineering Systems Monograph, Engineering Systems Symposium, March 2004. May
14, 2004. http://esd.mit.edu/symposium/pdfs/monograph/framing.pdf.
Nightingale, D.J.,(2009), "Principles of Enterprise Systems", MIT Second International
Symposium on Engineering Systems, Cambridge, MA
Nightingale, D.J., (2010). "Intergrating the Lean Enterprise", Course Material,
Cambridge, MA: Massachusetts Institute of Technology, Fall.
Page 92 of 94
Nightingale, D.J., and Mize, J.H. (2002). "Development of a Lean Enterprise
Transformation Maturity
Model", International Knowledge Systems Management
Journal.
Nightingale, D.J., and Rhodes, D., (2011). " Enterprise Architecting", Course Material,
Cambreidge, MA: Massachusetts Institute of Technology, Spring.
Nightingale, D.J. and Rhodes, D., (2011). "Fundamental Concepts for Architecting",
Enterprising Architecting, Course Material, Cambridge, MA: Massachusetts Institute of
Technology, Spring.
Nightingale,
D.J. and
Architecting",
Rhodes, D.,
Enterprising
(2011).
Architecting,
"Holistic Thinking
Course
Material,
for Enterprise
Cambridge,
MA:
Massachusetts Institute of Technology, Spring.
Nightingale, D.J., Stanke, A.K., and Bryan, T., (2008). Enterprise Strategic Analysis for
Transformation Guide. Cambridge, MA: Lean Advancement Initiative, MIT.
Sussman, Joseph. Introduction to Transportation Systems. Boston: Artech House, 2000.
Sussman, Joseph. Perspective on Intelligent Transportation Systems (ITS). New York:
Springer, 2005
Sussman, J., Dodder, R., McConnell, J., Mostashari, A., Sgouridis, S., The CLIOS
Process User Guide, Feburary 2009
Sussman, J., Sgouridis, S., and Ward, J. (2005). A New Approach to Transportation
Planning for the
2 1 "s Century:
Regional Strategic Transportation Planning as a CLIOS.
Transportation Research Record, No. 1931, pp. 8 9 - 9 8 .
Page 93 of 94
Omwenga, B.G. (2009), "A Technology Strategy Analysis for the Deployment of
Broadband Connectivity for Economic Development in Emerging Economies: Studying
the Case of Keya Using the CLIOS Process", Thesis, Cambridge, MA, MIT.
Wang, C., Marticello, D., Kamin, C., Ippolito, A., Smith, A., and Gentiletti, A,
Integrating Lean Enterprise(2010) and Enterprise Architecting(201 1) Team Reports,
Cambridge, MA, MIT.
Ward, J (2004), "Toll Road Public-Private Partnerships in Malaysia: Using the CLIOS
Process for Policy Improvements", Thesis, Cambridge, MA, MIT.
Zakaria, Z (2004), "Framework for designing regional planning architecture for APTSenabled regional multimodal public transportation system", Thesis, Cambridge, MA,
MIT.
Page 94 of 94