SERVICE SETTINGS FOR AN AGING SOCIETY: ©
advertisement

SERVICE SETTINGS FOR AN AGING SOCIETY:
A Community Ordering Principle
by
Gaius Grant Nelson
Bachelor of Architecture
University of Minnesota
1981
SUBMITTED TO THE DEPARTMENT OF ARCHITECTURE
IN PARTIAL FULFILLMENT OF THE REQUIREMENTS OF THE
DEGREE
MASTER OF SCIENCE IN ARCHITECTURE STUDIES AT THE
MASSACHUSETS INSTITUTE OF TECHNOLOGY
SEPTEMBER 1987
© Gaius Grant Nelson 1987
The author hereby grants to M.I.T.
permission to reproduce and to distribute publicly copies
of this thesis document in whole or in part
Signature of the author
daius Grant Nelson
Department of Architecture
June 16, 1987
Certified by
Sandra C. Howell
Associate Professor of
Behavioral Science in Architecture
Thesis Advisor
Accepted by
Julian Beinart
\j
Chairman
Department Commitee for Graduate Students
MASSACHUSETTS INSTITUTE
OF TECHNOLOGY
SEP 2 3' bl
LIBRAP3ES
EsC~
SERVICE SETTINGS FOR AN AGING SOCIETY:
A Community Ordering Principle
by
Gaius Grant Nelson
Submitted to the Department of Architecture on June 16, 1987
in partial fulfillment of the requirements for the degree
Master of Science in Architecture Studies.
Abstract
Current facility models used in the design of housing and service settings for
older people encourage the development of urban, large scale, age-segregated
or not,
unwittingly,
either
has
Research
environments.
institutional
need for
by
stressing the
these models
and perpetuated
encouraged
Such research has
congruence between person and dwelling environment.
encouraged the movement of individuals to alternative living environments
when age related changes in social, economic or health status reduce this level
of congruence between person and environment based on key factors which
are deemed important by gerontological researchers.
This is a
Homeownership by older people is a behavior which is increasing.
Approximately 75% of all
trend which is not likely to reverse in the future.
people over the age of 65 choose to remain in their own owned single-family
residential settings. It is estimated that by the year 1995 over 80% of all older
people will live in their own homes, yet research of alternative models for
The key to
service delivery to support these actions is sorely lacking.
providing services to an increasing number of older people in our society will
What is
not be through the production of alternative housing situations.
needed is the provision of service settings which assist these people in the
maintenance of their lives within their chosen and preferred living situation.
The research undertaken in this paper will investigate the development of
alternative neighborhood based service settings designed to meet this growing
The proposed model will integrate these service settings into residential
need.
A case study will
areas using the neighborhood as an urban design framework.
examine the usefulness of the neighborhood concept in the planning and
delivery of services to older populations within a suburban community.
Thesis
Title:
Advisor:
Sandra C. Howell
Associate Professor of
Behavioral Science in
Architecture
2
Acknowledgements
I would like to thank Sandra Howell, my thesis
advisor, for her patience and understanding
through the times when I knew what I wanted to
say, but was unable to put it down on paper.
Thank you to our friends who made our stay at
M.I.T. all the .more worthwhile.
Special
thanks
to
Janet
Gardner
for
friendship and help when it was needed.
her
Most of all many thanks to my wonderful wife
Wendy Weeks, without her support I may never
have accomplished all the things that needed to
be done during my stay here.
Acknowledgements
Acknowledgements
3
3
Table
of
Contents
3
Acknowledgments
4
Table
6
Introduction
6
An
of Contents
Aging
Society
The Need for Long-Term Care Services
The Aging of the Suburbs
Implication for the Future
1 3
for
Environments
Aging
The Continuum of Care
Institutional Settings
Multi-Level Facilities
Service Enriched Housing
The Blurring of the Boundaries
Continuing Care Retirement Centers
2 2
The
Neighborhood
27
Case Study
2 7
The
Community
of
Definition
Use
3 7
Neighborhoods
Neighborhood
Where
Older
Residential
4 1
Concept
Service
People
Live
Integration
Needs
of Older
People
Institutional Care
Non-Institutional Care
Informal Care
Formal Community Based Care
Contents
of Contents
Table of
Table
4
4
51
Existing
Services
in
Arlington
Age-segregated Housing
Meal Programs
Transportation Services
Home Care Services
Visiting Nurses Association
Adult Day Heath Care
Long-Term Care Facilities
59
Segmentation
in
Segmentation
in
Service
Delivery
Planning
LTCSA Planning Area
Home Care Catchment Area
Characteristics of Service Settings
Institutional vs. Community Care
73
The Model
73
A Neighborhood
Service
Setting
The Nursing Home A Consolidated Service Setting
Size of Facility
Relationship
to The
82
Conclusion
84
Bibliography
of Contents
Table of
Contents
Table
Neighborhood
5
5
1
Introduction
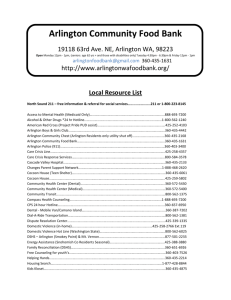
The older population has inc reased far more
rapidly than the rest of th e population for
In the last two decades
most of this century.
alone, the 65-plus population grew by more
the
under-65
percent
while
than
54
24 percent.
population increased by
on ly
Since 1960, an average of 1 49,000 persons a
month have joined the ranks of the elderly
(Soldo and Manton 1984).
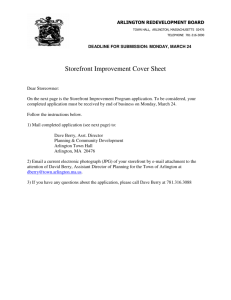
An Aging Society
There
is
no
doubt
that
the
population
United States is growing older.
dramatic
increases
too 120-
80
There have been
in the numbers
POPULATION 55 YEARS AND
OVER
of the
of people
BY AGE: 1900-2050
55-64
65-74
{ ~]85+
75-84
POPULATION
IN
MILLIONS
40
i 00
1920
1W4
1960
1960
2000
2020
2040
S05E U.S. Bureau of the Census,CurrentPopulation Reports.Series P-25. No. 952
U.S. Censusof the Population. 1090-1960
Introduction
Introduction
6
6
over the age of 65, both in terms of real
numbers and as a percentage of the total
At the beginning of the century
population.
less than 1 in 25 Americans was over the age of
65. In 1985 this had increased to over 1 in 9,
making a total of 28.5 million individuals 65
years of age or older. It is projected that these
trends will continue well into the next century.
By 2010, due to the maturation of the
baby-boom, this proportion will increase to 1 in
7. By the year 2050 nearly 1 in 5 Americans are
expected to be over the age of 65.
The population of older Americans is not only
larger than in the past, it is also growing older.
The fastest growing portion of the older
population is made up of those individuals over
the age of 75. This group, the so called old-old, is
expected to equal nearly 50% of all elderly
individuals by the year 2000 (Special Commitee
It is
on Aging, United States Senate, 1986).
precisely this group of old-old Americans which
will require localized health and social services
on a long-term and continual basis.
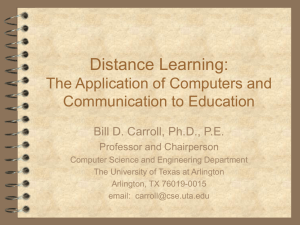
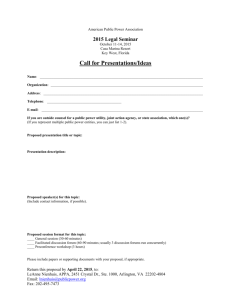
The Need for Long-Term Care Services
In announcing the formation of a new task
force on long term care policies, Dr. Otis R.
Bowen, Health and Human Services Secretary,
quoted National Center for Health Statistics
estimates that the nursing home population in
the United States will more than double within
Introduction
Introduction
7
7
NURSING HOME POPULATION PROJECTIONS
PERSONS 65 YEARS AND OLDER BY AGE GROUP
1980-2040
5.
4.6
4.
POPULATION .
IN
MILLIONS 2.
.
2.9
.9 2. 2
1.
1..
1.
0
1980
1985
1990
1995
2000
2020
2040
YEAR
*65-74
U
75-84
E] 85 AND OVER
SOURCE: Manton and Soldo, "Dynamics of Health Changes in the
New Perspectives and Evidence," Milbank
Oldest old:
Memorial Fond Quarterly, Vol. 63, No. 2, Spring 1985
and unpublished tabulations from the author
Other
the next generation (Eastman 1987).
estimates indicate that there will be a 47%
increase in the nursing home population by the
year 2000 and another 100% percent increase
by the year 2040. If these projections are
actualized there will be a need to add over
500,000 new nursing home beds to the nations
current stock of 1,400,000 beds within the next
and another 2.2 million beds
fifteen years
between the years 2000 and 2040 (Manton and
Soldo 1985).
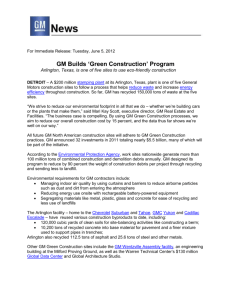
At any given time, approximately 5% of all older
people are likely to be in a nursing home
(National Center for Health Statistics, 1977
But care
National Nursing Home Survey).
within a nursing home is not the only service
required by older people. A 1982 National Long
Term Care Survey estimated that for every
Introduction
Introduction
8
8
18
OLDER AMERICANS IN NEED OF LONG-TERM CARE
1980 -2040
14-
PERSONS
(IN MILLIONS)
LIVING IN COMMUNITY
2
IN NURSING HOMES
0ooo
200
2040
YEAR
SOURCE: Manton and Soldo, "Dynamics of Health Changes in the
Oldest Old: New Perspectives and Evidence," Milbank
Memorial Fund Quarterly, Vol. 63, No. 2, Spring 1985
and unpublished tabulations from the author
person age 65 years or older residing within an
institutional setting there are nearly four times
that many living within the community and in
need of some form of long-term care approximately 4.6 million persons or 19% of the
total population of older people (Special
Committee on Aging, United States Senate 1986).
The service needs of this population, though
often non-medical in nature are nonetheless
critical to the maintenance of an independent
way of living and the avoidance of unnecessary
institutionalization.
The
Aging
of the Suburbs
In 1980, for the first time in history, there were
more people over the age of 65 living in the
suburbs (a total of 10.1 million people) than in
Suburbs,
central cities (8.1 million people).
most often perceived as areas consisting mainly
of young families with children, have changed
The elderly
drastically in the last decades.
Introduction
9
9
population
within
community
the
in
a
United
the
potential
implications
social
of
carrying
for the provision
services
now
States
averages
This aging of the suburbs
11.8% (Logan 1984).
has
suburban
typical
to
an
with
of
vast
it
health
older
and
population
increasingly in need of a wide array of services.
Implications
Long-term
for
care
concentrated
the
Future
service
on
the
provision
has
construction
stock
of
nursing
far
of facilities
designed specifically for this task.
current
thus
Much of the
facilities
was
constructed in the early 1960's and 1970's when
there
was
large
an
incredible
variety
of
push
housing
construct
to
and
institutional
settings for the elderly (Koncelik 1976).
with
an
often
aging
built
research
population,
without
new
adequate
into the long-term
knowledge,
design
was
a
as
were
knowledge
or
of older
Due to this lack of
hospital-based
chosen
Faced
facilities
care needs
people (Kayser-Jones 1986).
a
model
the
of
means
facility
for service
delivery to old people requiring long-term care.
Since
that
time,
environmental
the psychological
these
settings
1972,
Koncelik
created
an
traditional,
and
on
sociological
users
1976).
increased
medical
has
These
of
(Snyder
studies
recognition
model
into
impacts
occured
that
associated
long-term care is not sufficient in
Introduction
Introduction
research
have
the
with
and of itself
10
10
as a response to the growing needs of older
The creation of
people in this country.
residential settings for long-term care now
receives much greater attention due to the
realization that an individual is a resident a
majority of the time and a patient for only a
small fraction of the time.
of
creation
for
the
Suggestions
non-institutional care settings range from the
encouragement of social interaction amoung
residents and with the greater community
(Pastalan 1986), to the design of "open nursing
homes" which are meant to return control over
the environment to residents and offer as many
ways out of the setting as there are into it
But these modifications and
(Koncelik 1976).
of
refinements to the existing models
almost
deal
settings
service-enriched
exclusively with the the details of the
environment. These studies encourage the
creation of age-segregated, health care settings
microcosms
self-contained
separated from the greater community without
addressing the overall needs of an aging
designed
as
population.
Long-term care service settings must not be
viewed in isolation. It is time to step back and
determine whether settings being created using
current models of service provision are truely
being planned to meet the demands of the
Introduction
11
11
future.
to
Demands of a population which wishes
continue
living
neighborhoods
in
even
their
own
homes
and
as their need for services
increases.
There is little doubt that an expansion in the
development
of
long-term
care
services
and
settings will occur in the coming decades.
the
question
designed
as
to
for this
into alternative
the
purpose
nature
of
remains.
But,
settings
Research
frameworks for the planning of
long-term care settings is sorely lacking.
is
the
time
neighborhood
integral part of
to
investigate
the
based
service
settings
urban
Now
use
of
as
an
design.
Service settings of this type should be looked at
as a form
design
aging
and
of infra-structure
organization
of
investment
communities
into
for
the
an
society.
Introduction
Introduction
12
12
Environments
The
current
design
based
of
approach
the
environment
health
to
concept
and
between
Aging
environments
on
person
for
the
for
older
is
one
of congruence
in
individuals
status
and
the
which
the
social,
environments
congruence
environment
placed
in
providing
ideal
economic
in
which
available to
rank
low
order
levels
from
of care
those which provide high levels of care.
example,
independent
housing,
for older
people, is meant to provide
barrier-free,
environment
interaction
for
a
is
thought
to
there
services
provided
other extreme
are
that
few
"low
For
a secure,
social
beginning
to
Such housing
levels
or no
within the
to
especially
promotes
of aging.
provide
meaning
built
population
experience the effects
or
Using this model
range of housing options
is
is
between
An
they live are at a high level.
individuals
and
people
environment.
an
the full
planning
of
staff
and
facility.
are settings designed
care,"
few
At the
specifically
for the provision of health care services such as
a
skilled
nursing
providing
"high
including
all
activities
and
A Continuum
facility,
levels
meals,
or
nursing
of care"
assistance
24-hour nursing
to
home,
residents
with
daily
care.
of Care
The design of different types of environments is
based on the provision of a given level of care
Introduction
13
13
to the individuals residing within the setting. It
is believed that when a greater number of
optional levels of care are made available to
members of the community, the more likely the
match between
person
and
environment
becomes.
Within some community settings the
choice of housing options for old people may be
"Lower"*
"Higher"
-Lower levels of care refer to the common
instance where fewer staff and fewer services are available
CONTINUUM OF CARE:
TYPICAL PATTERNS OF MOVEMENT WHEN ALL LEVELS OF CARE ARE AVAILABLE
-Servlces**
High
1
Moderately
High
Type of Institution
Acute Care Hospital
Rehabilitation Hospital
Hospice
Skilled Nursing Facility (also: SNF.
Convalescent Home, Rest Home)
Moderate
Intermediate Care (also: Nursing
Home. Rest Home. ICF)
ModerateLow
Homes for the Aged (also: Adult
Homes; Personal Care Homes)
Congregate Care Apartments
Apartments for Disabled
Brief Description
Diagnosis. Medical Supervision,
Surgery (see above + Therapy
Emphasis)
Care for Terminally Ill Cancer
Patient
Registered Nurse 24 hours/day:
about 2.5 hrs/patient day of nursing
care: all meals: housekeeping;
activities
Licensed Practical Nurse (requirements vary) supervises; about 1.5
hours/patient day of nursing care
Meals; housekeeping: personal
assistance. may be a nursing staff
available (not generally required)
Apartment residences with central
meals available or accessible; may
be emergency or coordinating staff
available
Like Congregate Care Apartments;
typically more architecturally
accessible
Very
Low
Group Homes
Shared Housing/Small Group
Cooperative Housing/Self-help
housing
Smaller residences for adults and/or
children; emphasis on minimal staff
intervention in adult residences
Clusters of 8-30 older people in
residential style community-based
housing: tasks may be shared by
occupants and/or supplemented by
community agencies.
Apartment residences, typically age
and often income prerequisites: may
include government rent support for
some or all apartments: may be no
Specially Built Apartments (also:
Right: Table and Diagram
Apartments for Elderly: High Rise for
Elderly: Garden Apartments; Retiredeveloped by Lorraine Hiatt
ment Housing)
meal service
presenting the full range of
Note: The overwhelming majority (70%) of all older people reside in homes which they own. NOT in options ideally available to the institutions. apartments or shared living arrangements. There are exceptions to the amount or
degree of care in inqividual cases. Multi-level care or retirement campuses typically offer two or
elderly.
Source: Progressive more of these types of facilities.
~Nuber andvar"iy of services
Architecture, August 1981.
Introduction
14
14
very limited.
On the other hand, if a community
contains a full range of optional settings, from
those providing a very low level of services to
is
others providing high levels, the community
considered to possess a Continuum of Care for
older people.
Settings
Institutional
The concept of levels of care is loosely defined
in
care
health
an
of
institutionalization
case
In the
there
however,
facilities,
of
varieties
many
available.
settings
residential
the
to
relationship
been
has
The
concept.
the
of
design of facilities and the description of people
is
patients)
care
such
within
living
directly
involving
costs
the
with
of
regulations
care
"leveled"
of
facilities
according to
tools and cared for only
assessment
standardized
intensity
reimbursement
long-term
"patients" be
that
as
Federal
and
licensure
associated
require
and
State
provided.
to the
related
to
(referred
settings
within facilities licensed to provide the level of
care
determined
regulations
long-term
the
as
provided.
Though
into
patients,
referred to by the level of
well as, facilities are
care
Often,
necessary.
the
care
vary
facilities
following
Introduction
Introduction
are
catagories
Commonwealth
Department of Public
from
of
state
typically
to
state,
divided
(excerpted
from
Massachusetts,
Health Regulations
1984):
is
15
Levels I and II - Skilled nursing facilities
provide
of care
available
outside of an acute hospital
setting.
Services
include
continuous
nursing
addition
to
for
the
highest
levels
(SNF),
skilled
restorative
patients
and
who
improvement
or
therapeutic
show
to
a
or who
have a deteriorating
requiring
skilled
care.
provide
routine
availability
of
restorative
and
patients
point
that
services,
nursing
therapeutic
whose
condition
they
need
condition
facilities
nursing
skilled
for
stabilized
condition
care
only
(ICF),
periodic
services,
services.
has
in
services
potential
restoration
Level III -Intermediate
care
.
for
to
the
.
stabilized
supportive
and
nursing
care.
Level IV - Personal
the Aged,
residents
care facilities or Homes for
provide protective
who
do
not
or other medically
routinely
Facilities
One
associated
physical
settings
requirements
relocating
of
As
a
aspects
response
of
Introduction
Introduction
with
according
residents
individuals
(or improvements)
require
nursing
related services.
Multi-Level
problem
. . for
supervision.
in their
to
these
relocation
to the
is
with
the
the
design
health
necessity
subsequent
health
care
of
declines
status.
potentially
trauma,
of
negative
multi-level
16
16
facilities, that
is,
care
long-term
facilities
which provide two or more levels of care within
one
increasingly
become
have
facilitity
Such facilities are beneficial because
popular.
they minimize the effects of relocation by only
requiring a move from one part of the facility
to
rather than
another,
within
a
move,
simply
lower)
levels
facility
to
have
setting to
which
they
and
not
required
next
higher
accustomed
become
one
In this way, people may
another (Fisher 1978).
remain
from
are
the
because
are
of care
to
(or
where
not provided
they are.
Service
Housing
Enriched
As the population has aged the need for services
provided
within
has greatly
acute
visible
within age-segregated
needs
service
of
these
people
older
have been
models
additional housing
to
response
In
settings.
changing
settings
This need is especially
increased.
and highly
housing
housing
independent
developed
which include varying levels of services.
The
of
development
known
settings,
as
service-rich
moderately
"congregate
housing"
intended to provide an intermediate
of care,
continuum
and
housing
intermediate
people
activities
health
of some
and personal
Introduction
Introduction
care
level to the
that of independent
facilities.
This
level was designed for those older
need
in
between
was
assistance
with
daily
care but, who are not in
17
17
of
need
people
24-hour
in
services
nursing
need
into
of
By
moving
additional
support
care.
these
congregate
housing
which
is
designed especially to accomodate such needs a
match
between
setting
and
need
can
be
maintained.
This conceptual
model
of an intermediate
level
of service rich housing has not been completely
realized.
In reality there has been virtually no
movement
from
housing.
independent
Services
meals program
are
to
typically
providing
one
congregate
limited
meal
a
to
day,
a
five
days a week and some form of emergency access
Admissions
system.
settings
limit
substantially
rules
admission
to
to
those
independent and
for themselves
without
congregate
most
who
capable
outside
are
of caring
assistance.
Still, there has been a marked increase in the
number
of
services
independent
those
and
being
brought
congregate
housing
residents
who
have
aged
setting
and
now
require
current
into
both
sites
within
for
their
a
greater
housing
projects
range of services.
A
longitudinal
(Lawton
1980)
additional
that
services
is termed
In
five
study
and
of
a
settings
were
two
subsequent
study
(Lawton
1985),
progressively
an "accomodating
contrast
Introduction
to
the
added
model"
"constant
in
of
an
found
what
of housing.
model"
which
18
attempts
the
to maintain
population
the
original
through
transfers
settings, the "accomodating
the increased
infusion
character
laundry
care;
meals;
and
of services to residents
assistance
shopping;
and
other
model" has allowed
as their service needs increased.
of on-site
to
of
The provision
with
housework,
personal
transportation
and
health
programs,
have
reached the point where as one administrator of
a
large
housing
development
stated,
"in
practice, we now provide all but skilled nursing
care in our facility."
The
Blurring
The
continual
housing
of
the
accomodation
settings has
boundaries
settings.
between
There
definitions
continuum
Boundaries
no
caused
care
within
a blurring
of the
housing
longer
between
of
of services
and
care
to be
clear
within
the
appear
levels
except
health
in
the
institutional
models of care.
The advent of community based
Home Care
Personal
older
and
people
to
remain
Care
within
services
varied
allows
housing
settings, thus avoiding the need for institutional
care
much
longer.
independent
and
developments,
as
community
based
In
large
part,
however,
congregate
well
services,
as
have
the
housing
associated
been
targeted
only towards low and moderate income elderly.
Introduction
19
19
Continuing Care Retirement Communities
The lack of alternative settings providing home
and health care services within residential
environments for moderate and higher income
elderly populations is now being approached
through the development of Continuing Care
Retirement Communities (CCRC).
provide
This
lifetime residence to older people.
includes the provision of an
normally
independent living unit, a variety of in-home
services, as well as long-term health care, often
provided by an on-site skilled nursing facility.
Many such communities also include a wide
array of social and recreational spaces such as a
restaurant, swimming pool, library, game rooms
and lounges. Additional facilities may include a
grocery store, bank, beauty/barber shop, and
newsstand, making the CCRC a microcosm of the
These
communities
are
designed
to
larger community, with most of the services
needed for its residents' daily living provided
on-site. (Winklevoss 1984).
This provision of a full continuum within one
In
setting is not limited to new developments.
increasing numbers, housing projects for
independent living are providing additional
services to residents and in many cases either
constructing adjoining long-term care facilities
or forming contractual arrangements with
nearby nursing homes for the utilization of
Introduction
20
20
nursing beds for their residents.
From the
other direction existing nursing homes are
developing independent housing units in order
to "build-in" a market for health care services.
With all services and facilities provided within a
single development, the entire continuum of
care has been totally consolidated under a
single roof.
Introduction
21
21
The
Neighborhood
Concept
The idea of the neighborhood
community
organization
is
a unit of
a
commonly
accepted notion.
Though there are no clear
definitions of what constitutes a neighborhood,
three features are prominent in attempting to
describe just what constitutes a neighborhood.
These three features are the physical structure,
social construction and
functional uses that
combine to create the sense of community
referred to as a neighborhood.
Neighborhoods
defineable.
as
are often considered as discrete,
Particular
areas
within
communities often carry names of some
historical precedence.
These names appear on
maps and are typically thought of as physically
bounded areas. This may be the case with some
neighborhood areas that are contained by
strongly defined boundary conditions such as
rivers or busy streets.
But most neighborhoods,
are not clearly defined as to shape and
dimension and boundaries are more often than
not ill-defined and changeable.
The social construction of neighborhoods which
is based on the networks and interactions
between people has three separate aspects.
These are the social interactions, political
frameworks and cognitive images which define
the neighborhood unit as a social entity.
The
Introduction
Introduction
22
22
are formed
social interaction and aquaintences
of
small
town
Through
the
daily
contact
assitance
of
of
a
however, is the political framework of
today,
where
neighborhoods
live.
they
form
often
short-lived
their
own
third
socially
involves
aspect
This model
and comparable
which consists of the collective
images
of a community's
was
residents
Cognitive
Lynch (1960).
introduced by Kevin
arises.
constructed,
cognitive definitions of local areas.
mental
again
once
cause
another
until
way
subsides
and
and people
is gone
once the threat
together
neighborhood
of
This
is
organization
join
residents
threat to the area in which
against a common
The
families
More prevalent
sense of community is formed.
go
mutual
the
and
generations
many
the
structures.
social
analogy
on
based
is
contact
face-to-face
through
which
in
locations
as
of neighborhoods
idea
images of a sampling of individuals are mapped
a
considered
concensus
forming
thus
neighborhood,
what
create
to
aggregated
and
of
definition
a
be
may
social
a
construct
of the physical form of a neighborhood.
use
The functional
be
can
planning
are
grouped
This
pedestrian
oriented
Intriuctoi
was
Introduction
in
around
school.
traffic
in
observed
concept
seen
of
concept
areas
as
residential
which
structure
an
urban
traditional
the
the
neighborhoods
public
with
ideal
elementary
well
of
areas
little
defined,
through
environment
for
2
23
school aged children and became the model for
many cities and towns throughout the world.
This construction of physical planning units
based on one particular type of function or
service, however, ignores the fact that not all
elements and
have
the
Additionally,
networks are,
functional or
functions within a neighborhood
same
spatial
requirements.
there is no concensus that social
or should be tied to any particular
physical setting.
The concept of neighborhood units in the
design of cities has been criticized as a
planning illusion and also as merely a
physical
element
created by
convenient
planning professionals to ease the design of
communities. It is argued that people's interests
Social
are no longer oriented to local areas.
contacts and friendships are tied to old friends
and co-workers and are widely scattered across
With a highly mobile society,
the community.
shopping, workplaces and schools need not be
located within pedestrian walking distances and
are often aggregated on regional levels.
Even though the neighborhood as a planning
unit has been discredited the concept persists.
When people are asked where they live the most
common response will be the name of a
neighborhood.
The cognitive images of
neighborhoods
are often surprisingly
similar
Introduction
24
24
when compared over a sampling
residents within a community.
of
local
In the case of older people, the idea of the
neighborhood as a planning concept has great
appeal. As the population grows older and less
mobile the need for commercial and service
functions within convenient walking distances
may be critical to the maintenance of people in
The familiarity
an independent way of living.
of the neighborhood environment in which
people have lived for many years can provide a
great sense of stability in what may otherwise
be a time of many changes. Changes related to
the process of aging, such as, in employment
status, family relationships, friendships and
physical
health.
This study will primarily be concerned with the
implications that physical patterns may have on
the provision of services to community
residents.
This is not an in-depth analysis of
facilities or programs designed specifically for
older people though a review of these elements
will take place. Instead, this study is concerned
with the inter-relationship of elements within
the framework of (sub)urban communities.
Research will center on two aspects:
Introduction
2S
25
-
To investigate
as
concept
effective
the use
an
of the
appropriate
planning
of
neighborhood
unit
social
for
the
and
health
and
urban
care services for older people.
-
To
determine
for service
framework
assist
elders
preferred
introduction
Introduction
what
in
living
the
physical
settings is needed
maintenance
of
to
their
situation.
26
26
2 Case Study
The
Community
The Town of Arlington,
utilized
as
usefulness
a
case
of the
planning
Massachusetts
study
in
determining
neighborhood
of service
settings
will be
concept
for
the
in
the
older people.
Arlington was chosen for this case study due to
its characterization
Boston.
suburb
of
With a population of 48,219 people in a
relatively
town
inner-ring
as an
compact
proved
and
nearly
well
ideal
defined
for
area
the
this
case
study
approximately
five
miles
analysis.
The
town
west
and
district
east
is
located
north
between
and
which
from
bisects
commercial
to
activity
transportation
route.
arterial
street
nearly
in
northeasterly
a
Massachusetts
the
major
a
the
largely
major
city
occurs
commercial,
within
city
all
major
another
crosswise
intersecting
Arlington
cultural
on its
this
Avenue,
direction,
along
Nearly
along
the
west.
commercial
lengthwise
Pleasant
bisects
on the
on the
Lexington.
Avenue
business
of Cambridge
occured
Avenue,
Boston
central
of Lexington
development
Massachusetts
trip
Boston's
the City
the Town
Arlington's
street
of
and
Center,
political
center of town.
Case Study
Study - Arlington
Arlington
-
27
27
Several natural features are evident in the
landscape which provide strong boundaries
both within the town and between Arlington
Alewife Brook
and surrounding communities.
and Mystic Lakes define the town's boundary to
Cambridge, Somervillle and Medford to the east.
On the south, Route 2, a limited access highway
separates Arlington from the Town of Belmont.
Boundaries with Winchester to the north and
Lexington to the west are less clearly defined,
areas interrupt
though natural conservation
Natural land features within Arlington
......Lakes
Conservation Areas
Steep Slopes
Case Study
Study - Arlington
Arlington
-
28
28
The town itself
development in both directions.
is dominated by two hills, one on either side of
The eastern
feet from their base at Mass. Ave.
of
portion
the
and
flat
relatively
is
town
of
hundred
three
nearly
rise
hills
These
town.
part
western
the
in
Avenue
Massachusetts
contains a large body of water named Spy Pond.
Land
within
stated,
Massachusetts
Massachusetts
Avenue
residential
apartment
housing
configurations.
between
In
Cambridge
takes
along
high
density
on
density
two
different
part
of
eastern
and
Arlington
is two
of
form
Lower
the
dominant housing type
also
the
in
occurs.
buildings
typically
most
that
development
major
is
It
street.
the
is
Avenue
commercial
As previously
areas.
geographic
defined
well
relatively
is
town
the
within
use
town,
Center,
the
family dwellings.
Land uses within Arlington.
CaeStdl-Aligon2
Case Study - Arlington
29
This
housing
throughout
creates
the
flat
a
consistant
areas
of
western part of town, at a
Boston,
housing
predominance
of
town.
texture
In the
further distance from
development
changes
single
homes.
family
to
a
This
housing type occurs across both hillsides and is
interrupted
only
Massachusetts
by the
higher
density
along
Avenue.
Definition
of
Neighborhoods
Mappings
of
the
neighborhoods
cognitive
has
images
been
of
previously
investigated as a means for the establishment of
service
delivery
(Regnier 1973).
assumption
perceived
locations
for
services
located
cognitive boundaries
have
and potential
the
for use.
It was
topography
be useful
in narrowing the
and
within
accessability
also found
traffic
cognitive
This
congruence
of
that
patterns
can
scale of search due
to the congruence of these ecological
with
the
of a concensus
greatest
land-use,
images
people
This research was based on the
that
neighborhood
older
variables
boundaries.
of natural
local
districts
features
and mental
was
utilized
of
neighborhoods
within the Town of Arlington.
In addition, the
preliminary
definition
cognitive images of the environment
by the researcher,
of local
definitions
a
developed
as well as informal
residents'
as
surveys
of neighborhood
areas, was used.
Case Study - Arlington
Arlington
-
30
30
Through
these methods
the
into four neighborhoods.
These
are either strongly bounded,
Morningside
loosely
bounded
on
and
the
was
as in the case
northern
Heights
on
the
southern
fourth neighborhood
defined
fifth
not
part
of
town
is
hill,
overlapping,
and East Arlington.
located
as
or
Arlington
hill
as
of
with
is
in this way.
defined
located
divided
neighborhoods
Arlington Center
neighborhood
"""
located
town
a
along
the
A
discrete
and
Major Paths
Minor Paths
lIllIllIll Edges - Barriers
Commercial Node
:....::::.... Neighborhood Areas
The spatial organization of the Town of Arlington.
Study -- Arlington
Case Study
Arlington
31
31
approximately two blocks to either side of
Massachusetts Avenue, west of Arlington Center
and extending to the Lexington town line. Most
residents would consider this to be a part of
This
Arlington Heights, which it is by name.
from the
varies greatly
area, however,
The area
residential areas on top of the hill.
along Massachusetts Avenue predominantly
commercial and higher density in character is
separated from the single family areas by a
Hills may be seen as barriers to
travel by older people, thus limiting access
For this reason, in
between these areas.
addition to the different character of land use,
the area along Massachusetts Avenue is not
considered a part of the Arlington Heights
steep hillside.
and will be designated
Massachusetts Avenue Area.
neighborhood
as the
The neighborhood areas which will be utilized
throughout the rest of the case study have now
It is these neighborhood units
been defined.
which will be investigated as to their potential
usefulness in the planning and provision of
services to older populations.
Cas-S--y-
Aligto
Case Study - Arlington
3
32
Neighborhood
Use
A
wide
variety
typically
of
available
areas.
Several
commercial
living
commercial
within
studies
services
within
services
most
have
utilized
independent
are
neighborhood
identified
by
those
older
housing
people
settings
in
terms of their frequency of use and the critical
distances
which
minimize
services (Newcomer
1980).
what
1974,
non-use
Cantor
of
1975,
such
Howell
These criteria are typically used to define
is
called
the
Use
Neighborhood
surrounding a particular building or site.
Neighborhood
which
can be
those
defined
neighborhood
as
A Use
the
area
commercial
services
most often utilized by residents are located.
size
of
Use
Neighborhoods
considerably
depending
characteristics
of
studied.
the
In
the
case
Neighborhoods
pedestrian
population
are
is
In
vary
upon
the
group
older
for
being
people
Use
based
on
the
use
addition,
variable
The
may
typically
travel.
neighborhood
of
in
different
service
needs, as the distance one is willing to travel for
any
use
given service
for
is based on the frequency of
that
perceived
particular
importance
individual.
In
terms
neighborhoods that
available
the
are
those
service-rich
while
service-poor
(Howell
Case
Case Study
Study - Arlington
Arlington
and
service
of commercial
contain a
services
-
of
service
the
services,
large number of
considered
with
to
the
few
to
be
services
are
1980).
33
33
Location of facilities used by distance from older person's home.
Right: This diagram is based on
data from a survey of older
people within the city of New
York. Source: Cantor 1975.
CLUB, ORGANIZATIONS
::
0-20%
Ei
41-60%
21-40%
f
61-80%
MOVIES. THEATER
81-100%
The concept of Use Neighborhoods was utilized
in the case
study of Arlington in a slightly
Since this study involves
modified form.
looking at neighborhoods in general as service
settings
for
older
people,
defining
the
Use
Neighborhood for a particular site was not of
interest. Of importance to this study is locating
those neighborhoods (as previously defined, ie:
East Arlington, Arlington Center, Morningside
and
Arlington
service-rich
or
Heights)
are
either
service-poor.
Study - Arlington
Case Study
Case
Arlington
-
which
34
34
A windshield survey of Arlington was conducted
in
to
order
services
people
Howell).
stores
most
likely to
be
neighborhood
of
locations
defined
(as
by
utilized
older
and
Cantor
by Newcomer,
The services mapped include: grocery
and
beauty/barber
checks)
map
and
supermarkets;
shops;
laundry
drugstores;
banks
(for
services.
All
cashing
parts
of
Arlington, as well as, areas within one half mile
of the city boundary were mapped in this
manner.
A
catchment
area
with
a
3/8
mile
Number of Commercial Uses
IlUse
NNE= 2-3 Uses
40 ~ 3-5 Uses
Neighborhood commercial catchment areas within Arlington
Arlington
Study - Arlington
Case
Case Study
-
35
35
radius (approximately 6 blocks, a critical
distance as defined by Newcomer and Cantor)
was then traced around each mapped service
site. In this way, the community is divided into
areas which either fall inside or outside of the
critical pedestrian travel distances
of older
people.
This
examination revealed interesting though
somewhat predictable results.
Those areas
adjacent to Massachusetts Avenue contained the
greatest number of commercial services.
Often
all five service types are located in close
proximity to one another with overlapped
service areas making this a very service-rich
area.
This pattern covers much of East
Arlington and Arlington Center.
To a lesser
degree the commercial node along Massachsetts
Avenue in Arlington Heights has the same
characteristics.
Not surprisingly, at the other
extreme the single family neighborhoods of
Morningside and Arlington Heights are very
service-poor.
In many instances large portions
of these neighborhoods contain no commercial
services within the defined pedestrian travel
distances.
Older people, as well as others dependent upon
pedestrian travel, living in service-poor areas
might
experience
difficulties
in
the
maintenance of an independent life style.
Case
Case Study - Arlington
Arlington
-
36
36
Where Older People
Contrary
to
popular
Live
belief,
the
majority
of
people over 65 years of age are not fleeing their
homes
and
neighborhoods
to
move
into
age-segregated
retirement
communities.
Instead, evidence suggests that old people are
staying within the single family homes and
neighborhoods in which they have lived and
raised their families.
Homeownership
amoung
people over the age of 65 is exceeded only by
those 45-64 years old. The trend of high levels
of home ownership by older people is expected
to continue, and increase, well into the next
Living Situation of
Older Americans
(Summary of National Data)
decade when it is estimated that 80% of all old
people will be living in their own owned homes
(Special Committee on Aging, U.S. Senate 1986).
13%
2%
5%
74%
6%
private agesegregated hsg
nursing homes
public housing
Contributing to this trend is the low mobility
rates exhibited by older people. On the average
only 2.2% of all homeowners over the age of 65
change residence in any given year and 61% of
those that do move remain within the same
county of previous residence (U.S. Bureau of the
Older people generally prefer to stay
Census).
in the
cities
and
they are familiar.
tendency
for
neighborhoods
with
which
Studies have documented the
older people
to
maintain
their
own homes
familiar living situation even
other (ie: rent,
with child etc.)
would potentially trigger a move (Byerts 1981,
when life-events
Howell 1981).
Case
Case Study
Study - Arlington
Arlington
-
37
37
These factors have combined to create a
situation where older people are Aging in Place.
Aging in place refers to the phenomenon of
older householders remaining within the same
homes they occupied during their middle-aged
years.
It is believed that residential segregation
of older people will decline over time due to the
aging in place of suburban residents.
Residential
Integration
There have already been substantial increases
in the population of people older than 65 living
in suburban communities and the numbers are
increasing steadily.
The average population of
older people in suburban communities is now
11.8%.
These trends suggests that at least in
terms of residential distribution, persons over
the age of 65 are becoming more similar to the
rest of the adult population (Tierney 1987).
These trends are confirmed in the case of
Arlington.
There are 8032 people 65 years or
older living in Arlington. This is equal to 16.8%
of the total population, substantially higher
than the 11.8% nation average within suburban
areas. Of the total number of old people 44% are
in the category of older-old.
In order to determine the level of segregation of
older people in terms of locational distribution
within the town an analysis of census data was
undertaken.
The percentage and total numbers
Case Study
Study - Arlington
Arlington
-
38
38
of people 65 years and older was calculated at
the block level for the entire town and mapped
in order to determine locational concentrations.
High percentages of old people were found
through
out
the
community
having concentrations
Highest concentrations
with
few
of less than
were located
areas
10%.
along
Massachusetts Avenue in areas of higher
This is in part attributed to
density housing.
housing
age-segregated
public
five
developments
which contain
650 individuals.
Arlington Average = 16.8%
Percentage of population over 65 years of age within Arlington.
Case Study
Study - Arlington
Arlington
-
39
39
within
the
single-family
neighborhoods
of
Arlington
found
between
Whereas
Arlington
a
of
place
younger
slightly
into
this
housing
stock
was first
populations
actual
older was
also
were
not
newer
the the
aging in
population
which
when
the
constructed.
years
and
of the
five
neighborhoods
as
65
of people
calculated
determined
previously
25%
increased
neighborhood
moved
The
due
of older people
densities
of
with
area
experience
soon
will
housing
an
Morningside,
that
several
the researchers
It is
in Morningside.
observed
guess
magnitude
this
of
concentrations
excess
in
densities
with
areas
neighborhoods.
contained
Heights
and
observed
were
two
these
however
residential
Heights
Difference
Morningside.
also
were
people
old
of
numbers
Significant
for each
follows:
This
-
East Arlington
Arlington Center
Arlington Heights
Morningside
2400
1600
1300
1100
-
Mass. Ave. Area
Total
1600
8000
population
significant
occured
of
levels
shows
aging
evidence
that
place
have
in
in the Town of Arlington within all its
neighborhood
to continue
and
analysis
areas
and that this trend is likely
as the population of people 65 years
older increases
Case Study
Case
Study -- Arlington
Arlington
into the future.
40
40
Needs of Older People
Service
on a neighborhood
required by older
of services
and the magnitude
the types
are
These
basis.
services
care
long-term
planning
of
viability
the
determine
to
order
in
investigated
be
must
which
of need
two components
are
There
Starting from a hypothetical base of 100
people.
individuals 65 years of age or older, it is possible
to
institutional
either
of
nature
Non-instituional
well
skilled
II)
&
care
as
nursing
care
intermediate
or
Personal care facilities
are
analysis due to
in the
supervisory,
strictly
providing
care
will
informal
assistance
health
care
with
received
care
include
including
setting
community
the
as,
care.
care.
non-nursing
and
either
not included
specifically
within
defined
III).
facilities (level
their
I
(levels
facilities
be
will
within
recieived
requiring
non-institutional
or
care
Institutional
of people
percentage
the
estimate
activities,
daily
received
assistance
formal
as
either
in the home or at a community based setting.
Institutional
Most
the literature
of
nursing
home
other long-term
been
Care
estimated
over
population
utilization
date
to
care service
that
the
Case
Case Study
Study - Arlington
Arlington
-
to
the
of
on
exclusion
of
utilization.
approximately
age
focused
has
65
5%
are
It has
of
living
the
in
41
41
Studies also
Soldo
1984).
home
utilizatiion
the
For those between
that nursing
suggest
with
increases
and 74 the
is only
likelihood of institutionalization
age.
increased
of 65
ages
and
(Manton
time
one
any
at
homes
nursing
but
2%
for those over the age of 75 this rate increases
to
Policy
of Health
Office
23,
August
adopted
use
1983
its own
for
need
the
Guidelines
beds.
home
nursing
additional
developed
has
determining
for
guidelines
of Massachusetts,
Commonwealth
The
7%.
following
the
formulas:
Age 65-74
Age 75+
8.8 beds/1,000
15.5 beds1,000
58.3 beds/1,000
55.3 beds/1,000
Level II
Level III
In other words, 11.36% of all people over 75 and
2.43%
of those between 65 and 74 years of age
at
will
long-term
in
point
any
given
care
services
within
require
time
an
institutional
setting.
As
indicated
people within
old-old
of
of
population
older
of Arlington contains
individuals
within
Of all individuals
age group.
age of 65,
while
the Town
number
significant
the
earlier
a
the
over the
56% are between the ages of 65 and 74
44%
Considering
are
75
of
increased
the
institutionalization
years
and need
Study -- Arlington
Case Study
Case
Arlington
for
age
and
incidence
long-term
older.
of
care
42
42
City of Arlington - 1980 Census
Population by Age Groups
>75
65-74
54-64
44-54
age groups344
(in years)
24-34
14-24
4-14
0-4
0
2000
4000
6000
services
of all types
as people
1987),
this
percentage
individuals
high
can
thumb
used
when
using
in
greatly
age
care
data
old-old
the
rules
service
which
10000
(Wingard
of
influence
long-term
population
8000
of
planning
does
not
separate out this older-old group.
As indicated earlier the prevelance
rate for the
institutionalization of people 65 years of age and
older is 5%.
How does
anticipated
rate
Town
Arlington?
of
population
data
for
for
this compare
people
living
Using
to the
within
the
dis-aggregated
older people
in Arlington
(ie: 56%, 65-74 years of age and 44%, 75 and
older) one comes up with a bed need equaling
6.36% of all people 65 years and older.
Given an
older population of 8032 individuals the total bed
need calculation for Arlington
equals 510 beds
compared to 402 using the 5%
national rate,
an
increase of 27%.
Case Study
Study - Arlington
Arlington
-
43
43
A comparison of the calculated bed need to the
total supply of 122 beds (found in a survey of
existing
services
within
Arlington)
demonstrates a shortfall of 388 nursing home
beds within the Town.
This shortfall indicates
that over 75% of all older residents of Arlington
requiring nursing home placement must find
care within a different community or are cared
for at home.
It should be noted that the population of older
people utilizing nursing facilities as determined
by these formulae is not a static population.
Cross-sectional data of this sort is merely
representative of the total number of people
using a resource at any one time. It gives no
indication as to the highly varied movement
which takes place between nursing facilities,
hospitals and the community.
A
study which followed persons admitted to
nursing homes demonstrates the dynamic
nature of these movements over a two year
period (Lewis 1985).
Approximately 40% of
those discharged from nursing homes either
went home immediately (30%) or after an
intermediate stay in the hospital (10%).
This
movement is highly indicative of the nature of
nursing home resident movement.
The
implication of this for long-term and cotinuum
of care planning is that nursing homes are
Study - Arlington
Case
Case Study
Arlington
-
44
44
currently
serving
the
community
at
single
With outreach services
points in time.
preceding and following institutionalization, it
is possible that facilities could penetrate an
market
untapped
within
their
local
communities.
Right: Movement characteristics
of first time nursing home
patients. Source: Lewis 1985.
Transfer patterns - nursing home patients. The fractions indicate the approximate proportion of patients moving from one status to
another. For example, about three-tenths of first admissions went home on
discharge, a fourth went to the hospital, a twentieth went to another nursing home, and two-fifths died. Of those going home, a third stayed at
home, a third went to the hospital and a third went back to a nursing home.
Study - Arlington
Case
Case Study
Arlington
-
45
45
Care
Non-institutional
Once
been
have
residents
home
nursing
subtracted from the total population of people 65
or older, there remains 95% who live within the
Of these, it is estimated that
general community.
activities and
75% have no limitations to daily
basis
(National
daily
Statistics,
Health
for
Center
on a
living
of independent
are capable
The remaining portion of the population
1984).
(ie: 20%), however, has some degree of disability
care
as continuous
be
as well
or intermittant,
recuperative
some
either
could
care
This
services.
short-term
which require
in activities
or limitation
and long-term in nature.
A commonly used measure of disability in older
the
is
people
number
continence,
mobility.
These
for
the
are
those
activities which
living and include:
of
the activities
medicine,
transportation,
use
of
are
of
shopping,
laundry,
housework,
money,
Living
preparation,
are
IADL's,
life.
Daily
support
managing
which
activities
of
meal
and
transferring
contination
Instrumental Activities
dressing,
eating,
bathing,
include:
toileting,
essential
IADL
and
ADL's, Activities of Daily Living,
impairments.
measures
ADL
of
taking
telephone
and
mobility outside of the home.
Care
Informal
It is estimated that the number of older people
receiving
informal
Study - Arlington
Case Study
Arlington
-
care
within
the
community
46
46
This care is
is 70% (Special Report on Aging).
to
admitted
homes
of
former
percentage
largest
the
nursing
elderly
women
to
care
to
This is
alone.
living
were
who
to
providing
predominantly
were
care
these care
words,
other
In
institutionalization.
be
prior
immediately
individuals
givers
in
must
measures
data
this
that
remembered
It
1985).
(Smallegan
30%
care
Spouses helped 25% and other
65% of the cases.
kin,
were
givers
care
providing
children,
own
patients
the
that
found
or
recently
people
of
study
A
relative.
other
offspring
spouse,
a
by
provided
typically
derived from the facts that there are three times
more
women
men
and
givers
that
spouses
the situation
in
nursing
within
living
homes
than
the
care
typically
are
husband
and
both men
and
both
when
wife are still living.
Given
increases
the
women
where
a
situation
spouse
will require
life-span
in
for
occur
increasingly
will
who is providing informal
care
Beyond
that,
themselves.
services
as more people live into their 80's and 90's the
possibility
occupy
needs
the
that
their
ranks
of
of their own
Case Study
Case
Study -- Arlington
Arlington
children
the
will
elderly
increases
themselves
with
service
dramatically.
47
47
Community Based Care
Formal care services within the community are
typically broken into two categories, Health are
Health care services are
and Social Services.
those services which involve assistance with
ADL skills whereas social services typically deal
Formal
with IADL skills.
The Commonwealth of Massachusetts, Executive
Office of Elder Affairs estimates that 6% of all
elderly people in the state receive formal care
through state sponsored Home Care programs.
These programs include assistance with any of
following Social Services:
-
Case Management
Homemaker Services
Personal Care
Chore Services
Companionship Services
Social Day Care
Home Delivered Meals
Laundry Services
Transportation
Health Care services are provided through a
combination of agencies and can include:
-
Home Health Aides
Adult Day Health Programs
These services are administered through the
Department of Public Welfare because Medicaid
and Medicare reimbursements will cover many
of the costs involved with health care services.
Study - Arlington
Case Study
Arlington
-
48
48
Adult Day Health Care
care
services
nursing
Day
similar to
home,
Health
but
Care
only
Programs
provide
those
received
as
daytime
Programs
a
are
health
in
a
service.
as
designed
a
100%
all
elderly
livig.i
community
75
within an
institution
|
20
indepnde
........
m.n e ed........ ..........
of....
services...
14
. nformal
coare..
n ly.
.... .....
.. ...
formal. care......
..... ......
......
..
......
.......
...
.....
............
~adul
ho mecare.
.............
day...........
h ealth.
..................
care.
Total...service..needs.
- Ne......
d bein met
.................
through.....formal.....means..
Service Ned
.....
of......
Populatio 65..years...and..Older by % ..
..
of Current.Use.(ummary.of.State.nd.National.Data
Case
Stdy-.
...
rlngon4
services to those in
as, to provide medical
well
on an intermittant basis.
need of such services
for Adult
demand
of
a
Service
of
population
of
Care
Health
Day
1%
approximately
estimates
Welfare
Public
of
Department
Massachusetts,
of
Commonwealth
The
as
givers,
care
informal
supporting
for
means
total
the
older people within a given area.
The diagram
the
on
the
national data.
later
in the
potential
defined
current
of
magnitude
based
page
summarizes
service
utilization
on the preceding
previous
survey
These percentages
study to
market
for
neighborhood
Arlington
Study -- Arlington
Case Study
Case
determine
various
of
state
and
will be utilized
the needs
services
and
within
settings.
so
50
Existing
Services
in Arlington
A survey of services and housing projects
designed specifically for older people within
the Town of Arlington was undertaken in order
to acertain the types and levels of services
Both public and private
currently available.
service providers are included in the survey as
an attempt to document all available sources of
assistance to older people within the town.
Nursing Home Facility
A
Meals Program
Age-Segregated Housing
*
Adult Day Health Care
Existing service settings for older people within Arlington.
Study - Arlington
Case
Case Study
Arlington
-
Si
51
Housing
Age-segregated
There are five public housing projects in the
town designed specifically for older people.
These five projects contain a total of 600
apartment units serving approximately 650
people, or 6% of the age eligible population.
This compares closely to the overall national
percentage of people over the age of 65 living
It
in some form of publicly assisted housing.
should be noted, however, that age is not the
sole eligiblity requirement for such housing.
As is typical for most publicly assisted housing,
income eligibility requirements must also be
met. Because of this a much greater percentage
of those people both age and income eligible are
living in this type of
housing.
Four of the housing projects are located within
three blocks of Arlington Center, the town's
main commercial and governmental center.
The fifth, a 200 unit project, is located in the
Arlington Heights area near the border of
All of the projects are well sited
Lexington.
within easy pedestrian access to neighborhood
commercial facilities and public transportation
routes.
Meal Programs
There are two nutrition sites serving the older
The larger of the two
population of Arlington.
is located within the newly opened senior
citizens center in a former school building in
Study - Arlington
Case Study
Arlington
-
52
52
Arlington
Center.
Winslow
when
This
the
better serve
site has
from
projects,
order
in
to
all town residents and to increase
The second nutrition
within the center.
activity
moved
housing
opened
center
senior
was
of the
one
Tower,
site
in its
remained
housing
Heights
part of the Arlington
as
location
original
a
project
due to its remote location.
meals
sixty
approximately
Together,
day,
per
five days a week, are served at these sites for a
nominal donation of one dollar.
In
addition
to
meals
of
"meals-on-wheels"
meals
people
older
consist
a
of
thirty-five
are
meal
delivered
using
two
programs.
are delivered
the
are
another one hundred meals
homes
at
served
sites
to the
different
Sixty-five
of the
from the nutrition sites and
cold
The
lunch.
prepared
at the
remaining
Symmes Hospital
and include both a hot lunch and cold dinner.
This hospital based program,
with a mandatory
fee of $19/week, has the capability of preparing
"special diet" (ie: low sodium content) meals for
those requiring
such service.
All
other meals,
both home delivered and on-site which are not
prepared
at the
out-of-town
Arlington
hospital
private
vendor
using special
Study - Arlington
Case Study
Case
Arlington
-
are
contracted
and
with
trucked
an
into
vehicles.
53
53
Transportation
Services
The Town of Arlington is served by a series of
public bus routes.
Major service is along
Minor service routes
Massachusetts Avenue.
The
extend into Lexington and Winchester.
neighborhoods of Morningside and Arlington
Heights also receive limited service to the top of
Newcomer (1974) determined the
the hills.
critical distance for public transit access as one
block. An analysis of bus route catchment areas
(in this case two blocks) was conducted to
10-30 minute intevals
30-60 minute intervals
Public transportation catchment areas within Arlington.
Arlington
Study - Arlington
Case
Case Study
-
54
54
determine transit accessability.
Major portions
of the Morningside and Arlington Heights
neighborhoods are not well served according to
this analysis.
Alternative transport is available however.
The
MBTA runs a Dial-a-Ride program for older
people from a garage in Lexington.
The
Arlington Council on Aging also has two vans
These are
capable of transporting wheelchairs.
used primarily to transport Adult Day Care
participants to and from the program.
Home Care Services
All publicly sponsored homecare and personal
care services delivered within the Town of
the
through
Arlington
are
coordinated
Minuteman,
Minuteman Homecare Corporation.
a state designated homecare agency serves a
sixteen community catchment area out of a
single office located in Lexington.
At the present time Minuteman coordinates 433
cases serving 454 individuals (5.6% of all
elderly) in the Town of Arlington.
An
over-representation of clients is located within
age-segregated public housing projects (33%)
which house just 6% of the overall population of
older people.
It is the researchers opinion that
this over-representation is not caused by a
greater need within these settings, but rather
an increased awareness of the availability of
Study - Arlington
Case Study
Arlington
-
ss
55
such programs and the fact that public housing
for
qualified
likely income
residents are
most
participation.
There has been a steady increase
number of cases since the inception of
in the
the program.
in
excess
State-wide this increase has been
50%
of
since
1980
indicating
a
growing need for such services.
There
are
six
case
managers
assigned
to
the
Town of Arlington, each having a case load of
approximately
needs
seventy
cases.
assessment,
follow-up
case
assesments
After the initial
managers
every
three
perform
months,
as
well as, supervision of direct care workers.
Actual direct care services are delivered by any
of approximately six local provider agencies.
Of
these
in
provider
Arlington,
which
area
agencies,
two
within
adjacent
two
are a part
and
two
are
based
communities
of the home care
outside
of the
Provider agencies also provide
catchment
catchment
area.
services to over
income elders on a private pay basis.
Private
pay as estimated by one provider accounts
for
between
30% and 40% of the total number of
clients
served.
Given
these
figures
it
is
estimated that 9% of all older people in the Town
of Arlington are receiving some type of formal
care
services.
As
compared
to
the
reported
national average of 6% older people in the Town
of Arlington
are relatively
Case Study - Arlington
Arlington
-
well
served.
56
56
Association
Nurses
Visiting
A Visiting Nurses Association office is located
No data as to the
within the Town of Arlington.
of cases
number
agency
this
through
handled
was available, but it may be safely assumed that
services
from
services
are
will also receive
service
most clients of VNA
VNA
Many
sources.
other
medical
expenses
required after an acute hospital stay.
Services
as
reimbursed
provided by the
with
somewhat
overlap
VNA
personal care type services offered by the home
are normally
services
care agency though VNA
limited to shorter durations.
Care
Day Health
Adult
A thirty-six slot Adult Day Health Care program
Corporation
care
Home
of
total
this
individuals
fifty-eight
Town
the
thirty
come
far
Difficulties
remote
hour
of
Arlington,
participate
in
day
the
a
remaining
communities
surrounding
from
as
and
Wilmington.
arise out of the long
commute from
as
away
A
Twenty-eight participants are
week per person.
from
Center.
of three
for an average
program,
the
within
located
in Arlington
facility
senior center
is
Minuteman
the
with
association
in
operated
Woburn
communities.
program,
those
to attend
In order
individuals
farthest must often spend from
a
travelling
six
the
1 to 1 1/2 hours
each way aboard a van while other participants
are picked up and dropped off.
Study - Arlington
Case Study
Arlington
-
S7
57
Over 40% of the clients participate on a private
from
A
community.
greater
the
been
also
has
program
respite
bed
ten
services
indicating a need for these
pay basis
established by Symmes Hospital, both as a way of
a
need
for
community
and
to
meeting
under-utilized
provides
both
services
for
capacity.
day
and
illness,
through
either
whose
individuals
program
This
health
care
normal
care
overnight
to
unavailable
are
givers
bed
from
income
gain
the
in
services
such
provide
services,
situations
emergency
or
the need for a break from the demands of daily
provision.
service
There
two
are
long-term
of
Town
the
within
Facilities
Care
Long-term
facilities
care
located
Wellington
Arlington.
Manor, three blocks from Arlington Center is a
Park Avenue
42-bed Level III nursing facility.
Nursing
Home,
a
facility,
multi-level
near
Arlington Heights contains 40 level II beds and
40 level III beds for a total of 80 beds.
Though the 122 beds listed above are the only
long-term
care
boundaries,
four
facilities
within
homes
addition nursing
inside Lexington
three miles
by individuals from Arlington.
the
are
town
two or
often utilized
Combined these
facilities provide another 545 beds of long-term
care
capacity.
Study - Arlington
Case Study
Case
Arlington
-
S8
58
Segmentation
in
Service
Delivery
When it comes to the provision of services to
older people a wide array of services can
normally be found within most communties as
demonstrated in the survey of services provided
in the Town of Arlington. Services are typically
provided either privately or through a variety
of publicly-funded service organizations.
Some community services are available to
everyone at minimal or no cost, while others
For
are tied to income eligibilty guidelines.
example, residents below a certain income level
may be eligible for some free services such as
respite care while others must pay on a sliding
fee basis.
Still other "over-income" residents
may not qualify for any services at all.
For those in need of services, locating,
determining income eligibility and maintaining
contact with appropriate service providers can
There are few clear
be a bewildering task.
paths into the service provision system and a
great many services are provided by multiple
service provider groups.
and overlapping
In the case of homemaker services an older
person must first contact the local homecare
corporation to determine whether they are
eligible for services based on income level. If
so, a case manager is assigned and services are
Study - Arlington
Case Study
Arlington
-
S9
59
On the other hand if income exceeds
eligibilty levels a private pay home care
Ironically, the
provider must be located.
private sector service provider found in the
community would very likely be the same one
that provides services to the homecare
corporation on a contract basis. In the case of
provided.
health care services a different organization
Health care
must be approached for help.
services are reached through an entirely
different point of access. From an older person
in needs of services there is no clear means
This situation is
access into the system.
especially acute in the case of middle class
people who generally resist seeking assistance
from social service agencies due to the stigma of
social service programs as services for the poor.
Segmentation in Planning
If the provision of services appears fragmented
and difficult to understand, the planning of
service delivery systems is equally complex.
Though essentially targeted at a single
population group (ie: people older than 65) the
planning of services for older people is also
split into the two areas of health and social
services.
The planning of health care services is
historically geared toward the production, or
limitation of bed capacity of medically oriented
care facilities within Long-Term Care Services
Study - Arlington
Case Study
Case
Arlington
-
60
60
areas.
Long-Term Care Service Areas, or LTCSA's are
geographic
areas
Department
of
districts
for
designated
Public
long-term
by
Health
care
the
as
State
planning
facilities.
All
proposed additions to the the number of nursing
home
beds
within
Massachusetts
must
Determination
process.
the
of
Commonwealth
proceed
Need
or
of
through
D.o.N.
a
application
The D.o.N. is used to determine whether
a need for additional nursing home beds exists
within
an
given
determination
LTCSA.
is
based
nursing home utilization
the Department
beds
on
needs
projections
for
according to data from
of Public Health's,
Health Statistics.
home
This
Division of
If there is a need for nursing
within
an
LTCSA
a
nursing
home
nover
owAndover
Ciy-Tewksbury
Middleton
ChelmsfordN
Westford
Readig
Billerica
ttleton
Carlisle
>Zr AcoM~
[g
eadin
Ew-
S
L
o ac eD
DC
tn
City
it
Bedfordc lle
S
Saugus C
i
Concord
The Long-Term Care
Right:
which
Service Area (LTCSA)
includes the case study town of
Arlington. Source: Commonwealth
of Massachusetts , Department of
Public Health.
>w
ay
etford
Waltham
City
Rever
Ma
*et
.
Sudburryt
Peal
C
rlCt
s...on
stycW
camCo
c,
City
e14
:>Way-Wetn1
#ane
Case Study
Study - Arlington
Arlington
-
,,..,R***
S-
61
61
Areas.
Service
community,
study
case
our
Arlington,
nursing
a single
preclude
homes
nursing
its
for
constructing
from
communities
other
residents
own
concentration
of
nursing
can
small
geographic
areas
case
of Arlington
as
on
the
development
of
indicated
nursing
within
facilities
be
observed
in
the
on the diagrams
trace
which
page
following
since the
met.
bed capacity for the LTCSA is already
A
would
area
single
a
within
facilities
care
in
a concentration of
Such
any of the six towns.
located
facility
nursing
scale
large
within
be placed
potentially
Area could
Service
this
within
needed
beds
home
is
Any or all of
comprised of a total of six towns.
the
includes
which
LTCSA
the
example,
For
adjoining
within
occur
may
development
In some cases
Area.
Service
boundaries of the
the
within
anywhere
developed
be
may
homes
in
the
Arlington
over the last thirty years.
Viewed
passage
from
historical
this
perspective,
and Medicare
of Medicaid
legislation in
1966 had a vast impact on the development
physical
this
form
of
long-term
care
the
facilities
and
in
country.
Case
Case Study
Study - Arlington
Arlington
-
62
62
Development of
Nursing Homes
in Arlington
The first nursing homes serving
began
Arlington and Lexington
as small facilities serving 20 to
30 residents from the local area.
Accomodations were contained in
large residential stuctures, after
minimal renovation, either in
city neighborhood areas or on
former rural estates.
After the passage of legislation
establishing Medicare and
Medicaid in 1966 the nursing
home industry began a period of
rapid growth. Based on a medical
model of care, nursing homes
increased in size to 80 beds.
Newer homes were constructed
outside of built-up areas, older
homes expanded.
Expansion continued with the
reconstruction of older facilities
and the further development of
new ones. Major growth occured
in outer areas with the building
of large nursing homes (160-200
beds) on relatively inexpensive
land in open suburban areas.
Case Study
Study -- Arlington
Arlington
63
63
In
order to better
of
the
analysis
of the
associated
of
context
within
existing
surveyed
as
part
services
will
be
characteristics
of
of Age,
homes
Arlington
Size
an
community
facilities
at
and
settings
organizational
the
looked
spatial
service
nursing
Those
the
the
these
with
conducted.
downtown
understand
relationships
locational
Settings
Service
of
Characteristics
in
patterns
be
will
previously
survey
terms
of
and Distance
of
the
from
Boston.
lies
lies
(
Distance of Case Study Nursing Homes from Downtown Boston
Study - Arlington
Case Study
Arlington
-
64
64
study of the locational
In a
urban
elderly
it
was
characteristics
make
evironment
the
a
settings
of
older
for
One of the attributes used to
people (Carp 1974).
determine
settings
good
those
"city-ness"
elements which contribute to the
an
that
determined
of
degree
from
distance
was
surrounding
of city-ness
the
central
business district of the major city in a regional
This measure was used in the following
SMSA.
analysis of nursing facilities.
As indicated by the following chart there exists
a
direct
correlation
the
concerning
age,
As
facilities.
construction
they
the
of
and
size
location
of
newer
in
and
are
are
facilities
increase
characteristics
in
size
located within less densely populated
Age
date
Facility
site
1962
1972
1965
1966+
1972
1968+
A
B
C
D
E
F
Size
# beds
areas.
Distance
miles
6
7
10
9
9
9
42
80
81
104
158
202
It should be noted that two of the facilities (sites
D and F) have expanded their existing buildings
after
original
occupancy
Case Study
Study - Arlington
Arlington
-
and
that
a third
(site
6S
65
B) was built on the site of a previous smaller
scope
limited
in
nursing
facilities
area,
these
using
a
small
within
a
limited
of
inter-relationships
of
the
is
long-term
care
is rather
number
of
geographic
researcher
that
characteristics
for
the
opinion
it
analysis
Though this
nursing home.
facilities would
be
replicated
in
studies.
subsequent
analysis
Subsequent
of
three
representative
facilities from the previous sample, ie: Sites A, B
and
The
E.
environment
immediately
surrounding each of these facilities was mapped
and population densities calculated in an area of
one square mile around the site.
Population Density and Nursing Home Size
by Distance from Central Boston
Interpreted Data: 1980 U.S. Census and
Massachusetts Department of Public Health
left:
people/
sq. mi.
right:
# beds
10000
200
8000
150
6000
40000
4000
100
pop. density
n.h. size
50
2000
0
0
8
9
7
Miles to
Central Boston
6
Case Study - Arlington
Arlington
-
66
66
Site A, a small 42 bed nursing
home is located immediately
within a two-family residential
area in Arlington Center. The
facility is actually a large old
house which was renovated with
an extension added to the rear.
THe character of the building fit
directly in with the surrounding
neighborhood since the front of
the building was one of the
the
original structures in
neighborhood.
CCML7 OIV
a
0
0
0
Sa
Arlington
Case Study
Study - Arlington
-
Lzc
67
67
Site B, is located within a
single-family area of Arlington
The facility originally
Heights.
occupied an old mansion. The
existing facility, with 80 beds,
was built in 1972 and the former
building torn down after the
The
residents were moved.
of
that
is
facility
the
character of
building.
a mid-sized apartment
a Qgp
o
0,
f
102
%1
Ca
a
0
zoo1 6
00
L V
Study - Arlington
Case Study
Arlington
-
68
68
Site E is a large multi-level
nursing facility with 158 beds.
Though this facilitry was also
built in 1972 site location and
physical design characteristics
are quite different from those of
Site B. The facility is located in
density
areawith low
an
single-family housing to one side
and a medium density apartment
complex on the other. The site is
not served by any form of public
transit and a shuttle bus is used
to carry employees to the Bus
line. The design of the building
adopts an institutional character.
1?
C3
c
C
%
M
r, Eo; E
-
I?
0
flI
c
11
CM
C
oe
I
..........
Case Study
Study - Arlington
Arlington
-
69
69
This examination further comfirms the findings
Interestingly, the
of the previous sampling.
larger facilities also tended to group near one
another creating an area in the town which
could potentially be dominated by institutional
This may be attributable to any of
settings.
several factors such as, low land costs or liberal
The location of 464
zoning requirements.
long-term care beds within a small area such as
that in our case study has little relationship to
the demand for nursing care services on a local
level. This is surely a result of planning on a
large scale regional level.
Home Care Catchment Areas
Home Care Catchment Area
which includes the case study
Source:
town of Arlington.
Commonwealth of Massachusetts,
Executive Office of Elder Affairs.
are
geographically
a single Home Care
Home Care services
Agency
delivered to income eligible individuals within
In the case of Arlington,
the catchment area.
defined
in which
coordinates all
areas
Case
Case Study
Study - Arlington
Arlington
-
70
70
Minuteman Home Care with offices in Lexington
provides
all
case
referrals
for
residents
of
in
the
provision
services
are
delivered
role
providers
19
communities.
a Case
Minuteman serves mainly
of
by
Management
Actual
services.
home
private
throughout
located
service
and
management
care
thecatchement
To a certain degree the actual providers
area.
are
with
competing
one
for
another
referrals
Minuteman.
from
All
home
to
the
eligible
income
for
are
providers
by Minuteman
referred
services
care
The actual care providers also offer
individuals.
services on a private pay basis to people who do
not
meet
guidelines.
income
pay
estimated that private
One
provider
customers
accounted
for 30% to 40% of his business.
Institutional
It is
vs.
resonable
Community
to
assume
Services
that
the
growth
in
Home Care services has reduced the need for the
production
of
According
to
additional
a
nursing
sampling
of
home
beds.
home
care
recipients in 1983, it was estimated that 30% met
the
requirements
homes
for
placement
Commonwealth
within
nursing
of Massachsetts,
EOEA).
An estimated 16% of these would actually have
sought
homecare
placement
in
a
nursing
home
if
services had not been available.
Study -- Arlington
Case Study
Arlington
71
71
The
of both
size
community
the
based
increased
growth
in
strong
long-term
older
nursing home
Using
beds
of
and
long-term
segmentation
of
mechanisms
areas
planning
and
growth
their
into
the
of both
practices
the
two
services
will
grow
and
The
community-
their
funding
geographically
A
that
another.
out
by
services.
community
systems,
strategies.
suggests
the
one
point
caused
built
institutional
and
systems
be
care
of
service
catchment
guide
planning
independently
based
to
and
services
to
need
current
systems
for
care
populations
formulas
based
institutionally
demand
linkages
planning
the
the
defined
need
for
consolidated
new
planning
process must be developed to balance the supply
of all long-term
care
Neighborhood-based
potential
service
for
us
to
care
our
question
This
service
original
of whether
is a useful
services
service
providing
network.
long-term
services.
planning
settings
such
a
need for
delivery
unit
a consolidated
That
neighborhood
in
the
consolidated
system
investigation.
the
have
returns
is,
the
concept
the provision
of
for older people.
Study -- Arlington
Case Study
Arlington
72
72
3
A
The Model
Neighborhood
Service
Setting
In the preceding analysis two key criteria for
the development
settings
for
investigated.
of neighborhood-based
older
people
service
have
been
These are:
- The concept and definition of
neighborhood as a planning unit.
the
- A definition of the service needs of the
population of older people.
By
utilizing
the
neighborhoods
as
defined
applying
within the case study community and
estimates for service needs of older people it is
possible to determine the magnitude of service
needs within each individual
area. These needs are as folllows:
Neighborhood
East Arlington
Total
Population
( 65+ years)
Nursing
Beds
(@ 5.8%)
Community
Need
(@ 20%)
Formal
Homecare
(@ 9%)
neighborhood
Adult Day
Health
(@ 2%)
2400
140
480
216
48
Arlington
Center
1600
92
320
144
32
Arlington
Heights
1300
76
260
117
26
Morningside
1100
64
220
99
22
Mass. Avenue
1600
92
320
144
32
Estimated Magnitude of Service
Needs
Th....
M odel. by Neighborhood
...... Area within Arlington
73........
The Model
73
Some modifications to the magnitude of need as
defined
in
order
to
earlier
sections
better
represent
community
and to reflect
which
likely
are
services
to
are available.
higher
than
than
based
on
arriving
at this figure
programs
nursing
health
care
6.8%
will
current
level
was
it was
of 9%
there remains over
people
receiving
to
contain
requiring
of
being
Given
only
individual
clearly
significant
these
settings
The Model
Model
utilizing
In
within
the
to
care
need
for
adult
day
2%.
Home
placed
at
the
Arlington,
ie:
6%
private pay.
high
that the
home
case,
was
Even with
program
informal
in
utilization
the
the
care.
chart each of the
the case
numbers
long-term
levels
for
and
increased
of
care
units
study
appear
old
people
of
services.
service
neighborhood
exists
Arlington
assumed
the
but
10% of the population of old
defined
various
of
This
average
reduce
As indicated by the preceding
neighborhoods
types
for
health
utilization
assumptions
study
characteristics.
publicly funded plus 3%
these
in
magnitude
all
calculated
day
This
utilization
service
when
effectively
beds.
in
national
population
of adult
case
of all older people.
5%
lower
availability
our
made
Nursing home utilization
the
the
been
changes
occur
has been taken as 5.8%
is
have
needs
the
establishment
neighborhood
within
potential
of
service
concept.
74
74
The Nursing Home A Consolidated Service
With
in
increases
the
Setting
population
65
of people
years of age and older there will be an growing
need
care
for long-term
nursing
including
services
adult day
homes,
care
programs,
meals
neighborhood
commercial
facilities.
the provision
of these
and other
home
logical
for the nursing
role.
The
of all
home
development
types,
health care,
and
programs
to
To
assist in
services
play
it is
a central
of neighborhood-based
service settings will allow the provision of a full
range
of services
to
the
entire
homes
in
community
of
older people.
The use
of nursing
this manner
been described as the provision of a
Care Spectrum (Breger
care
spectrum
provision
people
of
involves
all
from
1985).
a
services
single
required
nursing homes can provide
from
requiring
this
in-home
housekeeping
services
for
level
people
for themselves.
retirement
settings
continuum
through
and
who
are
older
this
way,
range of
for
those
services
personal
capable
to
by
a
capable
of
Unlike
development
CCRC's,
of
care
continuing
providing
to
of caring
neighborhood-based
of care.
the
care
intensive
Similar
center,
are
of
In
a complete
in-patient
long-term
comprehensive
source.
services
Long-Term
The
the
has
care
service
a
total
however,
neighborhood-
based service settings older people would not be
required
The Model
Model
to
move
from
their
familiar
75
75
surroundings in order to receive care.
The concept
dispersed"
"geographically
of the
CCRC is under development by Brandeis
University and Friends Service for the Aging
In this model, enrollees would
(Pynoos 1985).
pay an entrance fee, in addition to monthly
fees, in order to guarantee the receipt of
As
various health and long-term care services.
services are needed they are either provided
within the enrollees home or at a facility
I
I
Homemaker
.
Services. ....
.. . ... . .
...Health
*~~E.
*
Care.
~
.
Care...
Proa
Se.ices
_.
...
.... .... ... .
Manaemen
eg b rh o
~ .... ..... '
........
Com ercial.
N eighb orh oo..............
......................
Model
A......
forNeihbohod-bsedSeric
Settings.
for Older.Commnity Resident
The Model....
76..
utilized
by
the
sponsoring
organization.
Essentially, the geographically dispersed CCRC is
and facilities brokered
a network of affiliations
together
to
provide
guaranteed
situated
ideally
would
be
provide
this
form
of
care
residents
to
at
a
level.
neighborhood
Size
to
long-term
guaranteed
settings
service
Neighborhood-based
services.
Facility
of
The minimum feasible size of 120 beds is often
sited
the
for
1985,
against
the use
case
older people
nursing
homes
might
and
as
of neighborhoods
planning units.
study
1980)
Aranyi
(Breger
care
of
development
argue
long-term
Only one in five of our
enough
neighborhoods
contained
to support this
size facility.
An
analysis of the size distribution for all licensed
nursing
facilities
within
produced
Massachusetts
the
Commonwealth
interesting
of
results.
Nursing Home Size Distribution Source: Commonwealth of Massachusetts
Department of Public Health Data Base
60
Number of
Nursing
Homes
50
40
30
20
10
0
110
4150
8190
121130
161170
201210
241250
Size by Number of Beds
The Model
77
77
As indicated by the chart above, a majority of
nursing homes contain fewer than 90 beds and
significant
numbers
have
within the facility.
50
and
fewer
beds
In fact, very few nursing
home contain 120 or more beds.
It has also been pointed out that the benefits of
quantity
(ie:
maximization
increased
pronounced
whether
quality
within
size
(Ullman
of
and
nursing
of care or simply
homes
facilities)
1987)
large-scale
nursing
the
homes
serve
is
not
issue
of
increase
as warehouses
for older people is being debated.
In the case of Adult Day Health Care Programs a
neighborhood
sized
The preferred
size of programs
state Medicaid
shows
the
health
programs
size
unit
appears
is 24 people.
distribution
in the
nearly
ideal.
funded through
The chart below
of
all
adult
day
Commonwealth.
Adult Day Health Care Size Distribution Source: Commonwealth of Massachusetts
Department of Public Welfare
25
number 20
15
of
programs 10
5
16- 2120 25
Nearly
The Model
all
26- 31- 36- 41- 46- 51- 5630 35 40 45 50 55 60
individuals / program
programs
have
fewer
than
30
78
78
services at reasonable program
sizes.
services have
and home care
Case management
for these
demand
adequate
have
neighborhoods
study
case
our
of
five
all
rate,
a
have
Given a 2%
16 and 25.
capacity of between
utilization
50%
approximately
and
participants
few constraints in terms of efficiencies of scale.
a
assure
laundry,
are
already
a
Opening
such
residents
could
be
increase
only
neighborhood
to
services
more
housing facilities
difficult
facilities.
home
nursing
of
item sales
many
though
of
viability
the
Grocery and convenience
operations.
may
part
pharmacists
and
shops
beauty/barber
as
such
services
commercial
Neighborhood
residents.
to neighborhood
of care
monitoring
continal
and
approach
comprehensive
help
would
setting
same
this
from
provided
services
care
Direct
settings.
of neighborhood
out
be based
and
areas
neighborhood
assigned
could easily be
Home Care
through Minuteman
operating
currently
managers
case
6
The
elderly
and CCRC's offer this service
with a market of fewer than 300 residents.
As additional services such as adult day care and
home
care
community
made
an
expanded
This expansion
can
nursing
of
expensive
in-patient
increasing the feasibilty
Model
The Model
market
to
contribute
dependence
home
bed
the
to
available
are
is
greater
produced.
the
reduced
on
revenues
capacity,
thus
of smaller facilities.
79
79
Neighborhood
the
to
Relationship
are
concept
of neighborhood
the
ways.
several
a functional use the need for long-term care
As
neighborhood
homes
already
which
need
capabilities
are
nursing
settings,
neighborhood
by
shops
beauty
stores,
within
located
were
Nursing
homes.
of
services
these
available
made
be
and
already
facilities.
As
physical
service
settings
point for
entry
imagable
familiar
A
people.
older
to
and
within
inherent
by
required
Services
A great many resources
provided
an
in
services.
many
to
only
elders.
as
of
contain
community
serve
terms
their
of
distance
walking
are
they
if
people
older
areas
would be of great benefit
facilities
laundry
neighborhood
drug
and
as grocery
such
and
commercial
neighborhood
a
health
addition
service-poor
be
to
found
and
many
on
exist
to
In
level.
services
social
to
shown
been
has
services
to
in
units
older
encourage
and
with
consistent
people
for
settings
service
Neighborhood-based
would
services
setting
where access to services is assured.
The
and
imagability
neighborhood
provision
to
as
a
planning
people
older
for
unit
has
other
the the provision
of information
positive
and entry
of community
day care services geared
dementia
Model
The
The Model
patients
was
in
into
In a recent
service systems is well documented.
non-utilization
the
service
The importance of informal linkages
factors.
study,
of
familiarity
respite
and
to assist caregivers for
attributed
to
caregivers
80
80
strangers
(Caserta
settings
would
problems
service
settings
the
utilization
the
establishment
of
component
of
inherent
an
and
such
through
as
service
Neighborhood
1987).
alleviate
referral
in the care of
ones
not wanting to leave loved
framework.
urban
A final benefit to the provision of services on a
quality of care provided
in the
increase
for
potential
the
is
level
neighborhood
within
in the case of
As pointed out
nursing homes.
an
free-standing
unlike
CCRC's,
(Branch
1987)
nursing
homes,
independent-living
eldery
nursing
home is
arises
need
the
and
incentive
that
assuring
in
if
the
have
therefore
interest
go
will
they
where
their own
that
know
residents
their
nursing
and
vested
home
is
the kind of environment they would like to live
arise.
in should the need
This
service
neighborhood
that
knowledge
the
a
much
now
Through
the
setting
sense
"belongs" to
ownership
of
assuring
and
quality
As the population ages the potential exists
that neighborhoods
the
to
developed
be
may
transferable
settings.
a particular
neighborhood
community
care.
directly
is
concept
quality
as
of
might someday
their
long-term
neighborhoods
judged
by
the
and
quality
be judged
care
services,
communities
of
their
by
are
school
systems.
The Model
Model
81
81
Conclusion
There is little doubt that the population of older
in
increase significantly
within
living
of older people to
development
of
based service
systems
This
to
reexamine
a
of
utilizing
in
the
planning
settings
consolidated
and
planning
and
community
at regional levels.
advantages
concept
service
care
the
institutional
demonstrated
study
need
segment
which
provision
suburban
long-term
of
models
current
trend
single-family
indicates
neighborhoods
This
the future.
combined with the preference
remain
will
services
social
and
health
requiring
people
the
and
usefulness
the
neighborhood
development
and
for the
designed
of
provision
of health and social services to older community
Yet,
service
settings
opposition
from
face
could
homeowners
of
single-family
within
neighborhoods
residential
of a system
implementation
residents.
who
are
strong
unaware
of the need for these services at a local level and
service providers
from
invest
in
priced
land.
To
further
facilities
the
service settings
are
-
not choose to
who may
of reduced
establishment
scale
of
areas
on higher
neighborhood
the
following
of research
of
of
means for encouraging the
neighborhood
settings, by
suggested:
Investigation
development
Conclusion
Conclusion
82
82
zoning ordinances
of restrictive
removal
and the purchase of potential building sites
strategically located within neighborhoods.
-
Techniques for limiting the size of new
facilities to meet only the market demands of
neighborhood
surrounding
immediately
areas as opposed to current regional market
considerations.
-
Research into the acceptability of service
settings within residential areas in terms of
These studies may
scale and massing.
of
service
attributes
physical
compare
acceptable,
more
generally
settings to other,
institutions such as schools.
-
Community
-
The effects of economies of scale on the
development of long-term care settings to
determine the minimum feasible size for
facilities and the potential areas for shared
services between nearby settings.
-
An examination
of the inter-relationship
between service utilization of various types
of long-term care services when all types of
This
care are available and accessible.
research could dramatically alter projections
of the need for additional nursing home beds.
Research
have
that
part
efforts
the
of
the
such
potential
long-term
community
into
attitudes
the
and
care
towards
framework
homes.
as those mentioned
for
creating
settings
support
as
nursing
such,
of
are
services
should
urban
an
an
awareness
essential
within
be
design
above
any
integrated
elements
which combine to create "good city form."
Conclusion
83
83
Bibliography
Aranyi, L., Goldman, L., Design of Long-Term Care
Facilities. NY, NY Van Nostrand Reinhold Company Inc.
1980
Arling, Greg, "Strain, Social Suppport and Distress in
Old Age." 1987 ; Journal of Gerontology, 42-1, 107-113
"Continuing Care Retirement
Branch, Laurence G.
Communities: Self-Insuring for Long Term Care." 1987
February; The Gerontologist, 27, 4-8
Nursing
Breger, William N., Pomeranz, William R.
Home Development: A Guide to Planning, Financing and
Constructing Long Term Care Facilities. New York, NY:
Van Nostrand Reinhold Company Inc. 1985
Byerts, Shirley L., "The Subjective value of the Home to
Paper presented at the Gerontological
Older People"
Society, 1981
Cantor, Marjorie H. "Life Space and Social Support."
1975; The Gerontologist, 15, 23-27
Carp, F. "Life-style and Location Within the City"
Environmental Context of Aging. Edited by Byerts,
NY, NY, Garland STPM Press: 1979
Howell & Pastalan.
Castera, M., Lund, D., Wright, S., Redburn, D.,
"Caregivers to Dementia Patients: The Utilization of
Community Services." 1987; The Gerontologist, 27,
209-214
Chellis, Robert D., Seagle Jr., J.F., Seagle, B.M.
Congregate Housing for Older People: A Solution for the
1980's, Lexington, MA: Lexington Books. 1982
Fisher, J., Bell, P., Baum, A. Environmental Psychology.
New York, NY: Holt, Reinhart and Winston. 1984
The Residential Location and
Golant, Stephan M.,
Chicago, IL: University
Elderly.
Spatial Behavior of the
of Chicago, 1972
Golant, Stephan M., "Residential Concentration of the
Future Elderly." 1975; The Gerontologist, 15, 16-23
Bibliography
Bibliography
84
84
Howell, S., Lane, T., & Friedman, S. "Determinants of
Administration on Aging,
Housing Choice."
Department of Health and Human Services, 1981.
Howell, Sandra C. Designing for Aging: Patterns of Use.
Cambridge MA: MIT Press. 1980
Koncelik, Joseph A., Designing the Open Nursing Home.
Stroudsburg, PA: Dowden, Hutchinson & Ross Inc. 1976
Lawton, M. P., Greenbaum, M., Liebowitz, B., "The
Lifespan of Housing Environments for the Aging."
1980; The Gerontologist, 20, 56-64
Lawton, M. Powell, Moss, Miriam, Grimes, Miriam,
"Changing Service Needs of Older Tenants in Planned
Housing" 1985, The Gerontologist, 258-264
Lynch, Kevin
Press 1981
Good City Form.
Cambridge, MA. MIT
Lynch, Kevin The Image of the City.
MIT Press. 1960
Cambridge, MA:
Newcomer, Robert J., "An Evaluation of Neighborhood
Service Convenience for Elderly Housing Project
Residents." Human Resourses Agency, San Diego, CA
"Six Principles for a Caring
Pastalan, Leon A.
Environment." Provider. 1986 April;Vol.12, No. 4 : 4-5
Pynoos, Jon, "Option for Mid-Upper-Income Elders"
Spring 1985, Generations: In-Depth Views on Issues in
Aging, 31-33
Regnier, Victor A., Eribes, Richard A., Hausen, Wayne
"Cognitive Mapping as a Concept for Establishing
Neighborhood Service Locations for Older People."
Paper presented at the 8th Annual ACM Urban
Symposium. 1973
Planning for the Elderly: Alternative
Regnier, Victor.
Community Analysis Techniques. The University of
1979
Southern California Press.
"The Congregate
Ruchlin, Hirsh S., Morris, J. N.
Housing Services Program: An Analysis of Service
February; The
1987
Utilization and Cost."
Gerontologist, 27, 87-91
Bibliography
Bibliography
85
85
Simon, Herbert
Cambridge, MA:
A.
The Sciences
MIT Press. 1969
of the
Artificial.
Smallegan, Marian, "There Was Nothing Else To Do:
Needs for Care before Nursing Home Admission." 1985;
The Gerontologist, Vol. 25, No. 4, 364-369
The
Snyder, L. H., Ostrander, E. R., Koncelik, J. A.,
New Nursing Home: A Response to the Behavior and Life
Style of the Aging. Conference Proceedings. Ithaca, NY.
1973
Soldo, B., Manton, K. The graying of America:
Demographic challenges for Socioeconomic Planning.
The Journal of Socio-Economic Planning Sciences, 1984.
Tierney, Joseph P., "A Comparative Examination of the
Residential Segregation of Persons 65 to 74 and Persons
75 and Above in 18 United States Metropolitan Areas
for 1970 and 1980." 1987 ; Journal of Gerontology,
42-1, 101-106.
Tobin, Sheldon S., Lieberman, Morton A. Last Home for
the Aged. San Francisco, CA: Jossey-Bass, Inc. 1976
Ullman, Steven G., "Ownership, Regulation, Quality
Assesment and Performance in the Long-Term Care
1987 Feb.; The Gerontologist, 27, 233-239
Industry."
United States Bureau of the Census- Characteristics of
Population and Housing Units, by Blocks: 1980
United States Senate, A Report of the Special Committee
on Aging. Developments in Aging: 1986
"Early
Wachtel, Tom J., Fulton, J.P., Goldfarb, J.
after
Disposition
of
Discharge
Prediction
1987 February; The Gerontologist,
Hospitalization."
27, 98-103
Weeden, Joel, "The Housing Compendium." Spring
1985, Generations: In-Depth Views on Issues in Aging,
Western Gerontological Society, 9-10
Winkelvoss, Howard E., Powell, A. V., Continuing Care
Retirement Communities: An Emperical, Financial and
Legal Analysis. Homewood IL, R. D. Irwin Inc. 1984
Bibliography
Bibliography
86
86