Assessment - Aynsley C. Brian
advertisement

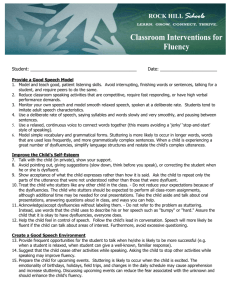
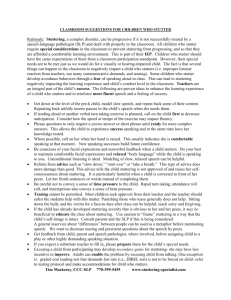
Stuttering is one of the most extensively studied yet poorly understood communicative disorders. Authorities in fluency disorders do not agree on a universal definition or on an etiology. The disagreements about causation do not significantly influence the assessment process because it is possible to validly detect and assess stuttering without knowing the etiology. HISTORY OF CLIENT: Procedures • Written case history • Information-getting interview • Information from other professionals Contributing Factors • Medical or neurological factors • Family history • Sex, motivation, and levels of concern ASSESSMENT OF FLUENCY Procedures • Screening • Speech sampling • Stimulability Analysis • Dyfluency indexes • Associated motor behaviors • Other physiological factors • Rate of speech • Feelings, Attitudes, and Reactions to Speech ORAL-FACIAL EXAMINATION HEARING ASSESSMENT DETERMING THE DIAGNOSIS PROVIDING INFORMATION Written report Interview Community resources Support Groups Important for risk factors finding triggers (ex: adult who goes in and out of fluency at different points in his life) differential diagnosis • Ex: Child with Tourette's and chronic stutterer; tick disorder—research now shows that ADD medication may worsen or trigger ticks. Screening • The most important procedure for a stuttering evaluation is a speech sample • Obtaining speech samples for more than one session and setting is recommended. Clinic/testing site Outside the assessment area Home Classroom Playground Work • Obtain the most representative sample possible Fewest dysfluencies Most dysfluencies Typical # of dysfluencies Important because it will be the primary basis on which most analyses and judgments about fluency are made Establish a positive rapport prior to collecting sample Strive for a long sample ( 200+ utterances) Alter the contexts • Conversation/ conversational starters • Narratives (for reading aloud) • Response/description of pictures (have the child describe what’s going on in picture) Avoid yes/no questions Be willing to WAIT for the client to talk Use a good quality recorder/video Preselect materials and topics that will be interesting to the client Determine • Total # of dysfluencies • Frequencies of different types of dysfluencies • Dysfluency indexes • Duration of individual instances of dysfluency • Types and frequencies of associated motor behaviors Repetitions • Part word repetitions “What t-t-t time is it?” • Whole word repetitions “What what what are you doing?” • Phrase repetitions “ I want to- I want to- I want to do it.” Prolongations • Sound/syllable prolongations “Llllllet me do it” • Silent prolongations A struggling attempt to say a word when there is no sound Interjections • Sound/syllable interjections “um….um…I had a problem this morning” • Whole word interjections “ I had a well problem this morning.” • Phrase interjections “ I had a you know problem this morning.” Silent Pauses • A silent duration within speech considered abnormal “ I was going to the (pause) store.” • Awkward sounding to a normal conversation; usually placed randomly in sentences Broken Words • A silent pause within words “ It was won(pause)derful. Incomplete Phrases • Grammatically incomplete utterances “I don’t know how to….Let us go, guys” • Complete stoppage of phrase and then moving on to something else (like circumlocution). Revisions • Changed words, ideas “ I thought I will write a letter, card” Dysfluency Indexes refer to percentages of dysfluent speech present in the speech sample. Index grids are helpful in identifying and quantifying dysfluencies Examples of Indexes • Form 9-1: The fluency Charting Grid • Form 9-2: Frequency Count for dysfluencies • Form 9-3: Calculating the Dysfluency Index Example: • When determining a dysfluency index, count each repetition of a sound, part of a word, whole word, or phrase only ONCE. ba ba ba ba ball I want I want I want a ball The total dysfluency index reflects ALL dysfluencies produced by the client. • 500 word sample: 75 repetitions 50 pauses 25 sound prolongations 150 total dysfluencies Count total number of words in speech sample (500) Count total dysfluencies (150) Total dysfluencies/total words (150/500=.30) 30% TDI Specific dysfluencies • Total # of specific dysfluencies/total # of words • Total repetitions 75/500=.15 (15%) Percentage of each dysfluency type • Total # of specific dysfluencies/total # of dysfluencies 75/150=.50 (50% of dysfluencies present were repetitions) Time each dysfluency with a stopwatch. Pauses and prolongations are the most commonly timed 10 dysfluencies resulting in a total of 42 seconds yields an average duration of 4.2 seconds Extraneous motor body movements in association with dysfluencies Usually involve parts of the oral facial mechanism: eye blinking, wrinkling of the forehead, sudden exhaustive exhaling, frowning, distorting the mouth, moving the head and quivering the nostrils. Can involve arms, hands, legs, feet or torso Form 9-4 Identify and chart the frequency of motor behaviors Respiratory Phonatory Articulatory Prosodic Note aspects if these features are present during fluent or dysfluent speech Assessing speech rate is an especially important element of the evaluation Determine what you want to evaluate: • Overall rate: • Normal rate: S-Scale: assesses stutterers’ attitudes about various speaking situations. Form 9-6 Understanding a client’s feelings and attitudes about his or her stuttering behavior may be helpful for making decisions about the client’s care. Parental Concern: • Particularly for children who stutter • Important to assess parental fears, anxieties and concerns that they have surrounding their child’s stuttering Two specific responses to negative feelings about stuttering are AVOIDANCE and EXPECTANCY Sounds Words Topics People (employer, teacher, strangers) Situations (ordering in a restaurant) Communicative Events (public speaking) Primary Avoidances • Starters • Postponements • Retrials • Circumlocutions • Antiexpectancies Secondary Avoidances • Reducing verbal output or not talking at all • Relying on others to communicate for them The expectation of the stutter before it occurs Some stutterers will push through the stutter when it occurs and others will avoid that situation Assess this by observing and listening during speech tasks and through interviews. You can “suspect” expectancy, but can only confirm this by asking the client Clinicians must use their professional judgment and experience to make an appropriate diagnosis. 1. The total dysfluency index: must be 5% or greater is usually considered a fluency disorder 2. The dysfluency indexes for repetitions, prolongations and pauses between words is 3% or greater is usually considered a fluency disorder 3. The duration of dysfluencies are 1 second or longer usually warrant a diagnosis of a fluency disorder 4. The presence of associated motor behaviors 5. The client or caregivers degree of concern about dysfluency Differentiate between children with normal dysfluency and stuttering disorders? Research shows that a child is more likely to outgrow stuttering if: • The child is a girl • The onset is fairly recent (spontaneous recovery usually happens within 12-14 months of initial onset) • The onset of stuttering occurred after the child’s 3rd birthday • The prevalence of sound/syllable or word repetitions declines quickly after onset • The child demonstrates few to no associated motor behaviors and no articulation or language problems Diagnosis of stuttering if any one of these behaviors are present: • Total % of dysfluencies is greater than 10% of all words or • • • • • • • syllables uttered. Prolongations longer than 1 second on 2% or more of the words uttered. Increases in loudness, pitch rises, and abrupt termination of prolongations are additional indicators of a fluency disorder Part-word repetitions of two or more units per repetition on more of the words uttered. Involuntary blockings or hesitations that last longer than 2 seconds Signs of struggle Noticeable emotional reactions Complaints of being unable to perform satisfactorily bc of speech Obvious variations in the frequency or severity of speech disruptions with changes in speaking situations Mild, Moderate, Severe Stuttering Severity Instrument for Children and Adults : SSI (Riley 1994) Based on four major measures: frequency, duration, concomitant behaviors and overall severity Used for all ages and yields a quick estimate for severity Rate speaker on 10 pt. scale (1 is no stutter;10 is most severe) Would it be possible for a clinician to rate an entire days worth of disfluencies? No It’s important to get parents and friends to use the rating scale for x amount of time as well. Very subjective measure—measures disfluencies over time Gives clear parameters of what to look for in each level (1-10) unlike SSI For this form, ‘Very Severe’ is stuttering on 25% or more of words. • As a clinician you would have to calculate this via language sample, a parent would just estimate. Questions for child to answer (Yes or No format) Taps into emotional based questions without directly using word stutter Be careful not to put ideas into the patients head For adults Answer questions based on avoidance, reactions, and stuttering itself Helps determine which core behaviors are more dominant