Active assisted exercises are used when
advertisement

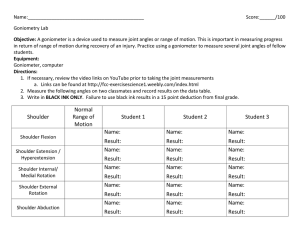
Definition: Active assistive exercises are exercises performed by the patient or with the assistance of an external force as therapist, cord & pulley, weight & pulley circuit etc… Active assisted exercises are used when: 1. The muscles acting on one of the body levers are too weak to bring about movement, or 2. The muscles are too weak to control the movement adequately. 3. For the restoration of mobility. Indications: – To assist movement in case of m. weakness. – To increase ROM. – To assist functional activities of ADL. – After removal of plaster cast. – Following tendon or m. transplantation. – As a method of muscular reeducation. Types of assistance I. Manual assistance: When the assistance is provided by a. The P.T. b. The pt’s sound limb (self assisted). II. Mechanical assistance: When the assistance is applied by mechanical tools as a. slings. b. Pulleys. c. Slings. d. Wheels, etc… Rules & principles of application 1. Starting position: Complete stability & comfort must be provided to the body to ensure complete pt’s attention, concentration & maximum effort required for performance. 2. Fixation: The proximal part of the exercised limb should be adequately fixed by the PT to improve the efficiency of the agonist muscles. 3. Support: Full support must be given to the exercised part or limb by means of: • Pillows. • Boards. • Slings. • Manually. Support → eliminate any force or load on the weak ms by counterbalancing the effects of gravity (eliminate effect of gravity). 4. Characteristics of active assistive ex: a. The assistance should be sufficient to give adequate help to the working ms, it must not be allowed to exceed this level or a passive mov. will result. b. As the m. power increases (↑), the given assistance must be decreased (↓) proportionally. 5. Direction: The assistance or external force employed is applied in the direction of m. action. 6. Repetition: Depends on the level of m. fatigue. So the cause & extent of weakness must be known & understood. Understanding the pattern of movement: Clear information must be given & understood by the patient about what is expected from him to perform. This may be taught to him by: a) Applying passive movement to the affected side or b) Active movement of the contra-lateral sound side. 8. Patient’s co-operation: * Full pt’s cooperation is essential during application of A.A. exs. * Encouragement, concentration & co-ordination are essential to achieve controlled active assisted movement. * i.e. use a mirror, palpate his/her ms as they contract will encourage him/her. I. Manual assistance 1. Self assistance When a patient has unilateral weakness or paresis, he can be taught to use his normal extremity to move the affected limb through ROM. Examples of movements: II. Shoulder flexion & extension. I. Shoulder horizontal abd. & add. II. Shoulder rotation. III. Elbow flexion & extension. IV. Forearm supination & pronation. V. Wrist flexion & extension. VI. Radial & ulnar deviation. VII. Finger flexion & extension. VIII. Thumb flexion with opposition & extension with reposition. IX. Hip & knee flexion & extension. X. Hip abd. & add. XI. Ankle & toes movs. 2. Therapist assistance: The same movements are done with the therapist assistance, but not by the therapist completely. II. Mechanical Assistive Exercises 1. Wand Exs.: a wooden stick, cane or similar objects may be used. 2. Finger Ladder: with wall climbing are tools used to assist shoulder & hand movs. 3. Cord & Pulley or Weight & Pulley Circuit: provide assistance for shoulder, elbow & wrist ROM. 4. Shoulder Wheel: provide assistance for the ULs. 5. Skate Board & Powder Board: a board is placed under the affected limb to assist : a. Isolate the effect of gravity. b. Help post surgery cases. c. After removal of plaster cast. – Suspension: the involved segment is suspended in a sling attached to a rope fixed to a point above the body segment. – Reciprocal Exercise Unit: is a device used to provide some hip & knee flex. & ext. to an involved LL by using the strength of the normal side. Wand Exercises 1. 2. 3. 4. 5. Shoulder flex & return. Shoulder hyper ext. Shoulder horizontal abd. & add. Shoulder int. rot. & ext. rot. Elbow flex. & ext. Finger Ladder Exercises 1. Shoulder flex. 2. Shoulder abd. * Precaution: The patient must be taught the proper motions & not allowed to substitute with trunk side bending, toe raising, or scapular elevation. Overhead Pulleys Pulley set up: 1. Two pulleys are attached to an overhead bar or to the ceiling approximately shoulder-width apart. 1. A rope is passed over both pulleys, & a handle is attached to each end of the rope. 2. The pt may be supine, sitting, or standing with the shoulders aligned under the pulleys. Pulley Exercises: 1. 2. 3. Shoulder flex & abd. Shoulder int. & ext. rot. Elbow flex. & ext. Shoulder Wheel Set-up: 1. A shoulder wheel is permanently attached to a wall. 2. Usually it can be adjusted to various heights & arm lengths. Shoulder wheel Exercises: 1. Sh. bd. & add. 2. Sh. flex. & ext. 3. Sh. int. & ext. rot. Skate Board & Powder Board • These devices are usually used following surgical procedures of hip to encourage ROM. • Proper instructions make them useful. • The advantages of their use encourage the pt versus telling the pt to move his leg, which often results in faulty mov. or lack of interest. Exercises: 1. 2. 3. Hip abd. & add. Hip flex. & ext. Knee flex. & ext. Suspension This technique is used to free a body part from the resistance of friction while it is moving. * The part is suspended in a sling attached to a rope that is fixed to an appropriate point above the body segment. Types of suspension: 1. Vertical suspension The point of attachment of the rope is over the center of gravity of the moving segment. The part can move like a pendulum. The mov. in a small ROM. Used for support. 1. Axial suspension The point of attachment of all ropes supporting the part is above the axis of the joint to be moved. The part will move on a flat plane parallel to the floor. Used to allow maximum mov. of a joint. Benefits of suspension for ROM exs. 1. Active participation is required, thus the pt learns to use the appropriate ms. for the desired mov. 2. Relaxation is promoted through secure support & smooth rhythmic movs. 3. Little work is required for stabilizing ms because the part is supported. 4. Modifications can be made to the system to provide grades of ex resistance. 5. After instructions, the pt can often work independently. Exercises using axial suspension: 1. Sh. abd. & add. 1. Sh. flex. & ext. 2. Hip flex. & ext. 3. Hip abd. & add. Reciprocal Exercise Unit * It uses the strength of a normal lower limb. * It is mobile, can be attached to the bed, wheelchair, or standard chair. * It improves reciprocal patterns of movs. * It improves endurance. * It initiates strengthening programs.