Transcatheter Aortic Valve
Implantation
Aortic Root Rupture
UC201403230 EE
INTERNATIONAL. CAUTION—For distribution only in markets where CoreValve has been approved. Not approved in the USA or Japan.
Non destiné au marché français. ©Medtronic, Inc. 2013. All Rights Reserved.
Background | Definition
•
The aortic root extends from the
basal plane of the valve leaflets to
the sinotubular junction, and
includes the annular plane.
•
Aortic rupture occurs when a portion
of aorta is torn, allowing blood to
exit the aortic lumen. This may lead
to a lack of blood flow to other
organs, and hemodynamic collapse.
•
Any portion of the root, including
the annulus, may be ruptured during
TAVR procedures.
Piazza et. al; Circ Cardiovasc Interv. 2008; 1: 74-81
INTERNATIONAL. CAUTION—For distribution only in markets where CoreValve has been approved. Not approved in the USA or Japan. Non destiné au marché français.
©Medtronic, Inc. 2013. All Rights Reserved.
Background | Definition
•
Aortic Root Rupture: Rare (0.5-1.0%)1,2,3, but potentially catastrophic TAVR
complication. Often leads to uncontrollable bleeding/tamponade, hemodynamic
collapse, and may lead to death if not controlled.
– Mortality for patients that experience aortic root rupture is nearly 50%4.
–
Patients must often be converted to open surgery immediately after
controlling bleeding and stabilizing hemodynamics.
• Less severe ruptures may be controlled by packing and sutures, or a second
balloon dilatation5 or valve-in-valve6 may be performed to seal the leak.
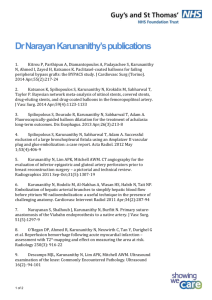
Autopsy study showing a
subannular transmural tear with a
prosthetic Sapien valve in the
aortic position (A), and left
ventricular rupture (B) after TAVI.
Transmural tears are marked with
a white vessel loop. Calcification is
noted by (1) in each image.
Haldenwang, Thorac Cardiovasc Surg; 2013; 61(5):425-7
1Pasic
et. al, Ann Thorac Surg 2010; 90: 1463-70; 2Lange et. al, Eur J Cardio-Thorac Surg 2011; 40: 1105-1113; 3Eltchaninoff et. al, Eur Heart J 2011; 32: 191-197;
et. al, Circ 2013; 128: 244-253; 5Mylotte et. al, Eurointervention 2013; 8: 1103-1109; 6Moat et. al, Eurointervention 2013; 8: 1103-1109.
4Barbanti
INTERNATIONAL. CAUTION—For distribution only in markets where CoreValve has been approved. Not approved in the USA or Japan. Non destiné au marché français.
©Medtronic, Inc. 2013. All Rights Reserved.
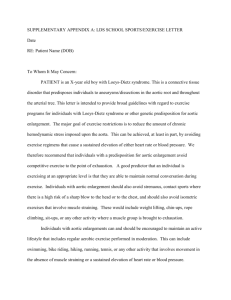
Contained and Uncontained Rupture Severity
Contained
Pseudoaneurysm of LVOT, Periaortic Hematoma
Uncontained
Cardiac Tamponade, Death
Pasic et. al, Circ Cardiovasc Interv. 2012; 5:424-432
Subban et. al, JACC Cardiovasc Int 2013; 6(6): e33-34
INTERNATIONAL. CAUTION—For distribution only in markets where CoreValve has been approved. Not approved in the USA or Japan. Non destiné au marché français.
©Medtronic, Inc. 2013. All Rights Reserved.
Background | Valve Sizing
•
Sizing goal: Transcatheter valve must be larger than annulus to establish a proper
seal, reduce PVL, and ensure anchoring, but not large enough to cause annular
injury/rupture.
•
For balloon-expandable valves, 5-15% area based oversizing is recommended1-3.
However, oversizing is also associated with increased risk of annular rupture.
•
–
If extensive oversizing is necessary, underfilling the balloon is suggested1.
–
Presence of root calcification or other anatomic modifiers may also influence sizing
choice.
For self-expandable valves, greater oversizing (perimeter or mean diameter) may
be needed to ensure adequate radial force1.
–
Multimodality imaging, including CT, is highly recommended4, but there are not
specific oversizing guidelines for self-expandable valves.
1Willson
et. al, J Cardiovasc Computed Tomography 2012; 6: 406-414
et. al, Circ Cardiovasc Interv 2012;5:540-548.
3Binder et. al, JACC 2013; 62 (5):431–8
4CoreValve Best Practices Handbook; June 2013
2Blanke
INTERNATIONAL. CAUTION—For distribution only in markets where CoreValve has been approved. Not approved in the USA or Japan. Non destiné au marché français.
©Medtronic, Inc. 2013. All Rights Reserved.
Multislice Computed Tomography (MSCT) Imaging
•
MSCT can provide a more accurate, 3D assessment of the noncircular aortic
annulus than 2D forms of imaging, such as transesophageal echocardiography
(TEE) for sizing.
–
•
The only method available for proper calcification assessment.
MSCT is the preferred imaging modality – provides the ability to make multiple
measures of the annulus, including perimeter, area, and diameter. This is
important for sizing non-circular annuli.
–
A retrospective analysis of 157 patients treated with CoreValve revealed that using MSCT
perimeter guidelines resulted in significantly reduced PVL, compared with TEE-sizing1
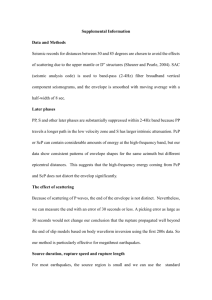
Double-oblique transverse MSCT projections of LVOT showing calcification degree
None
1Mylotte
Mild
Moderate
Barbanti et. al, Circ 2013; 128: 244-253
Severe
et. al, JACC 2013; 62(18)SB: B227. Poster abstract, TCT 2013.
INTERNATIONAL. CAUTION—For distribution only in markets where CoreValve has been approved. Not approved in the USA or Japan. Non destiné au marché français.
©Medtronic, Inc. 2013. All Rights Reserved.
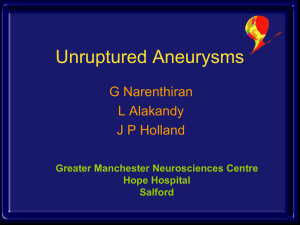
Clinical Experience | Type and Site of Rupture
•
In a survey of 31 consecutive patients who
received Sapien (n=27) or Sapien XT (n=4)
transcatheter valves, and experienced aortic
root/annular/LVOT rupture, approximately 2/3
were uncontained ruptures, and 1/3 were
contained periaortic ruptures/hematomas1.
•
Site of rupture:
•
1Barbanti
–
annulus (67.7%)
–
sinus of valsalva (16.1%)
–
LVOT (9.7%)
–
sinotubular junction (6.4%)
Predictors of Rupture: Moderate/severe
subannular or LVOT calcification and prosthesis
oversizing (> 20%).
White arrow: periaortic contrast extravasation from
aortic root rupture
Colli et. al, Eur J Cardiothoracic Surg 2011; 39:788
et. al, Circ 2013; 128: 244-253
INTERNATIONAL. CAUTION—For distribution only in markets where CoreValve has been approved. Not approved in the USA or Japan. Non destiné au marché français.
©Medtronic, Inc. 2013. All Rights Reserved.
Increased Number of Aortic Root Rupture Cases
•
Since 2010, there have been only 13 published case reports specifically on
annular/aortic root rupture1-13.
• The number of yearly case reports has increased in 2013, and may be due to:
• Increased numbers of TAVR procedures performed
• Heightened awareness/increased publication on aortic root rupture
9
Number of Patients
8
7
8
6
5
4
3
2
1
0
2
2
2011
2012
1
2010
2013
1Aminian
et. al, Cath and Cardiovasc Interventions 2013; 81:E72-E75; 2Bouabdallaoui et. al, Int. J Cardiol 2013; 16963; 3Colli et. al, Eur J Cardiothoracic Surg 2011;
39:788;
et. al, JACC Cardiovasc Int 2013; 6(4): 416-417; 5Debonnaire et. al, Eurointervention 2013; 8:1103-1109; 6Haldenwang et. al, Thorac and Cardiovasc
Surg 2013; 61(5): 425-427; 7Hayashida et. al, JACC Cardiovasc Int 2013; 6(1): 90-91; 8Himbert et. al, Eur Heart J 2010; 31(24): 2995; 9Kim et. al, Cath Cardiovasc Int
2013; epub; 10Lee et. al, Cath Cardiovasc Int 2012; epub; 11Negi et. al, Gen Thorac Cardiovasc Surg 2013; epub; 12Subban et. al, JACC Cardiovasc Int 2013; 6(6): e33-34;
13Yu et. al, J Invasive Cardiol 2013; 25(8): 409-410
4Dahdouh
INTERNATIONAL. CAUTION—For distribution only in markets where CoreValve has been approved. Not approved in the USA or Japan. Non destiné au marché français.
©Medtronic, Inc. 2013. All Rights Reserved.
Aortic Root Rupture Case Outcomes
•
While aortic root rupture is potentially fatal, approximately half of patients still
survive the event.
–
After stabilization of hemodynamics and hemorrhaging, most patients are converted to
open chest surgery for repair of the rupture and surgical replacement of the valve14,15.
–
Transcatheter valve-in-valve is also performed to stabilize these patients16.
9
Number of patients
8
7
6
5
5
Survived
4
Died
3
2
1
0
1
2010
1Aminian
2
2011
1
3
1
2012
2013
2Bouabdallaoui et.
et. al, Cath and Cardiovasc Interventions 2013; 81:E72-E75;
al, Int. J Cardiol 2013; 16963; 3Colli et. al, Eur J Cardiothoracic Surg 2011; 39:788;
5
et. al, JACC Cardiovasc Int 2013; 6(4): 416-417; Debonnaire et. al, Eurointervention 2013; 8:1103-1109; 6Haldenwang et. al, Thorac and Cardiovasc Surg 2013;
61(5): 425-427; 7Hayashida et. al, JACC Cardiovasc Int 2013; 6(1): 90-91; 8Himbert et. al, Eur Heart J 2010; 31(24): 2995; 9Kim et. al, Cath Cardiovasc Int 2013; epub; 10Lee et.
al, Cath Cardiovasc Int 2012; epub; 11Negi et. al, Gen Thorac Cardiovasc Surg 2013; epub; 12Subban et. al, JACC Cardiovasc Int 2013; 6(6): e33-34; 13Yu et. al, J Invasive Cardiol
2013; 25(8): 409-410; 14Barbanti et. al, Circ 2013; 128: 244-253; 15Pasic et. al, Ann Thorac Surg 2010; 90: 1463-70; 16Yu et. al, J Invasive Cardiol 2013; 25(8): 409-410
4Dahdouh
INTERNATIONAL. CAUTION—For distribution only in markets where CoreValve has been approved. Not approved in the USA or Japan. Non destiné au marché français.
©Medtronic, Inc. 2013. All Rights Reserved.
Pre- and Intra-Procedural Contributors to Rupture
Pre-Procedural
Small Annulus
Calcified Annulus/LVOT/Root
Intra-Procedural
Over- or post-dilatation of
prosthesis
Enhanced oval shape of
annulus in the presence of
calcification
INTERNATIONAL. CAUTION—For distribution only in markets where CoreValve has been approved. Not approved in the USA or Japan. Non destiné au marché français.
©Medtronic, Inc. 2013. All Rights Reserved.
Conclusions
• Rupture of the aortic root is a rare but
potentially catastrophic complication of
TAVR. There has been an increase in
published cases recently.
• Predictors of rupture include moderate or
severe calcification of the LVOT, root, or
annulus, as well as prosthesis oversizing.
– Accurate pre-procedural sizing and caution
with balloon post-dilatation may help in
reducing the frequency of these events.
Pasic et. al, Ann Thorac Surg 2010; 90: 1463-70
INTERNATIONAL. CAUTION—For distribution only in markets where CoreValve has been approved. Not approved in the USA or Japan. Non destiné au marché français.
©Medtronic, Inc. 2013. All Rights Reserved.