CASE PRESENTATION
advertisement

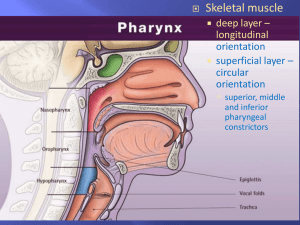
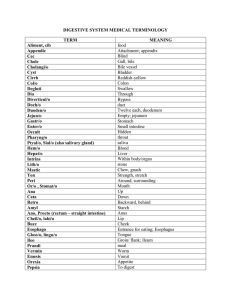
Surgical Unit 1 CASE 1 DR. SAJID MAHMOOD Name: Najma Shaheen W/O Asif Age: 30 Years Sex: Female Occupation: House Wife Address: Dhok Farman Ali Rwp. DOA: 26-12-14 MOA: Referred from MU II Presenting Complaints History of corrosive intake ….5 months back. Difficulty in swallowing………..5 months History of presenting complaints My patient had argument with her husband 5 months back following which she intentionally ingested acid Amount and nature of which is not known She had severe burning sensation in epigastrium and was brought to hospital Initial management was done. Later after 2 weeks she started having difficulty in swallowing for semi solids and solid food. Symptoms worsened over the next 02 months She was able to swallow her saliva and tolerate liquids. No history of vomiting. No H/O odynophagia, retrosternal burning pain, dyspepsia , acid or water brash. No H/O cough, choking sensation or chest pain. No H/O anorexia , she gives history of weight loss She underwent endoscopy 6 weeks after corrosive intake and lower esophageal stricture was noted, dilatation was done Symptoms were relieved temporarily. Later she had multiple sessions(10 times) of upper GI endoscopies and dilatation of esophageal stricture was attempted. However her last endoscopic dilatation was not successful. Her last endoscopy, done on 20th December 2014 ,shows : Tight stricture 30 cm from incisors Dilatation was not possible beyond 9 fr for the 4th consecutive time. She was referred to surgical department for definitive surgical management Past medical history No H/O D.M., T.B., I.H.D., H.T.N., Asthma. No past history of hospital admission. No past history of any psychiatric illness. Past surgical history History of C section 9 years back Family history No family history of psychiatric illness No family history of DM , HTN , TB, any malignancy Personal history Non smoker Non addict Normal sleep habits Drug history No H/O any drug allergy. Obstetric history 3 sons and 1 daughter Age of eldest child is 13 years Age of youngest child is 7 years Socio economic status Belongs to middle class family General physical examination A young lady of average built, lying comfortably on the bed with i/v cannula on left forearm , well oriented in time place and person. Pulse=78/min BP=100/60 Temp=A/F R/R=14/min Pallor absent Jaundice absent Cyanosis absent Clubbing absent Koilonychia absent Pedal edema absent JVP not raised Skin - normal Thyroid not enlarged No lymph nodes palpable Body weight : 48 kg Height : 156cm BMI=19.7 kg/m2 Systemic examination GASTROINTESTINAL SYSTEM Oral mucosa, teeth, gums ,tongue and palate =normal Scaphoid abdomen, moving with respiration, umbilicus central & inverted, no visible swelling, scar mark or veins. Soft, non-tender abdomen with no mass or viscera palpable and hernial orifices intact. Percussion note resonant . Bowel sounds audible. RESPIRATORY SYSTEM Normal vesicular breathing No added sounds CARDIOVASCULAR SYSTEM S1 + S2 +no added sounds CENTRAL NERVOUS SYSTEM Higher mental functions……..intact Sensory system……intact Motor system: power 5/5 on both sides reflexes normal Cranial nerves…..intact SUMMARY A 30 years female , normotensive and normoglycemic , presented to surgical floor ,being referred from mu2 after failure of endoscopic esophageal dilatation. Provisional Diagnosis Esophageal stricture secondary to corrosive intake INVESTIGATION Endoscopy findings Tight stricture 30 cm from incisors. For 4 consecutive times the dilatation not possible beyond 9 Fr. HB=11.3 g/dl WBC=3400/ul PLT=204000/ul S/Urea=28 mg/dl S/Creat=0.7mg/dl T/bilirubin=.8mg/dl S/ALT=33u/l S/ALP=186UL Serum albumin 4.5 g/ dl ECG : Normal CXR : Normal DIAGNOSIS Benign Esophageal Stricture secondary to corrosive intake. Plan Definitive surgical intervention was planned Pre-operative preparation Calculate BMI Nutritional Assessment & Diet Charting. Counseling Of Patient & Attendants about the Operative Procedure and Prognosis Pre op psychiatric consultation Availability of Bed/Vent in SICU. Informed consent. Anesthesia fitness. Arrange Blood & Blood Products. Pass CVP PROCEDURE Upper mid line abdominal incision given , abdomen opened Stomach was found to be normal left lobe of liver mobilized by cutting the coronory ligament, left gastric artery, short gastric and left gastro- epiploic arteries ligated and divided. Stomach mobilized and tube made and hinged to lower esophagus with stitch after dividing the GE junction. Feeding jejunostomy done Abdomen closed, skin closed with skin staples RIGHT THORACOTOMY Right sided thoracotomy done Per op Findings : Middle and lower esophageal stricture with very narrow lumen. Azygous vein ligated between ligatures Thoracic part of esophagus mobilized under vision Stomach pulled up through the diaphragm. Haemostasis secured Chest tube placed Thoracotomy wound closed in layers. NECK DISSECTION Neck incision given on right side Esophagogastric anastomosis done Drain placed in neck. Skin closed with skin staples. Per operative 01 RCC and 3 bags of platelets were transfused Patient was successfully extubated. Then shifted to surgical ICU for monitoring. Post op orders NPO till further order Oxygen at 4L/min via face mask. I/V fluids x TDS with K+ replacement. Inj. Omeprazole 40 mg I/V BD Inj. imipenum 1g I/V TDS Inj. Vancomycin 1 g i/v BD Epidural top up QID Esophagectomy sample for H/P Post operative course Patient had fits and Oxygen saturation dropped on first POD, was put on mechanical ventilation. Work up done for fits which showed hypocalcemia Calcium replacement done. Extubated after 12 hours Nutrition according to standard protocol was started in feeding jejunostomy. Remained in SICU for 3 days Shifted to HDU on 3rd POD Post operative course NGT and Foley catheter removed on 4th POD. Neck drain removed on 5th POD. Chest tube was removed on 8th POD after getting CXR Oral sips were allowed on 8th POD after contrast study Semi solid diet started on 9th POD Patient was discharged on 11th POD. Right thoracotomy wound Abdominal wound Neck wound Barium swallow (AP view) Lateral view CASE 2 DR AFIYA ZULFIKAR Name :Adnan Age :18 years Sex: Male Occupation: student Address :kot P/O Abbasspur Date of admission:13-01-2015 Mode of admission: ER History of corrosive intake …3 months back. Iatrogenic Esophageal perforation secondary to endoscopic dilatation....2 months back Unable to swallow…..2 months History of presenting complaints My patient had argument with his father 3 months back following which he intentionally ingested acid Amount and nature of which is not known He had severe burning sensation and was brought to hospital(HFH) Initial management was done. Later he started having difficulty in swallowing for semisolids and solid foods. Worsened over 2 next weeks Liquids well tolerated ( till esophageal perforation) No history of vomiting No h/o odynophagia, retrosternal burning pain, dyspepsia , acid or water brash No h/o cough, choking sensation, chest pain present He underwent endoscopy 2 weeks after corrosive intake and lower esophageal stricture was noted, dilatation was done Symptoms relieved temporarily Later he had 3 sessions of upper GI endoscopies and dilatation of strictured part of esophagus was attempted During the 4th session he developed iatrogenic esophageal perforation Esophageal exclusion procedure was done which consists of 1. Cervical oesophagostomy 2. Closure of oesophagogastric junction 3. Feeding jejunostomy Bilateral Chest intubation for drainage Remained admitted in SICU for 8 days Later shifted to surgical ward and was discharged in stable condition. Plan of definitive surgery was made after nutritionally building the patient Readmitted on 13 -01-2015 Complete work up done and patient was prepared for definitive surgical management Past medical history No h/o D.M., T.B., I.H.D., H.T.N., Asthma. No past history of hospital admission. No past history of any psychiatric illness. Past surgical history Not significant Family history No family history of psychiatric illness No family history of DM +HTN +TB +malignancy Personal history Non smoker Non addict Normal sleep habits Drug history No h/o any drug allergy. Socio economic status Belong to lower class family General physical examination A young male of average built sitting comfortably on the bed well oriented in time place and person with following vitals Pulse=70/min BP=120/80 Temp=A/F R/R=14/min Pallor Jaundice Cyanosis Clubbing Pedal edema -ve JVP not raised Thyroid not enlarged No lymph nodes palpable -ve -ve -ve -ve body wt =51 kg height= 160 cm BMI= 19.92 Koilonychia -ve Skin normal Systemic examination GASTROINTESTINAL SYSTEM Oral mucosa, teeth, gums ,tongue and palate =normal (Spit fistula in neck) Scaphoid abdomen, moving with respiration, umbilicus central & inverted, no visible swelling, scar mark, or veins. Soft, non-tender abdomen with no mass or viscera palpable and hernial orifices intact. Percussion note resonant Bowel sounds audible RESPIRATORY SYSTEM Normal vesicular breathing No added sounds CARDIOVASCULAR SYSTEM S1 + S2 +no added sounds CENTRAL NERVOUS SYSTEM Higher mental Functions……..intact Sensory system……intact Motor system: power 5/5 on both sides reflexes normal Cranial nerves…..intact summary 18years male having esophageal exclusion done after iatrogenic esophageal perforation. Now admitted for definitive surgical management investigations WBC : 9.4/ul Hb : 14.9mg/dl Plt : 253/ul Urea: 46mg/dl s/creat :1.4 mg/dl S/E : WNL S/Albumin : 4.1g/dl CXR : N ECG : N Pre operative preparation Calculate BMI Nutritional Assessment & Diet Charting. Counseling Of Patient & Attendants about the Operative Procedure and Prognosis Pre op psychiatric consultation Availability of Bed/Vent in SICU. Informed consent. Anesthesia fitness. Arrange Blood & Blood Products. Pass CVP Operation Mckeown esophagectomy Per op findings Inflammed middle and lower esophagus Normal stomach Post op orders NPO till further order I/V fluids x TDS with K+ replacement. Inj Omeprazole 40 mg I/V BD Inj . imipenum 1g I/V TDS Inj. vancomycin 1 g i/v BD Epidural top up QID Esophagectomy sample for H/P Post operative course Shifted to ICU Remained on ventilatory support for 1day Extubated after 24 hours Nutrition started in feeding jejunostomy according to standard protocol Remained in SICU for 3 days Shifted to HDU on 3rd POD Post operative course NGT and Foley catheter removed on 4th POD. Neck drain removed on 5th POD. Chest tube removed on 7th post op day Oral sips allowed on 8th POD after getting CXR Discharged on 13th POD Right thoracotomy wound Abdominal wound Neck wound Barium swallow CORROSIVE INTAKE DR GOHAR RASHEED AP SU1 OBJECTIVES Mechanism of injury Initial management Later management Surgical management TYPES OF CORROSIVES Typically Acids or Alkali. Alkali dissolve tissue thus penetrate more and result in perforation. Acids cause coagulative necrosis that limit there penetration and present with more strictures. Causes severe injury to mouth , pharynx, esophagus and stomach. Phases of injury 3 phases Acute necrotic phase (1-4 days) coagulation of intracellular protein >cell necrosis> surrounding tissue inflammation Ulceration +granulation phase (3-5days)necrotic tissue slough leaving ulcerated base + granulation tissue Phase of cicatrization and scarring (10-12) previously formed connective tissue begins to contract resulting in narrowing of esophagus It is during this phase efforts should be made to reduce stricture formation(PPI+H2 blockers) Outcomes Of Corrosive Intake: Depends upon… Caustic properties. Amount, concentration and physical form. Duration of contact. Clinical Presentation: Larynx & Pharynx Esophagus Stomach Perforation Stridor Dysphagia Epigastric Pain Hypotension Hoarseness Odynophagia Hematemesis Fever Chest Pain Laryngitis ------ ------- Peritonitis ALGORITHM ENDOSCOPIC VIEWS OF CORROSIVE INJURY Indications For Emergency Surgery: Signs of Perforation. Peritonitis Extra visceral air. Mediastinitis. Patients with complex/multiple perforations and widespread necrosis may require extensive debridement, esophagectomy or even esophagogastrectomy. With more devastatiing injuries burns can be found in bowel distal to stomach. Adjacent organs like Transverse Colon, Liver, Pancreas and Spleen. These injuries have high mortality. Late Complications: Stricture Formation. • Peak incidence 02 months. • Occurs as early as two weeks or as late as years after ingestion. • Barium swallow examination is useful in evaluation. Gastric Outlet Obstruction. • Takes about 05-06 weeks up to several years. • Usually acid ingestion. Late Complications: Esophageal Carcinoma. 3% have history of caustic ingestion. • Begin 15-20 years after ingestion. Stricture due to corrosive intake increases the risk of esophageal CA by 1000 times in 10-25 years more than normal population* Gastric Carcinoma Rare occurrence. Tracheo-esophageal Fistula: *Update on diagnosis and treatment of caustic ingestion, Michael Lupa, Jacqueline Management Of Benign Esophageal stricture: • Strictures caused by caustic ingestion are often complex (>2cm long, tortuous or diameter precludes the passage of endoscope). Complex stricture is more difficult to treat and tend to recur. Refractory strictures : Recur in 2-4days or require more than 7-10 dilatations Balloon or Bougie dilatation. No data to support the superiority of one over the other. Stents. (intraluminal self expandable plastic stents), an option in refractory stricture. Goal is to hold the stricture open for a prolonged time allowing tissue to remodel before removing the stent Indications of Surgical Interventions Complete stenosis in which all attempts have failed to establish patent lumen Marked irregularity and pocketing on barium swallow Inability to dilate or maintain the lumen above 40 Fr bougie Development of severe peri-esophageal reaction or mediastinitis with dilatation Fistula Formation Patient who is unwilling or unable to prolong period of dilation SURGICAL MANAGEMENT OF STRICTURE ESOPHAGUS Damaged and strictured esophagus may be left in place but it constitutes increased risk of malignancy and gastro esophageal reflux. Peri esophageal inflammation may cause formation of abscess years later. But at the same time surgical dissection of the scarred esophagus may be difficult and technically demanding due to adhesions with surrounding structures. COMPONENTS OF SURGERY Mainly Comprises of two steps Resection of the Damaged esophagus/ Stomach. Reconstruction via stomach , colon , jejunum IVOR LEWIS ESOPHAGECTOMY Surgical lnterventions: Distal esophagectomy and primary esophagogastric anastomosis in the chest. Subtotal esophagectomy with gastroesophageal anastomosis in neck. Esophagectomy + gastrectomy and colonic interposition graft. Esophagectomy + Jejunal free graft with microvascular anastomosis. Esophageal Reconstruction: No replacement organ that is able to mimic the function of a healthy esophagus. All suffer from lack of effective peristalsis & the absence of a physiologic barrier to reflux. Esophageal replacement organ permits most patients to eat satisfactorily. Swallowing significantly improved in patients with severe strictures Stomach--Most Common Esophageal Substitute. Advantages: Stomach can be mobilized with relative speed & ease. Need for only one anastomosis. Generally reliable good blood supply through the Rt. Gastroepiploic arcade along the greater curvature Disadvantages: Relative ischemia at tip of the fundus. Leak and stricture rate of cervical esophagogastric anastomosis can be as high as 30%. Long term presence of acid secreting gastric mucosa can lead to complications of reflux. Tumors near GE junction, use of stomach may compromise the oncologic resection Stomach Tube The stomach is the conduit of choice because of ease in mobilization and its ample vascular supply Colon As Esophageal Substitute: Advantages: Excellent oncologic resection of tumors near GE junction. Acid resistant, by virtue of its long length prevents reflux. Excellent blood supply, tip of colon graft well perfused Stricture rate significantly reduced Disadvantages: Colon interposition is difficult to mobilize. Three anastomosis rather than one. Takes longer time in operating room Results. Mortality: 5 – 10% Leak rate: 4 -15% Early function satisfactory. Long-term function very good Jejunal Grafts: More suitable for limited esophageal replacement. Long Roux-en-Y limbs are useful to reconstruct alimentary tract following gastrectomy & distal esophagectomy. Free grafts are used to bridge gaps either between the esophagus itself or between esophagus & another conduit such as stomach or colon. Advantages: Peristaltic tube No acid/alkaline reflux (Roux–en-Y). Free graft Disadvantage: Limited length. Size. THANK YOU