H 2 O 2
advertisement

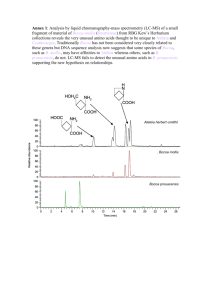
IV: Mitochondrial Function (cont’d). HEPATIC DETOXIFICATION OF a) monoamines, alcohol, toluene b) dietary or endogenous purines (meat), heme (red meat) & bilirubin, 1 a) Detoxification of monoamines catalysed by mitochondrial outer membrane MAO e.g., dopamine norepinephrine tyramine phenethylamine octylamine serotonin outer membrane MONOAMINE OXIDASE R-CHNH2 Flavin-containing amine oxidase R-CH=NH (imine) O2 H2O2 NAD+ NADH R-CHO aldehyde dehydrogenase inner membrane NH3 ATP, HCO3urea cycle UREA R-COOH b-oxidation CO2 2 Amine specificity for the two isoforms (A & B) in humans MAO A preferentially metabolizes serotonin. MAO B preferentially metabolizes phenethylamine, dopamine. MAO inhibitor + dietary amines or proprietary drugs MAOB inhibitor deprenyl (selegiline) similar to phenethylamine and increases brain dopamine levels. This is used to treat Parkinson’s disease. But “Hypertensive crisis” is a hyperadrenergic state induced by MAO inhibitors + pressor amines (e.g., tyramine in cheese,beer,wine or soya sauce) or proprietary drugs (e.g., L-DOPA, mazindol, ephedrine, etc). Cheese Cheese Tyramine (mg/g) Tyramine (mg/g) Cheddar cheese, old 1530 English Stilton 1157 Beer 2-11 Blue 998 Sherry Wine 3 Mozzarella 158 Chianti Wine 25 Feta 76 Processed cheese slice nil Perry, 1996. http://www.vh.org/adult/provider/psychiatry/CPS/19.html 3 b) Detoxification of alcohols by matrix ALDH2 Covalently binds to protein-NH2 (ADH) ETHANOL cytosolic alcohol dehydrogenase NADH Methyl pyrazole acetaldehyde ANTABUSE (disulfiram) or cyanamide NAD+ NAD+ aldehyde dehydrogenase (ALDH) NADH acetate ADH Chromosome # 4 Caucasians 99% normal ALDH 9, 12, 17 90% normal Japanese 40% deficient 90% atypicial ATP CoASH CO2 TCA cycle acetylCoA Suscept. to alcoholism Appearance social drinking 10% (>) < 10% -flushing 4 c) Benzoic acidosis induced by toluene glue sniffing Toluene Benzaldehyde Benzyl alcohol ADH Cyt P-450 CH3 CH2OH ER CHO CYTOSOL ALDH1/ ALDH2 MITOCHONDRIA COOH URINE CONHCH2COOH Benzoic acid ATP CoA Hippuric acid Benzoyl-CoA synthetase Benzoyl-CoA glycine Teratogen Update: Toluene teratology. 55, 145-51, (1997) 5 8. Hemoprotein toxicity diseases caused by heme or bilirubin A) Rhabdomyolysis (drug induced) releases myoglobin and heme and causes kidney mitochondrial damage B) Kernicterus:- bilirubin causes neonatal brain mitochondrial damage 6 A) Myoglobin mediated rhabdomyolysis rarely caused by statins STATIN Drug BAYCOL withdrawn by BAYER, 2001 Muscle Cell Drug reactive metabolites Mitochondrial/cytotoxicity Myoglobin release Massive muscle breakdown CRUSH INJURY Or if LAIN IMMOBILE for hrs (e.g. EtOH, heat stroke) a) x10 creatine phosphokinase b) Dark brown granular casts in urine Acid Mb Fe accumulates in kidney renal tubule Acid lipid peroxidation (proximal tubule) mitochondrial toxicity KIDNEY Failure (7% of all cases of acute renal failure) Spontaneous myalgias Muscle tenderness, Weakness, malaise, fever DEATH THERAPY 1.) NaHCO3 base 2.) Desferoxamine CMAJ 165(5) pg 632 (2001); J. Biol. Chem. 273, 31731-7 (1998) 7 B) Hemoglobin/heme mediated brain damage ie. Kernicterus (brain damage caused by bilirubin in the newborn (hyperbilirubinemia)) • re-emergence (due to shorter hospital time, breastfeeding) • danger signs onset of jaundice 3 days following birth, vomiting, lethargy, poor feeding, fever, high pitched crying. • plasma bilirubin > 340 uM = exchange transfusion therapy plasma bilirubin > 240 uM = Phototherapy (blue light) Drug therapy Sn protoporphyrin (inhibits heme oxygenase). Hemoglobin Heme oxygenase of reticuloendothelial cells of spleen, liver, kidney • Bilirubin Glucuronyl Transferase Appears at 7d after birth binds to serum albumin released by competing fatty acids or drugs bilirubin brain mitochondrial toxicity (hearing loss? brain damage encephalopathy) Glucuronide conjugated bilirubin. • 0.3% mortality (yellow staining of brain) • family history, hemolytic diseases, Gilbert’s disease, diabetes (erythrocyte fragility), 8 G6PD deficiency (Pediatrics 106, 1478-80 (2000), sickle cell. Metabolic pathway of heme degradation to bilirubin and detoxification of bilirubin by glucuronidation. (M=methyl,V=vinyl and P=propionate represent heme side chains Fe2+ CO Heme Oxygenase NADPH: P450 Reductase NADPH O2 NADP+ NADPH NADP+ H2O NADPH NADPH Biliverdin Reductase NADP+ UDP UDP-glucuronic acid UDP-glucuronosyl transferase JAUNDICE Antioxidant, but at high concn. TOXIC TO NEONATAL BRAIN MITOCHONDRIA 9 9. HEME BIOSYNTHESIS BY MITOCHONDRIA AND GENETIC DISEASES A) Heme biosynthesis for cytochromes, etc. B) Genetic diseases: Porphyrias and porphyrin toxicity C) Oxidative degradation of heme to bilirubin 10 A) HEME BIOSYNTHESIS and porphyria diseases 11 Cytochrome Heme Synthesis - Overall picture 12 Heme synthesis • Heme required for synthesis of mitochondrial cytochromes and endoplasmic reticular P450s. • Heme required for bone marrow synthesis of hemoglobin and muscle myoglobin • STEP 1 for heme synthesis is the synthesis of aminolevulinic acid (ALA) from succinyl CoA of the citric acid cycle and glycine 13 Heme biosynthesis in bone marrow (hemoglobin) and liver (cytochromes) ALA SYNTHESIS AND TOXICITY Mitochondrial Matrix H+ NH COO 2 COO + CH2 CH2 C R.L.S. ALA synthetase CH2 CoA pyridoxal CH2 C Glycine Succinyl CoA succinate 1 Feedback inhibition by heme (also induces heme oxygenase) O citric acid cycle COO CH2 COO S CO2 + CoA O Aminolevulinate (ALA) CO2 + CoA -ketoglutarate dehydrogenase complex Fe, O2 NH4+, O 2 ROS DNA strand breaks -ketoglutarate Therefore ANAPLEROTIC reaction required to replace succinyl CoA in citric acid cycle. C NH3 H2 COO CH2 DNA ADDUCTS LIVER CANCER CH2 C C H ALA synthetase induced by: 1) Heme deficiency due to excess P450 synthesis/induction e.g., by barbiturates Sulfonamides: Therefore an increase in urine porphyrins 2) ERYTHROPOIETIN (formed by kidneys) improves quality of life of patients on kidney dialysis. 3) Acute intermittent porphyria or ALA dehydratase deficiency. or lead 4) LEAD HEME BIOSYNTHESIS STEP II (CYTOSOL) ALA accumulates a) Acute intermittent porphyria b) Lead ALA toxicity 1) Brain Neuropsychiatric problems in acute porphyria, 2) Liver necrosis / cancer particularly if Fe overload Therapy 1) HEME arginate 2) High carbohydrate glucose-6-P O H2O2 NADPH GSH reductase GSH peroxidase O Arch Biochem Biophys. 373, 368-74, (2000) 4,5-dioxovaleric acid (DOVA) 14 Erythropoietin synthesised by kidney induces hemoglobin synthesis in bone marrow (replaces blood transfusion!) 15 Heme Biosynthesis - STEP 2 in the cytosol (4 enzymes 2-5) COOH LIVER/BONE MARROW cyto sol COOH COOH HOOC Cutaneous Porphyria Porphyria Cutanea Tarda HN NH coproporphyrinogen I non-e nzymatic * Acute Porphyria HN NH Hydroxymethyl bilane 5 HOOC COOH COOH COOH HOOC CYP1A2 COOH COOH HOOC Uroporphyrinogen I HN NH P A Symmetrical HO A P NH HN N HN HN NH HOOC COOH HOOC 3 COOH 4 Acute phosp hobilinogen Interm ittent deamin ase Porphyria* NH HOOC COOH P COOH HOOC Congenital Erythropoietic Porphyria A A COOH Uroporp hyrinogen III s ynthas e NH HN NH HN CYP1A2 P Uroporphyrin (UROPORPHYRIA) HOOC COOH NH2 HOOC HOOC Porphobilinogen (PBG) 2 Uroporphoryrinogen decarboxylase COOH Porphyria Cutanea Tarda COOH ALA Dehydratase Deficiency PBG Porphryia * SYNT HASE r.l.s polymorphism -4CO2 COOH NH HN STEP 3 COOH NH STEP 1 1 5 HN O H2N ALA COOH COOH Coproporphyrinogen III 16 Heme Biosynthesis - STEP 3 - mitochondrial final steps (3 enzymes) COOH Acu t e Po rp h y ria * Cu tan eo u s Po rp h y ria COOH STEP 2 NH HN NH HN Hered itary 6 Co p ro p o rp h y ria * O2 CO2 Cop roporph yrinog en oxidase COOH COOH Cop roporph yrinog en III m ito ch o n d ria l in term em b ra n e sp a ce Varieg ate Po rp h y ria * Pro t o p o rp h y ria 8 7 N N Fe N Fe2+ NH N N HN COOH HEME NH O2 i.m. r.l.s COOH HN Pro t o p o rp h y rin o g en o x id ase Ferro ch elatase N NH HN i.m. COOH COOH Protoporph yrin IX COOH COOH Protoporph yrinogen IX MITOCHONDRIA 17 B) PORPHYRIAS I. Enzymes Inhibitors causing porphyria II. Genetic porphyrias 18 I. ENZYME INHIBITORS CAUSING PORPHYRIA PORPHYRIA - Greek “porphyros” (purple urine) an over-production disease. Often neuropsychiatric (syphilis much more so). 2) ALA dehydratase - lead 5) Uro’gen decarboxylase - PCBs, dioxin, lead, cadmium, hexachlorobenzene (fungicide - seeds). Mitochondrial oxidase - steroids (birth control pills) and estrogens 8) Ferrochelatase – lead II. GENETIC PORPHYRIAS (Emerg Med Clin.N Am 23 (2005)885-899) 2) ALAD deficiency porphyria (Seminars in Liver Disease, 18, 95-101, 1998) excrete ALA not PBG, symptoms like (neurological). 19 Scriber et al. (eds). Metabolic and molecular basis of inherited disease. 7th ed. 1995, p.2124. 20 3) Acute intermittent porphyria (i.e. phosphobilinogenin deaminase deficiency) excrete ALA and PBG , the most common hepatic porphyria)- MEDALERT bracelet 1. Symptoms - excrete PBG and ALA in the urine , high plasma PBG/ALA - severe abdominal pain, nausea, vomiting, hypertension(cardiovascular) then CNS - anxiety, insomnia, confusion, hallucination, paranoia then peripheral neuropathy - fatal respiratory paralysis. Liver cancer. 2. a. PBG deaminase deficiency - gene locus 11q24 (>100 mutations), autosomal dominant 1:10,000-50,000 but 1:1000 in N. Sweden (Lapland) b. Precipitated by phenytoin, phenobarbital drugs, alcohol, fasting, hormones estrogen, stress, infection or lead poisoning 3. Biochemistry of neurotoxicity a. heme deficiency P450 drug metabolism tryptophan dioxygenase brain tryptophan brain serotonin mitochondrial cytochromes (mitoch.disease) b. ALA “ROS”, mitochondrial DNA damage. 4. Therapy –ALA with heme arginate (taken up by liver not b.m.), high glucose 5. Mouse model (PBG knockout) - called Vincent! - behavioural studies Suspects - Van Gogh, King George III(?) (Absinthe for insomnia) 6.Diagnosis :- Patients urine exposure to sunlight (reddish brown fluorescence) 21 4) Congenital erythropoietic porphyria (Erythroid, Photosensitive) -Fe overload of b.m., uroporphyrin overload of skin and erythrocytes hemolysis 1. Symptoms: skin lesions (light) , risk of infection in early infancy Anemia (hemolysis) Teeth reddish brown (fluorescence) 2. Uroporphyrinogen III synthase deficiency • Uroporphyrinogen I and coproporphyrin I accumulation in the skin, bone marrow, erythrocytes, urine, plasma 3. Treatment: activated charcoal (oral); b.m. transplant; gene therapy for bone marrow; blood transfusion to stop erythropoiesis in b.m. 4. Only 200 diagnosed so far; werewolf, vampires (early childhood sensitive to light skin blisters, infection disfigures) is not porphyria 22 5) Porphyria Cutanea Tarda - “heme deficiency and uroporphyrin overload of liver” (Photosensitive; commonest porphyria;readily treated). 1. Symptoms: lesions on backs of hands and face due to photosensitization by uroporphyrin I, III or uroporphyrinogen. Abdominal pain, neural,psychiatric. ALA,porphobilinogen. 2a. Diagnosis :- urinary uroporphyrin >> coproporphyrin. b. Uroporphyrinogen decarboxylase deficiency (liver but also erythrocyte in type II): or hexachlorobenzene or dioxin induced CYP 1A2. (Turkey bread disaster). Also Fe uroporphyrinogen III synthase - uroporphyrin I. c. Candidate hemochromatosis gene leads to diagnosis of hemochromatosis 3. Precip. by alcohol, hepatitis C virus, estrogen (birth control, post-menopause, prostate, pregnancy), Fe. 4. Biochemistry - inactivation of decarboxylase (-SH enzyme) by “ROS” from reduced P450/P450 reductase/Fe 5. Therapy:- Fe removal (phlebotomy or desferoxamine and ascorbic acid) - chloroquine endocytosis and releases uroporphyrin chloroquine complex from hepatocytes - heme? 23 6) Hereditary Coproporphyria - coproporphyrinogen oxidase deficient, chronic fatigue syndrome. - hepatic porphyria Symptoms: liver cancer 7) Porphyria variegata - protoporphyrinogen oxidase 50% deficient. – hepatic and skin porphyria Gene locus 1q2320. 20,000 S. Africans descended from a Dutch lady in 1688 who went to S. African for marriage to another Dutch settler . Now 3/1000 S.Africans have this! Symptoms: skin and acute porphyria if exposed to sunlight,neurovisceral symptoms (abdominal pain),liver cancer Diagnosis :- plasma fluoresces when exposed to UV. Precipitated by sunlight Treatment: increase ALA synthetase by heme arginate, glucose ( NADPH) ? 24 8) Erythropoietic protoporphyria - associated with liver cancer, red urine “porphyrin and Fe overload disease” “Skin photosensitive” a. Ferrochelatase decreased 75-90% b. Symptoms: photosensitive skin (infancy),velvet knuckles, black liver c. Biochemistry - protoporphyrin IX accumulates in erythrocyte membranes and liver; intramitochondrial Fe accumulates in bone marrow - skin photosensitivity results from protoporphyria IX effluxing erythrocytes into plasma. d. Treatment – topical sunscreens and oral beta-carotene (ROS scav.?) e. Diagnosis –incr. protoporphyrin in erythrocytes,plasma,bile,feces I. Liver transplant; operation is difficult as operating room must be kept dark (only yellow acetate filters) II. Abdominal burns; transfused blood is destroyed as blood difficult to store. 25 C) OXIDATIVE DEGRADATION OF HEME TO BILIRUBIN (a brain neurotoxin in babies) 26 Detoxification function of the liver a) heme toxin oxidation to bilirubin b) detoxification of bilirubin by glucuronidation or albumin albumin LIVER CO phagosome Heme oxygenase 27 Degradation of heme STAGE 1 Hemoglobin of old erythrocyte trapped in spleen HEME O2 + NADPH Heme oxygenase (ER) H2O + NADP+ exhaled Fe3+ CO Bone marrow transferrin M O V M C H N H P P C H N M C H N H V M O N H Excreted by Reptiles and birds Biliverdin H2O soluble NADPH + H+ Biliverdin Reductase Modified from Fig. 28-31 Stryer 4th Ed. NADP+ M O M V N H C H Fat soluble P P N H C H2 M M N H C H V N H O BILIRUBIN (Neurotoxin to babies) ANTIOXIDANT NEONATAL JAUNDICE Bilirubin accumulates in newborns. (destroy with sunlight). Plasma Serum Albumin Complex LIVER 28 STAGE II - ligandin in hepatocyte surface membrane traps bilirubin from plasma and helps transport it into the liver where it is glucuronidated Albumin - bilirubin (a GSH transferase) 29 COO COO COO M M V M M V O H + O N H C H C H2 N H C H N H OH UDP H Bilirubin OH UDP-glucuronate UDP Endoplasmic reticulum UDP-glucuronosyl transferase (UGT 1A1*) COO O H H *mutated gene in Gaucher’s disease (carried by 15% of population) H OH O OH H OH M O H OH O N H H C COO M V N H O C H M M N H C H2 N H C H V N H O BILIRUBIN MONOGLUCURONIDE UDP gluc. + UGT 1A1 BILIRUBIN DIGLUCURONIDE (Soluble bilirubin diglucuronide secreted into the bile) 30 Mitochondrial Function (Con’t). 10. a) N-Catabolism of Amino Acids (The Urea Cycle) and the Detoxification of Ammonia (very toxic) b) N-Catabolism of Purines • reperfusion injury and drug therapy • Genetic diseases: HGPRT • Gout, Lesch-Nyhan syndrome 31 Disposal of nitrogen by mitochondria a) Cytosol The urea cycle: Detoxification of NH3 (note: urea cycle enzyme in blue) citrulline + aspartate ALANINE -ketoglutarate synthetase arginosuccinate argininos uccinase aspartate aminotransferase Alanine aminotransferase oxaloacetate Pyruvate malate malate dehydrogenase UREA ornithine Pi phospho-enol-pyruvate INNER MITOCHONDRIAL MEMBRANE Pyruvate oxaloacetate transporter transporter malate NAD+ glutamate Alanine aminotransferase H2O arginas e fumarase glutamate H+ arginine + fumarate glutamate dehydrogenase -ketoglutarate NADH citrulline ornithine tr ans carbamoylas e Alanine NH3 carbamoyl phosphate ornithine 2 ATP Mitochondrial Matrix + HCO 3 - CO2 carbamoyl phosphate synthetase 32 Mitochondrial Function (Con’t). Formation of urea from amino acids transaminase dehydrogenase Urea cycle dehydrogenase Glutamate -ketoglutarate 33 IV: Peroxisomes Function • β-oxidation of fatty acids but oxidase forms H2O2 • Glyceraldehyde is metabolised to D-glycerate and glucose via glycolate (glycolate oxidase forms H2O2 and glyoxylate) • Catalase detoxifies H2O2 to form oxygen and H2O and cooxidises other substrates, including phenols, formic acid, formaldehyde, and methanol. • Glyoxylate detoxified by peroxisomal alanine:glyoxylate transaminase to form glycine & pyruvate. Otherwise glyoxylate would be oxidised by lactate dehydrogenase to oxalic acid which causes oxalate stone formation & kidney damage. • Biosynthesis of bile acids and ether phospholipids 34 V: CYTOSOLIC FRACTION N-catabolism of purines Glycogen synthesis and glycogenolysis 35 Disposal of nitrogen (Con’t): b) N-catabolism of purines in the cytosol & peroxisomes HGPRT + PRPP HGPRT + PRPP Voet pg. 714. 36 Cytosolic Fraction 1) N-catabolism of purines can be lethal Reperfusion Injury e.g. Myocardial infarction or Paraplegia a) ISCHEMIC STAGE • Lack of O2no ATP synthesis by heart muscle mitochondria. ADPAMPhypoxanthine accumulates and leaves muscle cell to enter endothelial cell. • Acidosis causes endothelial cell xanthine dehydrogenasexanthine oxidase • Acidosis results from marked increase in glycolysis to form ATP + lactic acid (to keep cells alive by maintaining ATP levels) b) Reperfusion of O2 • O2 is the substrate for xanthine oxidase Accumulated xanthine and hypoxanthine Xanthine oxidase O2 (Endothelial cell) •Damaged endothelial and muscle cells (ischemic toxicity) release factors which recruit neutrophils (inflammatory reaction activated NADPH oxidaseO2*-. 37 Drugs which prevent reperfusion injury 1) Allopurinol – inhibitor of xanthine oxidase 2) Desferal – Complexes Fe2+ 3) Antioxidants e.g. Lazeroids (upjohn) to prevent membrane lipid peroxidation 4) Removal of H2O2 by NADPH (e.g. glucose) or GSH (e.g. methionine) or dietary Se. H2O2 OH Catalase (activated by NADPH) H 2O GSH Peroxidase GSSG + H2O 2 GSH 5) Anti-inflammatory drugs (e.g. indomethacin or phenylbutazone) 6) Ca2+ Blockers 38 Treatment or to prevent Ischemic damage (reperfusion injury) OH OH C N C C N CH HC C N H H N Y P T h e a d m C C N X A N A T H C C X N HC N O OH L H IL a n t i n C N O N N h HO P E U R I N O L A C e C N L H C L O N x i d a s N O X A N ( T o H x I y s y n t h e s i s o f u r a t e f r o m i n i s t r a t i o n o f a l l o p u r i n 39 2) Purine catabolism can be painful and cause joint damage • • • • Figure 22.22 (Voet) – By James Gilroy Defects in excretion of uric acid and/or partial deficiency in HGPRT activity due to mutation in HGPRT gene Uric acid precipitation in joints – crystals activate leukocytes H2O2 and O2*- arthritis. Adults (0.55%) in males Often suffered by over-achieving males with too much drive and ambition (e.g. pharmacists). Drugs which trigger gout • Anticancer drug treatment of acute leukemia resulting in destruction of nucleic acids and accumulation of uric acid. • Long term diuretic treatment (impair glomerular filtration) Risk Factors • Eating too much meat (purines e.g. xanthine) • Alcohol ingestion increases hypoxanthine 40 • age, male gender, high body mass index, hypertension. Cytosolic Fraction 3) Genetic Deficiency of HGPRT LESCH-NYHAN SYNDROME – X-linked recessive (X-chromosome gene) 50% of cells have a complete deficiency of salvage enzyme HGPRT (Hypoxanthine – guanine phosphoribosyl transferase) or lyase (ASLI) which catalyses: synthetase adenylsuccinate HGPRT Hypoxanthine + PRPP Guanine + PRPP Lyase(ASLI) PPi + IMP PPi + GMP XMP adenosine AMP Nucleotide synthesis Results in enormous overproduction of PRPP,hypoxanthine,uric acid. PRPP (5-phosphoribosyl-a-pyrophosphate) ATP Ribose-5-phosphate ADP 2 P3 O O CH 2 H Pyrophosphokinase H H O H O OH OH O P O O O P O O 41 Children with LESCH-NYHAN SYNDROME (Incidence 1:380,000) (HGRPT deficiency) Children • Neurological dysfunctions ( serotonin metabolism) • Aggressive or self mutilating but affectionate, quick to laugh, likeable and open. • Tend to chew their lips and finger tips • Mental retardation • Cerebral palsy and spasticity • Obscene gestures • Flinging their feces • Die before reaching the age of 10 due to renal failure. • If mild enough, gout will develop into adulthood. 42 DRUG THERAPY ALLOPURINOL is the most useful drug for treatment of GOUT. Inhibition of uric acid production because xanthine oxidase (terminal step to uric acid production) is inactivated by allopurinol. However, neurological problems associated with LESCH-NYHAN SYNDROME which have been attributed to PRPP and de novo purine synthesis can not be alleviated by allopurinol. Allopurinol will prevent uric acid stones accumulating in the kidney and will prevent kidney infections and hematuria. NEUROLOGICAL TOXIC MECHANISM UNKNOWN HGPRT, which is required for purine synthesis is still functionally deficient and PRPP accumulates.Dopamine neuron function is still lost and neurological problems persist. 43 The End • Don’t memorize 9, 21, 31, 33, 35, 37, 43 44