MLAB 2401: Clinical Chemistry Keri Brophy
advertisement

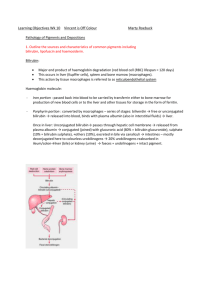
MLAB 2401: Clinical Chemistry Keri Brophy-Martinez Assessment of Liver Function Liver Panel • • • • • • Albumin Bilirubin, total Bilirubin, direct AST/SGOT ALT/SGPT Alkaline Phosphatase History of Bilirubin Analysis • Ehrlich(1883) – Described the reaction of bilirubin with diazotized sulfanilic acid= DIAZO REACTION • Malloy and Evelyn (1937) – Diazo reaction with 50% methanol as an accelerator • Jendrassik and Grof ( 1938) – Diazo reaction with caffeine-benzoate-acetate as accelerator – Increased sensitivity Measured vs. Calculated • Measured Analytes – Total Bilirubin – Conjugated bilirubin (DIRECT) • Calculated Analytes – Unconjugated bilirubin (INDIRECT) Fractions & Their Characteristics • Conjugated/Direct – Polar – Water-soluble – Found in plasma, unbound or free – Reacts with diazotized sulfanilic acid without an accelerator • Unconjugated/Indirect – Nonpolar – Water-insoluble – Found in plasma, bound to albumin – Reacts with diazotized sulfanilic acid with an accelerator • Delta – Conjugated bilirubin bound to albumin – Observed in hepatic obstructions Specimen Collection and Storage • Serum or plasma preferred • Temperature sensitive • Fasting sample preferred – Lipemia increases bilirubin concentrations • No hemolysis – Hemolysis decreases the reaction of bilirubin with the diazo reagent • Light sensitive – Bilirubin levels decrease by 30-50% per hour. Methods of Bilirubin Analysis • Jendrassik-Grof – Measures Total and Conjugated bilirubin – Principle • Bilirubin pigments in serum react with a diazo reagent which results in the production of azobilirubin( a purple product). Measured at 540 nm. • Caffeine -benzoate accerlerates the coupling of bilirubin with the diazo reagent. • Ascorbic acid stops the reaction. • Alkaline tartrate converts the purple azobilirubin to a blue azobilirubin. • This product is measured spectrophotometrically @ 600 nm. Jendrassik-Grof • Advantages – Not affected by pH changes – Maintains optical sensitivity at low bilirubin concentrations – Insensitive to high protein concentrations • Jendrassik-Grof Animation – http://webcls.utmb.edu/lo/publicdl.asp?616404F 6782E84851260BFF8F344F92903AF Reference Ranges for Bilirubin Urine Bilirubin • Presence indicates conjugated hyperbilirubinemia • Detected using urine dipsticks – Have a diazo reagent imbedded in the strip – Follows the Ehrlich principle – (Chemstrip/Multistix) • Fresh urine should be used – Avoid light and oxidation Urobilinogen • End product of bilirubin metabolism • Majority excreted in feces, some reabsorbed and returned to the liver • Increased – Hemolytic disease – Defective liver-cell function • Decreased – Biliary obstruction – Carcinoma Determination of Urobilinogen • Ehrlich’s reaction – Ehrlich’s reagent=p-dimethyl aminobenzaldehyde – Urobilinogen + Ehrlich’s reagent = Red color – Performed on fresh urine • Reference Range – 0.1-1.0 Ehrlich units in two hours Enzymes • Liver damage results in the release of enzymes into the circulation • Differentiate between functional or mechanical causes of disease • Significant enzymes – – – – – – AST ALT ALP GGT 5’ nucleotidase LDH Enzymes • Aminotransferases – ALT and AST rise rapidly in most diseases of the liver and stay elevated for up to 2-6 weeks – Highest levels seen with hepatitis, hepatic ischemia and drug/toxin-induced necrosis • Phosphatases – ALP differentiates hepatobiliary disease from bone disease – 5’-Nucleotidase is elevated in hepatobiliary disease Enzymes • GGT elevated in biliary obstruction and in chronic alcoholism • LDH/LD serves as a nonspecific marker of cellular injury Enzymes: Points to Remember • Elevated Liver enzymes are as easy as ABC – Alcoholism – Biliary Obstruction – Cirrhosis Misc. Liver Function Tests • Prothrombin time – Elevated in liver disease • Ammonia – Elevated in liver disease • Glucose/Galactose Tolerance – Assess the liver’s ability to metabolize carbohydrates Disease States Condition AST ALT ALP GGT Albumin Alcoholic hepatits I I NI III N Acute Hepatitis III II I I N Biliary Obstruction NI NI I I I Cirrhosis NI NI NI NI D Reye’s Syndrome I I N I= Increased N= Normal Hepatitis A Markers • Performed by serological antibodies – IgM indicates acute infection and can persist for 3-6 months – IgG appears shortly after IgM, and confers lifelong immunity. Hepatitis B Markers •HBsAG: Hepatitis B Surface Antigen •Detected prior to onset of symptoms •HBcAG: Hepatitis B Core Antigen •Found in an acute infection •HBeAg: Hepatitis B Envelope Antigen •Found in acute and chronic infections Hepatitis B Virus Hepatitis C Testing • Two methods currently used – Anti-HCV detection by EIA (Screen) • A positive test indicates exposure to HCV, it can not determine a current infection versus a past infection – Quantitative nucleic acid PCR for HCV RNA (Confirmatory) References • Bishop, M., Fody, E., & Schoeff, l. (2010). Clinical Chemistry: Techniques, principles, Correlations. Baltimore: Wolters Kluwer Lippincott Williams & Wilkins. • http://www.abbottdiagnostics.co.uk/About_Us/UK/hepatitis_ antigen.cfm • http://depts.washington.edu/labweb/Divisions/Viro/Hepatitis _sero.htm • http://tmp.kiwix.org:4201/A/Hepatitis_B.html • Sunheimer, R., & Graves, L. (2010). Clinical Laboratory Chemistry. Upper Saddle River: Pearson .