Human Diseases
A Systemic Approach
Sixth Edition
Mary Lou Mulvihill
Mark Zelman
Paul Holdaway
Elaine Tompary
Jill Raymond
Chapter 9
Diseases of the Respiratory System
Mulvihill, Zelman, Holdaway, Tompary, and Raymond
Human Diseases: A Systemic Approach, 6e
Copyright ©2006 by Prentice-Hall, Inc.
Upper Saddle River, New Jersey 07458
All rights reserved.
Chapter 9
Diseases of the Respiratory System
Multimedia Asset Directory
Slide 5
Slide 27
Slide 28
Slide 29
Slide 30
Slide 33
Slide 41
The Respiratory System
Asthma
Asthma (Continued)
Assesing Respiratory Rate
Tuberculosis Testing and
Analysis
Allergic Rhinitis
Sleep Apnea
Mulvihill, Zelman, Holdaway, Tompary, and Raymond
Human Diseases: A Systemic Approach, 6e
Slide 51
Slide 54
Slide 72
Slide 89
Slide 96
Slide 100
Influenza
Pulmonary Disease
Emphysema
Tuberculosis
Cystic Fibrosis
Spirometry
Copyright ©2006 by Prentice-Hall, Inc.
Upper Saddle River, New Jersey 07458
All rights reserved.
Overview
Organs of the Respiratory System
Bronchial tubes
Larynx
Lungs
Nose
Pharynx
Trachea
Mulvihill, Zelman, Holdaway, Tompary, and Raymond
Human Diseases: A Systemic Approach, 6e
Copyright ©2006 by Prentice-Hall, Inc.
Upper Saddle River, New Jersey 07458
All rights reserved.
Respiratory System Consists of
6 Major Organs
Nose
Pharynx
Larynx
Trachea
Bronchial tubes
Lungs
All function together to perform respiration.
Mulvihill, Zelman, Holdaway, Tompary, and Raymond
Human Diseases: A Systemic Approach, 6e
Copyright ©2006 by Prentice-Hall, Inc.
Upper Saddle River, New Jersey 07458
All rights reserved.
Click on the screenshot to view an animation showing the
respiratory system.
Mulvihill, Zelman, Holdaway, Tompary, and Raymond
Human Diseases: A Systemic Approach, 6e
Return to Directory
Copyright ©2006 by Prentice-Hall, Inc.
Upper Saddle River, New Jersey 07458
All rights reserved.
Respiratory System
Body cells require constant exchange of
fresh oxygen and removal of carbon
dioxide.
Respiratory system works in conjunction
with cardiovascular system.
Process must be continuous.
Mulvihill, Zelman, Holdaway, Tompary, and Raymond
Human Diseases: A Systemic Approach, 6e
Copyright ©2006 by Prentice-Hall, Inc.
Upper Saddle River, New Jersey 07458
All rights reserved.
Figure 9-1: The respiratory system
Mulvihill, Zelman, Holdaway, Tompary, and Raymond
Human Diseases: A Systemic Approach, 6e
Copyright ©2006 by Prentice-Hall, Inc.
Upper Saddle River, New Jersey 07458
All rights reserved.
3 Distinct Parts of Respiration
Ventilation – flow of air between outside
and lungs
Inhalation – flow of air into lungs; brings
fresh oxygen
Exhalation – flow of air out of lungs;
removes carbon dioxide
Mulvihill, Zelman, Holdaway, Tompary, and Raymond
Human Diseases: A Systemic Approach, 6e
Copyright ©2006 by Prentice-Hall, Inc.
Upper Saddle River, New Jersey 07458
All rights reserved.
External Respiration
Exchange of oxygen and carbon dioxide in
lungs
Gases diffuse in opposite directions
– Between air sacs of lungs and bloodstream
Oxygen enters bloodstream
Carbon dioxide leaves bloodstream.
Mulvihill, Zelman, Holdaway, Tompary, and Raymond
Human Diseases: A Systemic Approach, 6e
Copyright ©2006 by Prentice-Hall, Inc.
Upper Saddle River, New Jersey 07458
All rights reserved.
Internal Respiration
Oxygen and carbon dioxide exchange at
cellular level
Delivered to tissues
Necessary for metabolism
Referred to as tissue breathing
Mulvihill, Zelman, Holdaway, Tompary, and Raymond
Human Diseases: A Systemic Approach, 6e
Copyright ©2006 by Prentice-Hall, Inc.
Upper Saddle River, New Jersey 07458
All rights reserved.
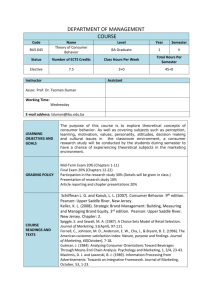
Figure 9-2: Exchange of gases between lungs and blood. High
concentration of CO2 in blood capillary to alveolus diffuses into
alveolus. High concentration of O2 in alveolus diffuses into blood
capillary leaving lung.
Mulvihill, Zelman, Holdaway, Tompary, and Raymond
Human Diseases: A Systemic Approach, 6e
Copyright ©2006 by Prentice-Hall, Inc.
Upper Saddle River, New Jersey 07458
All rights reserved.
Nose and Nasal Cavity
Beginning of ventilation process
Air enters the nasal cavity through the nostrils or nares.
The nasal cavity is divided by the nasal septum, a
cartilaginous plate.
The palate in the roof of the mouth separates the nasal
cavity above from the mouth below.
The walls of the nasal cavity and nasal septum are made
of flexible cartilage covered with mucous membrane.
Mucus cleanses air by trapping dust and bacteria.
Small hairs or cilia line the opening to the nose and filter
out large dirt particles before they can enter the nostrils.
Capillaries in the mucous membranes warm the air.
Several paranasal sinuses are located in the facial bones.
Mulvihill, Zelman, Holdaway, Tompary, and Raymond
Human Diseases: A Systemic Approach, 6e
Copyright ©2006 by Prentice-Hall, Inc.
Upper Saddle River, New Jersey 07458
All rights reserved.
Figure 9-3: Paranasal sinuses are part of the upper respiratory system.
From here infections may spread via nasopharynx to the middle ear or
bronchi.
Mulvihill, Zelman, Holdaway, Tompary, and Raymond
Human Diseases: A Systemic Approach, 6e
Copyright ©2006 by Prentice-Hall, Inc.
Upper Saddle River, New Jersey 07458
All rights reserved.
The Process of Ventilation
Air enters the nasal cavity
The walls of the nasal
through two external
openings called the two
nares.
The nasal cavity is
divided by the nasal
septum.
The palate in the roof of
the mouth separates the
nasal cavity above from
the mouth below.
cavity and the nasal
septum are covered with
mucous membrane.
Inhaled air is moisturized
as it passes by the
surface of the cavity.
Cilia line the opening to
the nose and filter out
large dirt particles.
Mulvihill, Zelman, Holdaway, Tompary, and Raymond
Human Diseases: A Systemic Approach, 6e
Copyright ©2006 by Prentice-Hall, Inc.
Upper Saddle River, New Jersey 07458
All rights reserved.
Pharynx
Air enters the pharynx, or throat, which is
used by the respiratory and digestive
systems.
At the end of the pharynx, air enters the
trachea.
Food and liquids are shunted into the
esophagus.
Mulvihill, Zelman, Holdaway, Tompary, and Raymond
Human Diseases: A Systemic Approach, 6e
Copyright ©2006 by Prentice-Hall, Inc.
Upper Saddle River, New Jersey 07458
All rights reserved.
Pharynx
5-inch tube, 3 parts
– Nasopharynx
– Oropharynx
– Laryngopharynx
3 pairs of tonsils (lymphatic tissue) to keep
out pathogens
– Adenoids
– Palatine
– Lingual
Mulvihill, Zelman, Holdaway, Tompary, and Raymond
Human Diseases: A Systemic Approach, 6e
Copyright ©2006 by Prentice-Hall, Inc.
Upper Saddle River, New Jersey 07458
All rights reserved.
Larynx
Voice box
Muscular structure
Between pharynx and trachea
Contains vocal cords
Mulvihill, Zelman, Holdaway, Tompary, and Raymond
Human Diseases: A Systemic Approach, 6e
Copyright ©2006 by Prentice-Hall, Inc.
Upper Saddle River, New Jersey 07458
All rights reserved.
Epiglottis
A flap of cartilaginous tissue
Sits above the glottis
Keeps food and liquid from being inhaled
into lungs
Covers the larynx and trachea during
swallowing
Thyroid cartilage forms the “Adam’s
apple.”
Mulvihill, Zelman, Holdaway, Tompary, and Raymond
Human Diseases: A Systemic Approach, 6e
Copyright ©2006 by Prentice-Hall, Inc.
Upper Saddle River, New Jersey 07458
All rights reserved.
Trachea
Windpipe
Passageway for air
Extends from pharynx and larynx to main
bronchi
Approximately 4 inches in length
Composed of smooth muscle and cartilage
rings
Lined with mucous membrane and cilia
Assists in cleansing, warming, and moisturizing
air as it travels to the lungs
Mulvihill, Zelman, Holdaway, Tompary, and Raymond
Human Diseases: A Systemic Approach, 6e
Copyright ©2006 by Prentice-Hall, Inc.
Upper Saddle River, New Jersey 07458
All rights reserved.
Bronchial Tubes
Formed by the division of the distal end of the trachea
Left and right main bronchi
Each bronchus enters one and branches to form secondary bronchi.
Each secondary bronchi becomes more narrow to form the
bronchioles.
Each bronchiole terminates in a small group of air sacs (alveoli).
Approximately 150 million alveoli in each lung
Network of pulmonary capillaries encases each alveolus = the
respiratory membrane
External respiration, the exchange of oxygen (O2) and carbon dioxide
(CO2) between the air within the alveolus and the blood inside the
capillaries, takes place across the respiratory membrane.
Mulvihill, Zelman, Holdaway, Tompary, and Raymond
Human Diseases: A Systemic Approach, 6e
Copyright ©2006 by Prentice-Hall, Inc.
Upper Saddle River, New Jersey 07458
All rights reserved.
Lungs
2 lungs; right lung has 3 lobes and left lung has
2 lobes
A lung is the total collection of the bronchi,
bronchioles, and alveoli.
Spongy because they contain air
Protected externally by the ribs
Protected internally by a double membrane
called the pleura
Mulvihill, Zelman, Holdaway, Tompary, and Raymond
Human Diseases: A Systemic Approach, 6e
Copyright ©2006 by Prentice-Hall, Inc.
Upper Saddle River, New Jersey 07458
All rights reserved.
Pleura
Parietal pleura is the outer membrane which
also lines the wall of the chest cavity.
Visceral pleura is the inner membrane; it
adheres to the surface of the lungs.
Pleura is folded to form a sac around each lung
= pleural cavity.
Serous fluid is between the two pleural layers to
reduce friction when the two layers rub together
during ventilation.
Mulvihill, Zelman, Holdaway, Tompary, and Raymond
Human Diseases: A Systemic Approach, 6e
Copyright ©2006 by Prentice-Hall, Inc.
Upper Saddle River, New Jersey 07458
All rights reserved.
Respiratory Muscles
Diaphragm is the muscle separating the
abdomen from the thoracic cavity. It contracts
and moves down into the abdominal cavity,
which causes a decrease of pressure, or
negative thoracic pressure, within the chest
cavity. Air can then enter the lungs to equalize
the pressure during inhalation.
Intercostal muscles are between the ribs. They
assist in inhalation by raising the rib cage to
enlarge the thoracic cavity.
Mulvihill, Zelman, Holdaway, Tompary, and Raymond
Human Diseases: A Systemic Approach, 6e
Copyright ©2006 by Prentice-Hall, Inc.
Upper Saddle River, New Jersey 07458
All rights reserved.
Lung Volumes and Capacities
It is important to know the lung capacity and the
volume of air that is actually flowing in and out of
the lungs.
The actual volume of air exchanged in breathing
is measured by respiratory specialists to aid in
determining the functioning level of the
respiratory system.
This volume is measured with pulmonary
function equipment.
Mulvihill, Zelman, Holdaway, Tompary, and Raymond
Human Diseases: A Systemic Approach, 6e
Copyright ©2006 by Prentice-Hall, Inc.
Upper Saddle River, New Jersey 07458
All rights reserved.
Respiratory Rate
One of the four vital signs (VS), along with heart
rate, temperature, and blood pressure.
Respiratory rate is dependent on the level of
CO2 in the blood.
When the CO2 level is high, a person breathes
more rapidly to expel the excess.
If CO2 levels drop, the respiratory rate will also
drop.
Mulvihill, Zelman, Holdaway, Tompary, and Raymond
Human Diseases: A Systemic Approach, 6e
Copyright ©2006 by Prentice-Hall, Inc.
Upper Saddle River, New Jersey 07458
All rights reserved.
Respiratory Rates for Different
Age Groups
Age
Newborn
1 year old
16 year old
Adult
Respirations per Minute
30–60
18–30
16–20
12–20
Mulvihill, Zelman, Holdaway, Tompary, and Raymond
Human Diseases: A Systemic Approach, 6e
Copyright ©2006 by Prentice-Hall, Inc.
Upper Saddle River, New Jersey 07458
All rights reserved.
Click on the screenshots to view animations on asthma.
Mulvihill, Zelman, Holdaway, Tompary, and Raymond
Human Diseases: A Systemic Approach, 6e
Return to Directory
Copyright ©2006 by Prentice-Hall, Inc.
Upper Saddle River, New Jersey 07458
All rights reserved.
Click on the screenshots to view the video and animation
for asthma.
Mulvihill, Zelman, Holdaway, Tompary, and Raymond
Human Diseases: A Systemic Approach, 6e
Return to Directory
Copyright ©2006 by Prentice-Hall, Inc.
Upper Saddle River, New Jersey 07458
All rights reserved.
Click on the screenshots to view videos on the topic of
assessing respiratory rate.
Mulvihill, Zelman, Holdaway, Tompary, and Raymond
Human Diseases: A Systemic Approach, 6e
Return to Directory
Copyright ©2006 by Prentice-Hall, Inc.
Upper Saddle River, New Jersey 07458
All rights reserved.
Click on the screenshot to view a video on tuberculosis
testing and analysis.
Mulvihill, Zelman, Holdaway, Tompary, and Raymond
Human Diseases: A Systemic Approach, 6e
Return to Directory
Copyright ©2006 by Prentice-Hall, Inc.
Upper Saddle River, New Jersey 07458
All rights reserved.
Upper Respiratory Diseases
Common cold
Sinusitis
Nasal polyps
Snoring and obstructive sleep apnea
Hay Fever (seasonal allergic rhinitis)
Tonsillitis, pharyngitis, laryngitis
Influenza
Mulvihill, Zelman, Holdaway, Tompary, and Raymond
Human Diseases: A Systemic Approach, 6e
Copyright ©2006 by Prentice-Hall, Inc.
Upper Saddle River, New Jersey 07458
All rights reserved.
Table 9-1: Comparison of Allergy, Cold, and Influenza.
Mulvihill, Zelman, Holdaway, Tompary, and Raymond
Human Diseases: A Systemic Approach, 6e
Copyright ©2006 by Prentice-Hall, Inc.
Upper Saddle River, New Jersey 07458
All rights reserved.
Click on the screenshot to view a video on the topic of
allergic rhinitis.
Mulvihill, Zelman, Holdaway, Tompary, and Raymond
Human Diseases: A Systemic Approach, 6e
Return to Directory
Copyright ©2006 by Prentice-Hall, Inc.
Upper Saddle River, New Jersey 07458
All rights reserved.
The Common Cold
More than 200 strains of viruses are capable of
causing this disease. Metapneumovirus, within
the paramyxovirus family of viruses, has recently
been described as a major virus causing adult
colds, and it acts very severely on infants when
first encountered.
In the weak or elderly this agent is taken
cautiously as well. Unlike many other diseases,
having had a cold provides no immunity.
Another strain of virus is always ready to attack.
Moreover, the common cold is relatively
contagious.
Mulvihill, Zelman, Holdaway, Tompary, and Raymond
Human Diseases: A Systemic Approach, 6e
Copyright ©2006 by Prentice-Hall, Inc.
Upper Saddle River, New Jersey 07458
All rights reserved.
Common Cold Symptoms, Etiology,
and Treatment
A cold is an acute inflammation of the mucous membrane lining the
upper respiratory tract. The initial stuffed-up feeling, is caused by the
swelling of the mucous membrane, which narrows the air
passageway. Copious secretion of mucus follows acute
inflammation.
There is no known cure for the common cold. Beyond bed rest, cold
symptoms can be treated by taking aspirin for fever and
antihistamines for relieving congestion.
Coughing helps clear irritants or excessive mucus in the nasal and
throat areas, and sometimes this abrupt flow of air races by at
speeds approaching 200 mph. Occasionally secondary infections
occur. The infection may be treated with antibiotics when caused by
bacteria, and therefore cold sufferers may be on antibiotics for a
“cold.”
Mulvihill, Zelman, Holdaway, Tompary, and Raymond
Human Diseases: A Systemic Approach, 6e
Copyright ©2006 by Prentice-Hall, Inc.
Upper Saddle River, New Jersey 07458
All rights reserved.
Sinuses And Sinusitis
In the United States, approximately one person in seven
has sinus problems at a cost of more than a billion
dollars per year. The air filled spaces provide a reduced
weight for the skull and contribute to nasal tone of the
voice.
Paranasal sinuses drain into the nasal cavity. These
cavities are named by the skull bone in which they are
found: frontal, ethmoid, maxillary, and sphenoid.
In sinusitis, the inflammation of the mucous membranes
that line the cavity causes a sensation of pressure, pain,
and often a headache. Children have a tendency toward
ethmoid sinus inflammation more commonly than do
adults.
Mulvihill, Zelman, Holdaway, Tompary, and Raymond
Human Diseases: A Systemic Approach, 6e
Copyright ©2006 by Prentice-Hall, Inc.
Upper Saddle River, New Jersey 07458
All rights reserved.
Sinusitis Etiology, Symptoms,
Treatment
Viruses, allergens, bacteria
Environmental conditions
– barometric pressure, airplane flight, swimming or diving
activities, and perhaps stale or contaminated indoor air like in
“sick building syndrome.”
– tooth extraction or dental work, abscesses, and allergens.
Sinusitis, an infection of the sinuses, can be caused by nasal
congestion blocking sinus drainage.
When the mucous membranes lining these cavities are
inflamed the results are headache above or below the
eye orbit, occasionally pain in the cheeks and upper
teeth and a general “stuffiness” felt behind or within the
nasal cavity.
Mulvihill, Zelman, Holdaway, Tompary, and Raymond
Human Diseases: A Systemic Approach, 6e
Copyright ©2006 by Prentice-Hall, Inc.
Upper Saddle River, New Jersey 07458
All rights reserved.
Sinusitis Etiology, Symptoms,
Treatment (continued)
Depending on the cause, susceptibility, and severity of a
case of sinusitis, it may take 3 to 4 weeks to resolve.
A thick viscous discharge varying in yellowish to green
color may suggest a bacterial invasion has occurred.
Sinusitis may be confirmed by physical observation that
may include x-ray and endoscopic sinuscopy plus patient
history. Discharge samples may be sent to the
laboratory to confirm or rule out bacterial invasion or
other agents.
Treatment: decongestants and antihistamines,
antibiotics, surgery
Mulvihill, Zelman, Holdaway, Tompary, and Raymond
Human Diseases: A Systemic Approach, 6e
Copyright ©2006 by Prentice-Hall, Inc.
Upper Saddle River, New Jersey 07458
All rights reserved.
Nasal Polyps
Nasal polyps are noncancerous growths within the nose or sinus
passageway. The exact cause of these growths is unknown.
Certain chemicals found within these polyps suggest that they may
be instrumental in causing the extra tissue formations.
Typically, nasal polyps form along with a sensitivity or allergic
response to aspirin and some aspirin-like substitutes. Individuals
with asthma and chronic rhinitis (nasal inflammation) are
susceptible, as are children with cystic fibrosis.
Large polyps cause nasal drainage, interfere with smell capability,
and, on rare occasions may be linked to obstructive sleep apnea
(OSA). Treatment primarily suggests surgery, but only if the polyps
are troublesome.
Nasal sprays with cortisone-like drugs are used for allergy control.
However, even if the surgery clears the passageway, it may not
prevent the uncertain cause of these internal nasal lumps.
Mulvihill, Zelman, Holdaway, Tompary, and Raymond
Human Diseases: A Systemic Approach, 6e
Copyright ©2006 by Prentice-Hall, Inc.
Upper Saddle River, New Jersey 07458
All rights reserved.
Obstructive Sleep Apnea
The most common sleep disorder
The apnea is noted by cessation of breathing during the
night due to a non-foreign obstruction like an inhaled
object, but caused by enlarged parts (e.g., nasal polyps
or uvula) or displaced parts like deviated septum or fatty
bodies.
Usually occurs in middle age, and in overweight males.
Individuals awake tired, without energy, and feel drowsy
most of the day while functioning at low capacity.
Four or five episodes of sleep apnea per hour is
significant. Twenty episodes per hour is severe; some
people experience 100–500 apneas in a single night.
Mulvihill, Zelman, Holdaway, Tompary, and Raymond
Human Diseases: A Systemic Approach, 6e
Copyright ©2006 by Prentice-Hall, Inc.
Upper Saddle River, New Jersey 07458
All rights reserved.
Click on the screenshot to view a video on the topic of
sleep apnea.
Mulvihill, Zelman, Holdaway, Tompary, and Raymond
Human Diseases: A Systemic Approach, 6e
Return to Directory
Copyright ©2006 by Prentice-Hall, Inc.
Upper Saddle River, New Jersey 07458
All rights reserved.
Obstructive Sleep Apnea Syndrome:
Symptoms and Treatment
Obstructive apnea causes heavy, long, and loud snoring and
snorting.
Three fourths of the time researchers have found that during this
interruption, decreased blood flow to the brain has occurred.
With upper airways blocked, lungs do not fill properly, which creates
a pressure in the chest that compresses the heart, and therefore
reduces blood flow.
The potential for cerebral stroke is increased, especially in moderate
and severe apnea cases. Causes and treatment for OSA were
outlined in the previous section.
Treatment depends on the particular case, but if weight is a problem
it may be dealt with without fanfare. If sinuses or nasal cavities are
misshaped or blocked they need repair. Some patients find relief
with pharyngoplasty—trimming of the uvula (superior mid throat
flap) to prevent blockage of breathing passageway.
Mulvihill, Zelman, Holdaway, Tompary, and Raymond
Human Diseases: A Systemic Approach, 6e
Copyright ©2006 by Prentice-Hall, Inc.
Upper Saddle River, New Jersey 07458
All rights reserved.
Hay fever
Also called seasonal allergic rhinitis, it is characterized by sensitivity
to airborne allergens, especially from pollens of ragweed and
grasses.
Respiratory mucosa secrete excessive mucus causing a runny nose
and congestion.
Mucosal surfaces of the eyes also react to the allergens causing
redness, watery secretions, and itching.
Because the release of histamine causes these unpleasant effects,
a substance that counteracts its action, an antihistamine, may give
relief.
Newer medications like Flonase may help sufferers on a short-term
basis.
Many hay fever sufferers take allergy injections to desensitize them
to pollen or other allergens.
– Desensitizing works by administering small doses of antigen and
gradually increasing the dosage, allowing the person to produce
antibodies against it. It is hoped that these antibodies can
inactivate the pollen before it interacts with the nasal mucosa.
Mulvihill, Zelman, Holdaway, Tompary, and Raymond
Human Diseases: A Systemic Approach, 6e
Copyright ©2006 by Prentice-Hall, Inc.
Upper Saddle River, New Jersey 07458
All rights reserved.
Tonsillitis, Pharyngitis, Laryngitis
These upper respiratory airway structures
can become infected with bacteria,
viruses, or other pathogens.
Infections of these tissues lead to difficulty
swallowing, and redness and pain in the
throat.
Mulvihill, Zelman, Holdaway, Tompary, and Raymond
Human Diseases: A Systemic Approach, 6e
Copyright ©2006 by Prentice-Hall, Inc.
Upper Saddle River, New Jersey 07458
All rights reserved.
Tonsillitis
The tonsils are masses of lymphatic tissue
located in the mucous membranes of the
fauces and the oral pharynx that protect
the throat from infection.
Infected tonsils may swell and become
painful, making swallowing very difficult.
When persistent bouts of infection
continue, it may call for surgical measures
(tonsillectomy), especially when the middle
ear (otitis media) becomes inflamed.
Mulvihill, Zelman, Holdaway, Tompary, and Raymond
Human Diseases: A Systemic Approach, 6e
Copyright ©2006 by Prentice-Hall, Inc.
Upper Saddle River, New Jersey 07458
All rights reserved.
Figure 9-4: Tonsils - normal and enlarged.
Mulvihill, Zelman, Holdaway, Tompary, and Raymond
Human Diseases: A Systemic Approach, 6e
Copyright ©2006 by Prentice-Hall, Inc.
Upper Saddle River, New Jersey 07458
All rights reserved.
Pharyngitis
An inflammation of the pharynx characterized by pain in
the throat. Foreign objects, hot liquids, or spicy foods
may contribute to short-term pharyngitis.
Just breathing through the mouth, due to stuffiness, or
falling asleep with an open mouth may cause a brief
discomfort caused by excessive drying and exposure.
Strep throat, a pharyngitis caused by streptococci, is
common, resulting in a red, purulent throat.
The presence of bacteria in the throat can be confirmed
by a throat culture or a rapid immunological test that can
be performed in the physician’s office.
Antibiotics control the infection.
Mulvihill, Zelman, Holdaway, Tompary, and Raymond
Human Diseases: A Systemic Approach, 6e
Copyright ©2006 by Prentice-Hall, Inc.
Upper Saddle River, New Jersey 07458
All rights reserved.
Laryngitis
An inflammation of the larynx or voice box, is
characterized by hoarseness and aphonia. A
“lost voice” may be caused by bacteria or
viruses or perhaps fungi, but it can also stem
from allergies, overuse of the voice, as
experienced by singers, politicians, and
auctioneers, and other factors.
For bacterial infections, antibiotics are used.
Laryngitis, which is one form of the “croup,” can
also be treated by resting the voice, drinking
fluids, and steam inhalations.
Mulvihill, Zelman, Holdaway, Tompary, and Raymond
Human Diseases: A Systemic Approach, 6e
Copyright ©2006 by Prentice-Hall, Inc.
Upper Saddle River, New Jersey 07458
All rights reserved.
Influenza
A viral infection of the upper respiratory system.
The onset of the disease is sudden. The individual experiences
chills and a fever, cough, sore throat, and runny nose. Chest pains,
muscular aching, and gastrointestinal disorders may also be
symptoms.
Many different strains of viruses causing influenza are known.
Unfortunately, immunity for one strain does not protect against
another strain.
There is a broad range in the severity of flu cases. It can be very
mild, or it can lead to pneumonia and be life-threatening. Influenza is
particularly serious in the elderly and chronically ill.
The virus can destroy the respiratory epithelium, a strong line of
defense against bacterial invasion. With the loss of the protective
epithelium, bacterial infection can invade any part of the respiratory
tract. Pneumococci, streptococci, and staphylococci are all capable
of causing pneumonia in patients with severe influenza.
Mulvihill, Zelman, Holdaway, Tompary, and Raymond
Human Diseases: A Systemic Approach, 6e
Copyright ©2006 by Prentice-Hall, Inc.
Upper Saddle River, New Jersey 07458
All rights reserved.
Treatment of Influenza
There is no medication that cures influenza.
Sometimes antibiotics are prescribed to ward off
secondary bacterial infection.
Bed rest, fluids, and aspirin to reduce fever are
the usual treatments.
Flu vaccines are made available before the
onset of the season, typically in October and
November, and are recommended for those
considered at high risk; elderly and respiratory
compromised. Unfortunately, these shots do not
give immunity for all strains of the influenza
virus.
Mulvihill, Zelman, Holdaway, Tompary, and Raymond
Human Diseases: A Systemic Approach, 6e
Copyright ©2006 by Prentice-Hall, Inc.
Upper Saddle River, New Jersey 07458
All rights reserved.
Click on the screenshot to view a video on the topic of
influenza.
Mulvihill, Zelman, Holdaway, Tompary, and Raymond
Human Diseases: A Systemic Approach, 6e
Return to Directory
Copyright ©2006 by Prentice-Hall, Inc.
Upper Saddle River, New Jersey 07458
All rights reserved.
Lower Respiratory Diseases
Chronic obstructive pulmonary disease
Bronchitis
Asthma
Emphysema
Pneumonia
Pleurisy
Pulmonary tuberculosis
Cancer
Cystic fibrosis
Mulvihill, Zelman, Holdaway, Tompary, and Raymond
Human Diseases: A Systemic Approach, 6e
Copyright ©2006 by Prentice-Hall, Inc.
Upper Saddle River, New Jersey 07458
All rights reserved.
Chronic Obstructive Pulmonary
Disease (COPD)
Chronic obstructive lung disease (COLD),
includes a number of conditions in which
the exchange of respiratory gasses is
ineffective. It includes chronic bronchitis,
emphysema, and chronic asthma.
Mulvihill, Zelman, Holdaway, Tompary, and Raymond
Human Diseases: A Systemic Approach, 6e
Copyright ©2006 by Prentice-Hall, Inc.
Upper Saddle River, New Jersey 07458
All rights reserved.
Click on the screenshot to view a video on the topic of
pulmonary diseases.
Mulvihill, Zelman, Holdaway, Tompary, and Raymond
Human Diseases: A Systemic Approach, 6e
Return to Directory
Copyright ©2006 by Prentice-Hall, Inc.
Upper Saddle River, New Jersey 07458
All rights reserved.
Bronchitis
Inflammation of the bronchi, which may be
acute or chronic.
The mucous membrane lining the bronchi
becomes swollen and red, the typical
inflammatory response. Irritants such as
industrial fumes, automobile exhaust,
viruses, or bacteria can cause acute
bronchitis.
Mulvihill, Zelman, Holdaway, Tompary, and Raymond
Human Diseases: A Systemic Approach, 6e
Copyright ©2006 by Prentice-Hall, Inc.
Upper Saddle River, New Jersey 07458
All rights reserved.
Acute Bronchitis
Most serious in small children, the chronically ill, and the
elderly.
Tiny bronchioles of children can become easily
obstructed. The elderly or chronically ill are likely to
develop a secondary infection, such as pneumonia.
Acute bronchitis is characterized by chest pains,
dyspnea, cough, fever, and sometimes chills.
The sputum coughed up may contain pus.
Depending on the organism causing the bronchitis,
antibiotics may be administered. Viruses do not respond
to antibiotics, but vapors, sprays, and cough medicines
may give relief.
Mulvihill, Zelman, Holdaway, Tompary, and Raymond
Human Diseases: A Systemic Approach, 6e
Copyright ©2006 by Prentice-Hall, Inc.
Upper Saddle River, New Jersey 07458
All rights reserved.
Chronic Bronchitis
Indicated by repeated attacks of acute bronchitis
and coughing with sputum production, lasting for
at least 3 months for 2 consecutive years.
Symptoms are persistent.
Chronic bronchitis may be a complication of
another respiratory infection, or can result from
long-term exposure to air pollutants or cigarette
smoke. It is more common in middle-aged men
than in women.
Mulvihill, Zelman, Holdaway, Tompary, and Raymond
Human Diseases: A Systemic Approach, 6e
Copyright ©2006 by Prentice-Hall, Inc.
Upper Saddle River, New Jersey 07458
All rights reserved.
Symptoms of Bronchitis
Symptoms include excessive secretion of mucus from the mucous
glands of the bronchial mucosa (lining). The mucous glands
hypertrophy, and the mucosa itself is thickened and inflamed.
The interference in the air passageway caused by the swelling and
mucus reduces the person’s oxygen level.
Hypoxia, an insufficient oxygenation of the tissues, results. Poor
drainage of the mucus sets the stage for bacterial infection. Parts of
the respiratory tract can become necrotic, and fibrous scarring
follows.
Chronic bronchitis is aggravated by other respiratory diseases or
environmental factors.
The symptoms can be treated with antibiotics and moist vapors to
ease the breathing. A cigarette smoker should quit smoking, and
clean air environments should be sought at all times.
Mulvihill, Zelman, Holdaway, Tompary, and Raymond
Human Diseases: A Systemic Approach, 6e
Copyright ©2006 by Prentice-Hall, Inc.
Upper Saddle River, New Jersey 07458
All rights reserved.
Bronchial Asthma
Characterized by hypersensitivity to various
allergens like dust, mold, pollen, animal dander,
and various foods
Eighty percent of children with asthma and fifty
percent of adult asthmatics have allergies. The
allergens trigger constriction of smooth muscle
in the walls of the bronchi, narrowing the lumen
of the tubes. The spasm is a sustained
contraction of the musculature, making
breathing, particularly expiration, very difficult.
Mulvihill, Zelman, Holdaway, Tompary, and Raymond
Human Diseases: A Systemic Approach, 6e
Copyright ©2006 by Prentice-Hall, Inc.
Upper Saddle River, New Jersey 07458
All rights reserved.
Bronchial Asthma (continued)
The mucous membrane becomes swollen with
fluid, also narrowing the lumen. Excessive
secretion of mucus adds to the obstruction. Stale
air becomes trapped, which decreases the
amount of fresh air that can enter the lungs.
The wheezing sound results from air passing
through the narrowed tubes. Psychogenic
factors such as anxiety are frequently associated
with an asthma attack.
A tense situation or an emotional experience
can trigger an attack.
Mulvihill, Zelman, Holdaway, Tompary, and Raymond
Human Diseases: A Systemic Approach, 6e
Copyright ©2006 by Prentice-Hall, Inc.
Upper Saddle River, New Jersey 07458
All rights reserved.
Bronchial Asthma (continued)
Other nonallergic causes are overexertion,
infection, or bronchitis. Exposure of the bronchial
mucosa to irritants such as cigarette smoke,
aerosol sprays, or perfume can also trigger an
attack.
There is no cure for asthma, but attacks may
become less severe with age. It is important to
identify the offending allergens and avoid contact
with them as much as possible.
Because overexertion may be involved, it is
important for the athlete to take some extra time to
“warm up” and get adjusted to the situation before
participating in physical activities and sports.
Mulvihill, Zelman, Holdaway, Tompary, and Raymond
Human Diseases: A Systemic Approach, 6e
Copyright ©2006 by Prentice-Hall, Inc.
Upper Saddle River, New Jersey 07458
All rights reserved.
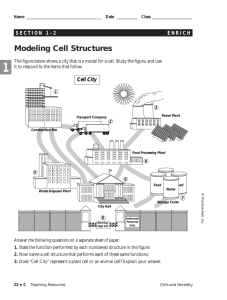
Figure 9-5: Normal bronchiole (A) and one constricted (B)
in asthma attack.
Mulvihill, Zelman, Holdaway, Tompary, and Raymond
Human Diseases: A Systemic Approach, 6e
Copyright ©2006 by Prentice-Hall, Inc.
Upper Saddle River, New Jersey 07458
All rights reserved.
Normal lung alveoli magnified 25X
(© J. Seibert/ Custom Medical Stock Photo.)
Mulvihill, Zelman, Holdaway, Tompary, and Raymond
Human Diseases: A Systemic Approach, 6e
Copyright ©2006 by Prentice-Hall, Inc.
Upper Saddle River, New Jersey 07458
All rights reserved.
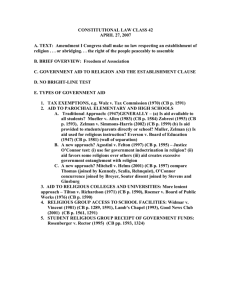
Emphysema. Note enlarged and fused alveoli in
emphysema.
(© C. Abrahams, M.D./Custom Medical Stock Photo.)
Mulvihill, Zelman, Holdaway, Tompary, and Raymond
Human Diseases: A Systemic Approach, 6e
Copyright ©2006 by Prentice-Hall, Inc.
Upper Saddle River, New Jersey 07458
All rights reserved.
Treatment and Prognosis
of Asthma
Medication and allergy shots can reduce the
incidence or severity of asthma attacks.
To counteract an ongoing attack, substances
that dilate the bronchi are effective. Ephedrine
sprays and epinephrine (adrenalin) injections
are often effective.
Bronchodilators like albuterol and
metaproterenol are sometimes prescribed.
Cortisone-like drugs and antihistamines are
sometimes used, but these carry a risk of side
effects.
Mulvihill, Zelman, Holdaway, Tompary, and Raymond
Human Diseases: A Systemic Approach, 6e
Copyright ©2006 by Prentice-Hall, Inc.
Upper Saddle River, New Jersey 07458
All rights reserved.
Treatment and Prognosis
of Asthma (continued)
The most severe form of an asthma attack is
called status asthmaticus, in which the patient
fails to respond to the usual treatment. A
procedure as drastic as a tracheotomy, an
opening of the trachea surgically, may be
required. If not treated, status asthmaticus may
end in respiratory failure and death.
Asthma kills at least 15 people daily in the
United States, according to the American Lung
Association.
Mulvihill, Zelman, Holdaway, Tompary, and Raymond
Human Diseases: A Systemic Approach, 6e
Copyright ©2006 by Prentice-Hall, Inc.
Upper Saddle River, New Jersey 07458
All rights reserved.
Treatment and Prognosis
of Asthma (continued)
The disease is also increasing across the
country (up 4% in 2002). About 4 million
Americans have asthma and it affects all ages,
but particularly youngsters. Perhaps because of
new building designs since the 1970’s and more
activities occurring indoors, asthma has become
a major concern for the medical community.
Education offers considerable relief
psychologically and physically.
Mulvihill, Zelman, Holdaway, Tompary, and Raymond
Human Diseases: A Systemic Approach, 6e
Copyright ©2006 by Prentice-Hall, Inc.
Upper Saddle River, New Jersey 07458
All rights reserved.
Emphysema
A crippling and debilitating (weakening) disease
with chronic lung obstruction and destruction
The word emphysema means inflation. The
lungs become filled with air that is high in carbon
dioxide. This air cannot be adequately exhaled
to allow oxygen to enter. The person
experiences a suffocating feeling and great
distress from the inability to breathe. Severe
pain accompanies the difficult breathing.
The cause of emphysema is not known, but it is
most frequently associated with heavy cigarette
smoking.
Mulvihill, Zelman, Holdaway, Tompary, and Raymond
Human Diseases: A Systemic Approach, 6e
Copyright ©2006 by Prentice-Hall, Inc.
Upper Saddle River, New Jersey 07458
All rights reserved.
Emphysema (continued)
An inherited form has been identified also.
Individuals with a deficiency in alpha-1antitrypsin are prone to alveolar destruction
characteristic of emphysema.
Air pollution and long-term exposure to irritants
of the respiratory tract also seem to be factors of
its etiology.
Emphysema is a frequent complication of
chronic bronchitis. Whatever the cause, the
alveolar walls break down, adjacent alveoli fuse,
and the lungs lose their elasticity.
Mulvihill, Zelman, Holdaway, Tompary, and Raymond
Human Diseases: A Systemic Approach, 6e
Copyright ©2006 by Prentice-Hall, Inc.
Upper Saddle River, New Jersey 07458
All rights reserved.
Signs and Symptoms of
Emphysema
Typically, a person with emphysema has an
increased rate of breathing and a greater than
normal expansion of the chest. This
hyperventilating clears out carbon dioxide that is
building up internally because of poor lung
functioning.
Permanent expansion of the chest (“barrel”
chest); abnormal respiratory sounds called rales
Right-sided heart failure or cyanosis because of
marked hypoxemia
Hypoventilation reduces oxygenation
Mulvihill, Zelman, Holdaway, Tompary, and Raymond
Human Diseases: A Systemic Approach, 6e
Copyright ©2006 by Prentice-Hall, Inc.
Upper Saddle River, New Jersey 07458
All rights reserved.
Signs and Symptoms of
Emphysema (continued)
Emphysema can last for many years, causing
irreversible damage to the lungs. As in any
serious disease, complications often develop.
With the breakdown of alveolar walls, the
surrounding blood capillaries are damaged.
This interference with circulation in the lungs can
lead to an obstruction of the pulmonary artery.
The large air sacs, formed by the fusion of the
alveoli, tend to rupture. This allows air into the
pleural cavity, the space between the lungs and
the chest wall. Air in this space can cause the
lung to collapse.
Mulvihill, Zelman, Holdaway, Tompary, and Raymond
Human Diseases: A Systemic Approach, 6e
Copyright ©2006 by Prentice-Hall, Inc.
Upper Saddle River, New Jersey 07458
All rights reserved.
Click on the screenshot to view a video on the topic of
emphysema.
Mulvihill, Zelman, Holdaway, Tompary, and Raymond
Human Diseases: A Systemic Approach, 6e
Return to Directory
Copyright ©2006 by Prentice-Hall, Inc.
Upper Saddle River, New Jersey 07458
All rights reserved.
Diagnosis and Treatment
of Emphysema
Early detection of emphysema can slow its
progression. Symptoms such as a chronic cough
(often called smoker’s cough), shortness of
breath, and abnormally rapid breathing indicate
a respiratory disease, and a physician should be
consulted.
A spirometer measures the movement of air in
and out of the lungs
X-rays do not show emphysema in the early
stages.
Mulvihill, Zelman, Holdaway, Tompary, and Raymond
Human Diseases: A Systemic Approach, 6e
Copyright ©2006 by Prentice-Hall, Inc.
Upper Saddle River, New Jersey 07458
All rights reserved.
Diagnosis and Treatment
of Emphysema (continued)
Treatment involves eliminating the source of the
irritation. A smoker will be told to quit smoking and to
avoid polluted air containing smoke, fumes, and irritating
dust. The patient should observe ozone warnings and
limit outdoor activity when the ozone level is high.
Medications that clear mucus from the lungs help
prevent infection. Some medications give relief from the
feeling of not being able to breathe, such as albuterol or
metaproterenol.
Physical therapy is sometimes helpful in teaching
individuals to use all the possible muscles for respiration
in the abdomen and chest wall.
Mulvihill, Zelman, Holdaway, Tompary, and Raymond
Human Diseases: A Systemic Approach, 6e
Copyright ©2006 by Prentice-Hall, Inc.
Upper Saddle River, New Jersey 07458
All rights reserved.
Pneumonia
Acute inflammation of the lungs in which air
spaces in the lungs become filled with an
inflammatory exudate.
Oxygen exchange is impaired, causing difficulty
breathing.
Fever, chest pain, and a productive cough
accompany this disease.
A chest x-ray and analysis of sputum can
diagnose pneumonia and determine its cause.
Pneumonia can be caused by a variety of
microorganisms, and it may affect different areas
of the lungs.
Mulvihill, Zelman, Holdaway, Tompary, and Raymond
Human Diseases: A Systemic Approach, 6e
Copyright ©2006 by Prentice-Hall, Inc.
Upper Saddle River, New Jersey 07458
All rights reserved.
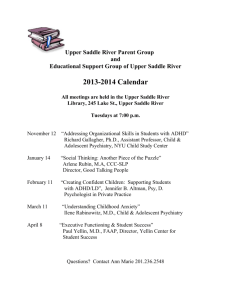
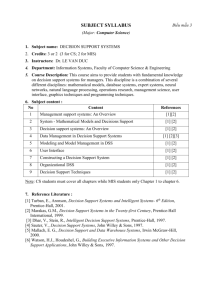
Figure 9-6: (A) Bronchopneumonia with localized pattern. (B) lobar
pneumonia with a diffuse pattern within the lobe. ( C ) interstitial
pneumonia typically diffuse and bilateral.
Mulvihill, Zelman, Holdaway, Tompary, and Raymond
Human Diseases: A Systemic Approach, 6e
Copyright ©2006 by Prentice-Hall, Inc.
Upper Saddle River, New Jersey 07458
All rights reserved.
Lobar Pneumonia
Lobar pneumonia is inflammation of a section,
often an entire lobe, of the lung. It is most often
caused by the pneumococcus bacterium,
Streptococcus pneumoniae.
This bacterium is carried in the respiratory
passages of many people, but it can infect the
lungs under optimal conditions.
People with other disease processes, chronic
bronchitis, or weakened immune systems are
most susceptible. Treatment includes use of
antibiotics, such as penicillin.
Mulvihill, Zelman, Holdaway, Tompary, and Raymond
Human Diseases: A Systemic Approach, 6e
Copyright ©2006 by Prentice-Hall, Inc.
Upper Saddle River, New Jersey 07458
All rights reserved.
Bronchopneumonia
Obstruction of the small bronchi
Due to infection or by aspirated gastric contents
Diffuse pattern of inflammation on x-ray
Mulvihill, Zelman, Holdaway, Tompary, and Raymond
Human Diseases: A Systemic Approach, 6e
Copyright ©2006 by Prentice-Hall, Inc.
Upper Saddle River, New Jersey 07458
All rights reserved.
Bronchopneumonia (continued)
This type of pneumonia is more common in
debilitated patients who are bedridden from
other pathology. Predisposing causes of
bronchopneumonia are:
– Chronic bronchitis
– Measles or whooping cough
– Bronchiectasis
– Old age
– Cancer
Mulvihill, Zelman, Holdaway, Tompary, and Raymond
Human Diseases: A Systemic Approach, 6e
Copyright ©2006 by Prentice-Hall, Inc.
Upper Saddle River, New Jersey 07458
All rights reserved.
Primary Atypical Pneumonia
Caused by a variety of microorganisms,
including viruses and unusual bacteria
called Mycoplasma pneumoniae.
Interstitial pneumonia, common in viral
pneumonia, is characterized by the diffuse
pattern on x-ray
The disease is more common among
adolescents and young adults.
Mulvihill, Zelman, Holdaway, Tompary, and Raymond
Human Diseases: A Systemic Approach, 6e
Copyright ©2006 by Prentice-Hall, Inc.
Upper Saddle River, New Jersey 07458
All rights reserved.
Legionnaires’ Disease
Caused by the bacterium, Legionella pneumophila
Characterized by flu-like symptoms, which sets it apart
from other pneumonias. This is a serious and potentially
fatal disease, and sputum cultures and chest x-rays can
differentiate it from other infections.
The disease is acquired by inhaling droplets
contaminated with the bacteria from air conditioning
cooling systems, humidifiers, and other equipment that
produces aerosol water droplets.
The antibiotic erythromycin is the treatment of choice.
Mulvihill, Zelman, Holdaway, Tompary, and Raymond
Human Diseases: A Systemic Approach, 6e
Copyright ©2006 by Prentice-Hall, Inc.
Upper Saddle River, New Jersey 07458
All rights reserved.
Secondary Pneumonia
Can develop as a secondary disorder from other
diseases that weaken the lungs or the body’s
immune system
Graft recipients and immunocompromised
people, especially HIV/AIDS patients, are
susceptible to pneumonia caused by unusual
infectious agents like the fungus, Pneumocystis
carinii, and the fungus, Cryptococcus
neoformans.
Mulvihill, Zelman, Holdaway, Tompary, and Raymond
Human Diseases: A Systemic Approach, 6e
Copyright ©2006 by Prentice-Hall, Inc.
Upper Saddle River, New Jersey 07458
All rights reserved.
Secondary Pneumonia
(continued)
Postoperative patients, bedridden patients, and those
with chronic respiratory illness may lack the ability to
clear their lungs effectively and are at risk for developing
pneumonia.
The most unfavorable secondary pneumonia is the one
acquired as a complication of influenza. It was
responsible for many of the 20 million deaths in the
Spanish Flu epidemic of 1918–1919. This was a
devastating disease that apparently started in the United
States, was transported to (and from) Europe by
American soldiers and always involved double (both
lungs) pneumonia. Today, influenza still causes many
cases of pneumonia, and the flu vaccine is
recommended for persons at risk.
Mulvihill, Zelman, Holdaway, Tompary, and Raymond
Human Diseases: A Systemic Approach, 6e
Copyright ©2006 by Prentice-Hall, Inc.
Upper Saddle River, New Jersey 07458
All rights reserved.
Pleurisy
An inflammation of the pleural membranes that
occurs as a complication of various lung
diseases, like pneumonia or tuberculosis.
May also develop from an injury or tumor
formation.
Pleurisy is extremely painful; a sharp, stabbing
pain accompanies each inspiration. The pain
may stem from excessive or insufficient pleural
fluid, or pus/blood in the lungs. It is treated with
antibiotics, heat applications, and bed rest.
Mulvihill, Zelman, Holdaway, Tompary, and Raymond
Human Diseases: A Systemic Approach, 6e
Copyright ©2006 by Prentice-Hall, Inc.
Upper Saddle River, New Jersey 07458
All rights reserved.
Pulmonary Tuberculosis
A chronic infectious disease characterized by necrosis of
vital lung tissue
Common in the respiratory system, but can affect other
body systems as well
Caused by the bacterium Mycobacterium tuberculosis
and related bacteria; The bacteria are most commonly
transmitted in contaminated sputum expelled in the
coughs of infected persons, although tuberculosis can
also be caused by contaminated milk from infected
cattle. This sputum may dry and settle in dust that can
contain infective bacteria for a long time.
The first infective exposure with the bacteria is called a
primary infection.
Mulvihill, Zelman, Holdaway, Tompary, and Raymond
Human Diseases: A Systemic Approach, 6e
Copyright ©2006 by Prentice-Hall, Inc.
Upper Saddle River, New Jersey 07458
All rights reserved.
Pulmonary Tuberculosis
Pathogenesis
The inhaled bacteria infect the lungs and induce a
chronic inflammatory response that leads to necrosis.
The tissue in this site becomes soft and cheese-like,
which is why it is described as a caseous lesion. The
tissue heals with fibrosis and calcification, walling off the
bacteria for months or many years. These lesions are
called tubercles.
During this period, a person may have no symptoms. A
secondary infection occurs when the person is infected
again or when the bacteria escape the walled-off lesions
in the lungs.
Mulvihill, Zelman, Holdaway, Tompary, and Raymond
Human Diseases: A Systemic Approach, 6e
Copyright ©2006 by Prentice-Hall, Inc.
Upper Saddle River, New Jersey 07458
All rights reserved.
Pulmonary Tuberculosis
Pathogenesis (continued)
The bacteria may spread this way when the person’s
resistance is reduced because of stress, infection,
malnutrition, or immuno-deficiency.
During the secondary infection, leukocytes now
recognize the bacteria and mount an attack that leads to
greater necrosis and destruction of lung tissue.
Necrotic tissue, blood, and bacteria may be coughed up.
The bacteria may spread to other organs like the brain,
kidney, and bones. Persons in the secondary stage of
the disease also lose weight and become cachectic; this
is the basis for the classic name for tuberculosis,
consumption.
Mulvihill, Zelman, Holdaway, Tompary, and Raymond
Human Diseases: A Systemic Approach, 6e
Copyright ©2006 by Prentice-Hall, Inc.
Upper Saddle River, New Jersey 07458
All rights reserved.
Screening and Treatment of
Tuberculosis
The treatment for tuberculosis involves antibiotics specially
designed for Mycobacterium species. These drugs may include
rifampin, isoniazid, ethambutol, or others. The drugs must be taken
over an extended period of time for as much as 18 months to ensure
that the bacteria are killed.
Screening for tuberculosis involves the Mantoux skin test in which
antigens from the bacteria are injected beneath the skin. If persons
have been exposed to tuberculosis, they will develop swelling at the
injection site. If persons have positive skin tests, then they may have
their sputum cultured and/or receive a chest x-ray to determine if
there is an active infection.
Tuberculosis is uncommon in much of the U.S., but its incidence has
increased since the 1980s and 1990s. This increase is thought to be
because of the evolution of antibiotic-resistant bacteria and the
increase in people infected with HIV, homeless people, and
immigrants.
Mulvihill, Zelman, Holdaway, Tompary, and Raymond
Human Diseases: A Systemic Approach, 6e
Copyright ©2006 by Prentice-Hall, Inc.
Upper Saddle River, New Jersey 07458
All rights reserved.
Click on the screenshot to view a video on the topic of
tuberculosis.
Mulvihill, Zelman, Holdaway, Tompary, and Raymond
Human Diseases: A Systemic Approach, 6e
Return to Directory
Copyright ©2006 by Prentice-Hall, Inc.
Upper Saddle River, New Jersey 07458
All rights reserved.
Table 9-2 Tuberculosis Increase in the United States.
Mulvihill, Zelman, Holdaway, Tompary, and Raymond
Human Diseases: A Systemic Approach, 6e
Copyright ©2006 by Prentice-Hall, Inc.
Upper Saddle River, New Jersey 07458
All rights reserved.
Bronchogenic Carcinoma
The most common type of lung cancer
Danger of airway obstruction; death results from complications of
obstruction or from the effects of metastatic tumors.
Lung cancer is the leading cause of cancer death among both men
and women. Death from lung cancer includes about 28% of all
cancer deaths. Approximately 80% of lung cancer is related to
cigarette smoking; lung cancer is ten times more common in
smokers versus nonsmokers.
Other causes include inhalation of carcinogens (cancer-causing
agents) which may be an occupational hazard among workers who
are constantly exposed to air pollution, exhaust gases, and industrial
fumes.
The great danger in bronchogenic carcinoma is blockage of the
airway by the malignant tumor as it grows into the lumen of the
bronchus. The affected part of the lung collapses for lack of air.
Mulvihill, Zelman, Holdaway, Tompary, and Raymond
Human Diseases: A Systemic Approach, 6e
Copyright ©2006 by Prentice-Hall, Inc.
Upper Saddle River, New Jersey 07458
All rights reserved.
Figure 9-7: Carcinoma of the lung (large white area).
(Courtesy of Dr. David R. Duffell)
Mulvihill, Zelman, Holdaway, Tompary, and Raymond
Human Diseases: A Systemic Approach, 6e
Copyright ©2006 by Prentice-Hall, Inc.
Upper Saddle River, New Jersey 07458
All rights reserved.
Symptoms and Treatment of
Bronchogenic Carcinoma
The symptoms or signs of early stage lung cancer may be
undetected, but later there is a persistent cough and hemoptysis.
The blood in the sputum results from the erosion of blood vessels by
the growing malignancy.
Anorexia, weight loss, and weakness accompany the disease. The
poor oxygenation of the blood explains the generalized weakness.
Symptoms include difficulty in breathing caused by the obstructed
airway.
Symptoms develop late in the disease so prevention and early
detection are essential.
Diagnosis of lung cancer is made from a biopsy of the tumor,
detecting cancer cells in the sputum, or washings from the
bronchoscopy examination.
Treatment may be surgery, radiation, or chemotherapy, depending
on the particular tumor. In addition to primary carcinoma of the
lungs, the lungs are a frequent site of metastases from the breast,
GI tract, female reproductive system, and kidneys. Average age for
diagnosing lung cancer is age 60.
Mulvihill, Zelman, Holdaway, Tompary, and Raymond
Human Diseases: A Systemic Approach, 6e
Copyright ©2006 by Prentice-Hall, Inc.
Upper Saddle River, New Jersey 07458
All rights reserved.
Cystic Fibrosis
A disease that affects all the exocrine glands of the
body, the glands of external secretion
Exocrine glands secrete mucus, perspiration, and
digestive enzymes.
The abnormality in cystic fibrosis is excessively viscous
mucus secretion. Cystic fibrosis is a hereditary disease
affecting young children. It is transmitted through a
recessive gene carried by each parent.
Before the disease was understood, the mortality rate of
afflicted children was extremely high. The most serious
manifestation of cystic fibrosis is in the respiratory
system. The trachea and bronchi secrete thick mucus
and, as it accumulates, the air passageway is blocked.
Mulvihill, Zelman, Holdaway, Tompary, and Raymond
Human Diseases: A Systemic Approach, 6e
Copyright ©2006 by Prentice-Hall, Inc.
Upper Saddle River, New Jersey 07458
All rights reserved.
Symptoms of Cystic Fibrosis
Wheezing, persistent cough, and thick sputum; the child
experiences difficulty in breathing because of the blocked airways.
The child is particularly susceptible to respiratory infections due to
the abnormal mucosal lining of the respiratory tract.
Normally, bacteria are carried away by mucosal secretions, but in
cystic fibrosis, the bacteria adhere to the sticky mucus.
The stationary secretions serve as a breeding ground for bacteria.
Bronchiectasis (weakened and dilated bronchial tubing) is a
common complication of cystic fibrosis.
Lung collapse can result from the inability to inflate them, and most
deaths occur as a result of respiratory failure. Not only are mucussecreting glands affected, the sweat glands are affected as well.
The child perspires excessively and loses large amounts of salt.
Susceptibility to heat exhaustion is a result. This abnormal excretion
of salt is the basis for the test that confirms cystic fibrosis.
Mulvihill, Zelman, Holdaway, Tompary, and Raymond
Human Diseases: A Systemic Approach, 6e
Copyright ©2006 by Prentice-Hall, Inc.
Upper Saddle River, New Jersey 07458
All rights reserved.
Click on the screenshot to view a video on the topic of
cystic fibrosis.
Mulvihill, Zelman, Holdaway, Tompary, and Raymond
Human Diseases: A Systemic Approach, 6e
Return to Directory
Copyright ©2006 by Prentice-Hall, Inc.
Upper Saddle River, New Jersey 07458
All rights reserved.
Table 9-3 Complications of cystic fibrosis
Mulvihill, Zelman, Holdaway, Tompary, and Raymond
Human Diseases: A Systemic Approach, 6e
Copyright ©2006 by Prentice-Hall, Inc.
Upper Saddle River, New Jersey 07458
All rights reserved.
Age Related Respiratory Disorders
Infants and youngsters may be spared some respiratory diseases
like diphtheria and pertussis (whooping cough) by vaccine (DPT)
injections.
When young children develop asthma they may tend to outgrow it,
but others who acquire asthma later tend to suffer its effects many
years.
For the elderly, deterioration of soft elastic tissue, which depresses
the lungs’ ability to inflate and deflate properly, is a concern.
– Muscles, like intercostals found in the rib cage, are less able to respond
and arthritic joints interfere with a smooth breathing action.
– There is usually some degree of emphysema in individuals 50–70 years
of age. On average one square foot of the respiratory membrane is lost
each year after age 30.
Mulvihill, Zelman, Holdaway, Tompary, and Raymond
Human Diseases: A Systemic Approach, 6e
Copyright ©2006 by Prentice-Hall, Inc.
Upper Saddle River, New Jersey 07458
All rights reserved.
Diagnostic Procedures
Bronchoscopy, chest x-rays, and, when warranted, fluoroscopy,
which permits visualization of the lungs and diaphragm during
respiration
Computerized tomography, also called a CT scan, augments chest
x-rays: a series of exposed films visualize lung tissue at different
depths
Arterial blood gas analysis evaluates gas exchange, oxygen for
carbon dioxide, blood pH, thus indicating respiratory function.
Sputum examination is helpful in the evaluation of pneumonias and
suspected malignancies.
Gram-stained smears and cultures are useful in identifying causative
organisms, determining proper antibiotic treatment, and diagnosing
tuberculosis and fungal lung infections.
Spirometry measures changes in gas volume in the lungs,
determining ventilation capacity and flow rate.
Mulvihill, Zelman, Holdaway, Tompary, and Raymond
Human Diseases: A Systemic Approach, 6e
Copyright ©2006 by Prentice-Hall, Inc.
Upper Saddle River, New Jersey 07458
All rights reserved.
Click on the screenshot to view a video on the topic of
spirometry.
Mulvihill, Zelman, Holdaway, Tompary, and Raymond
Human Diseases: A Systemic Approach, 6e
Return to Directory
Copyright ©2006 by Prentice-Hall, Inc.
Upper Saddle River, New Jersey 07458
All rights reserved.