Dr. Ross Walker's Presenation

MCCQE Part II
Preparing for the MCCQE Part II
Things you should know ….
But were afraid to ask!
OR
Couldn’t bother preparing for!
MCCQE Part II
Overview of exam structure
Ross Walker
Exam preparation and stress management
Mala Joneja
Practical tips and personal experience
Aaron Aggarwal
MCCQE Part II
Why?
• Deterioration in Queen’s Resident performance over the past 4 years (2004 – 2008)
• From top cohort of pass rates to last (16 th )!
• Decrease in the pass rate from 97% to 87%!
• Ranking of 5 th place in 2004 but last place in 2004
• Consistent performance until 2004
• Equally poor performance across all Programs!
• You may not think this exam is important BUT it’s too expansive to have to do it more than once!
MCCQE Part II
• Three (3) hour OSCE
• The questions will be in the domains of Medicine,
Surgery, Obstetrics & Gynecology, Paediatrics &
Psychiatry.
• Preventative Medicine and Community Health will be incorporated into some of the stations.
• MCC Objectives are exhaustive and should be reviewed at “www.mcc.ca/Objective”
MCCQE Part II
• The OSCE is made up of a series of 10 minute stations with short breaks between stations
• The exam is made up of 10 minute couplet stations and 10 minute history or physical stations
• Couplet stations consist of a 5 minute clinical encounter followed by a 5 minute post-encounter probe (PEP)
• The PEP is a written station;
– DDx, interpret test results, write orders or prescriptons, etc.
MCCQE Part II
• 10 minute stations are usually history taking or physical examination stations.
• There is usually a oral question asked by the examiner at the 9 minute mark.
• There are examples of all of these stations on the
MCC website.
Couplet History Taking
This is a 5 minute station with 5 minute PEP
• What the candidate reads
• Candidate’s Instructions;
• Luc Léger, 59 years old, presents to your office complaining of jaundice.
In the next 5 minutes, obtain a focused and relevant history.
At the next station, you will be asked to answer questions about this patient.
Couplet History Taking
• What the examiner completes
• Examiner’s Checklist
Fill in the bubble for each item completed satisfactorily
• 1.Elicits onset/duration
• 2.Elicits progression
• 3.Elicits associated symptoms
– dark urine
– pain
– color of stool
– fever
Couplet History Taking
• 4.Elicits risk factors
– previous exposure to hepatitis
– recent blood transfusion
– intravenous drug use
– foreign travel
• 5.Elicits an alcohol use history
• 6.Conducts a review of systems
– skin
– gastrointestinal
– weight loss
– change in appetite
Couplet History Taking
• Examiner asked to judge performance as
Satisfactory (borderline/good/excellent) or
Unsatisfactory (borderline/poor/inferior)
– This is a global rating
– If unsatisfactory there are several reasons
• Inadequate medical knowledge
• Could not focus
• Poor communication/interpersonal skills
• Potential harm to patient
• Dangerous act
Post-encounter Probe (PEP)
• What the candidate receives (5 minutes to write this answer)
• Post-Encounter Probe
• Q1. The abdominal examination of Luc Léger revealed no organ enlargement, no masses and no tenderness. What radiologic investigation would you first order to help discriminate the cause of the jaundice?
1.______________________________________________________
•
Q2. If the investigations revealed that this patient likely had a post-hepatic obstruction, what are the two principal diagnostic considerations?
•
1.____________________________________________________
•
2.____________________________________________________
• Q3. What radiologic procedure would you consider to elucidate the level and nature of the obstruction?
1.______________________________________________________
• Q4. If this patient were found to have a cancer localized to the ampulla of vater, what single treatment would you recommend?
1.______________________________________________________
Post-encounter Probe (PEP)
•
•
•
•
•
•
•
•
•
•
•
•
•
•
•
•
•
What the post-encounter probe marker receives
Answer Key
Q1.
The abdominal examination of Luc Léger revealed no organ enlargement, no masses and no tenderness. What radiologic investigation would you first order to help discriminate the cause of the jaundice?
Score
A1. Abdominal (liver) ultrasound 4
Endoscopic retrograde cholangiopancreatography (ERCP) 2
Maximum 4
Q2.
If the investigations revealed that this patient likely had a post-hepatic obstruction, what are the two principal diagnostic considerations?
Score
A2.
Pancreatic (periampullary) cancer 2
Choledocholithiasis 2
Gallstones 1
Maximum4
Q3.
What radiologic procedure would you consider to elucidate the level and nature of the obstruction?
Score
A3.
Endoscopic retrograde cholangiopancreatography (ERCP)4
Percutaneous trans-hepatic cholangiogram (PTC)4
Computed tomography (CT) scan1
Score
A4.
Hida scan (biliary) 0
Liver scan (Technetium 99M labeled sulphur colloid)0
Maximum4
Q4.
If this patient were found to have a cancer localized to the ampulla of vater, what single treatment would you recommend?
Whipple procedure (pancreatic-duodenectomy) 4
Biliary bypass 2
Excision 1
Chemotherapy 0
Radiotherapy 0
No treatment 0
Maximum 4
Couplet Physical Examination
• What the candidate reads
• Candidate’s Instructions
Joseph Trans, 12 years old, has been brought to your office with a history of right hip pain which occasionally radiates to the knee.
• In the next 5 minutes, conduct a focused and relevant physical examination.
• As you proceed, explain to the examiner what you are doing and describe any findings.
At the next station, you will be asked to answer questions about this patient.
Couplet Physical Examination
• Examiner’s Checklist
Fill in the bubble for each item completed satisfactorily
• 1 Observes patient walking
• 2 Examines stance - looks at leg lengths and measures
- checks for Trendelenburg sign
[standing on each leg alternately]
• 3 Examines hips - palpation
- flexion
- extension [patient on side or front]
- internal rotation
- external rotation
- abduction
• 4.Examines knees - palpation
- flexion
Couplet Physical Examination
• Did the candidate respond satisfactorily to the needs/problem(s) presented by this patient?
• If unsatisfactory, please specify why:
(For items 4-6, please explain below)
• Satisfactory - Borderline
- Good
- Excellent
• Unsatisfactory - Borderline
- Poor
- Inferior
• Inadequate medical knowledge and/or provided misinformation
• Could not focus in on this patient's problem
• Demonstrated poor communication and/or interpersonal skills
• Actions taken may harm this patient
• Actions taken may be imminently dangerous to this patient
• Other
• Do you have concerns regarding this candidate's ethical and/or professional behavior?
Yes (please specify) No
Couplet Physical Examination PEP
• What the candidate receives
• Post-Encounter Probe
• Q1. Examine the antero-posterior / frog x-ray of both hips of this patient. List the abnormalities, if any. If normal, state so.
_(Multiple Answers allowed)___________________________
• Q2. What is the most likely diagnosis?
1. __(one answer only!)_______________________________
• Q3. What is the appropriate management of this patient?
__(Multiple answers allowed)__________________________
Couplet Physical Examination PEP
•
•
•
•
•
•
•
What the Post-Encounter Probe marker receives
Answer Key
Candidates are provided with the antero-posterior / frog x-ray of both hips for this patient.
Q1. Examine the antero-posterio / frog x-ray of both hips of this patient. List the abnormalities, if any. If normal, state so.
A1.
Posterior inferior slip of epiphysis of metaphysis 4
Slipped epiphysis 3
Mention made in any way of opposite side (bilateral approx. 50% in this condition) 1
Abnormality of the hip 1
Maximum 4
Q2.What is the most likely diagnosis?
A2.
Slipped epiphysis OR slipped capital femoral epiphysis 4
Arthritis 1
Septic hip 0
Trochanteric bursitis 0
Tendinitis 0
LeggCalvé-Perthes 0
Maximum 4
Q3. What is the appropriate management of this patient?
A3. Medication OR urgent referral to orthopedic surgeon within 1 week 3
Crutches until sees orthopedic surgeon 1
Elective referral to orthopedic surgeon 0
Decrease activity, stop gym before consultation 0
Anti-inflammatory medication only 0
Maximum 3
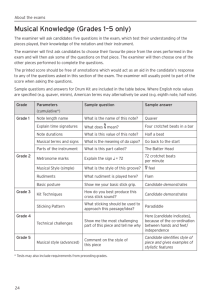
Ten (10) minute history station
• What the candidate reads
• Candidate’s Instructions
• Julia Russo, 65 years old, has come alone to your office with the following complaint: "I just can't cope. Everything seems to be going wrong." She brought with her a note from her son which she gave to your receptionist
(see below).
• In the next 10 minutes, complete a focused history and mental status examination.
•
Dear Doctor,
My mother is no longer able to manage herself and her affairs. She makes frequent financial mistakes such as not paying her bills, getting overdrawn at the bank, and hoarding money in her home. The bank manager is very concerned and so are we. She is not herself. She seems sad and irritable.
She does not remember much of what we, or others tell her. We are afraid that she is not safe at home and should not be living on her own.
Thank you for your help.
Oliver Russo
Office: 222-9999
Ten (10) minute history station
•
•
•
•
•
•
•
•
•
•
•
What the examiner completes
Examiner’s Checklist - Fill in the bubble for each item completed satisfactorily
1. Elicits - onset/duration
- memory
2. Elicits - mood
- anxiety
3. Asks about changes in daily activities
4. Asks about
- drug use
- alcohol use
5. Elicits dangerousness/risk factors
- suicide potential
- getting lost
- financial management
6. Elicits constitutional signs and symptoms
- energy
- sleep
- appetite
- weight gain/loss
7. Conducts mental status testing
- orientation:
- time
- person
- place
- memory:
- concentration
8. Elicits family history of senility
9. Elicits past medical history
- immediate
- recent
- long term
Ten (10) minute history station
• Did the candidate respond satisfactorily to the needs/problem(s) presented by this patient? If unsatisfactory, please specify why:
Satisfactory - Borderline
- Good
- Excellent
• Unsatisfactory - Borderline
- Poor
•
- Inferior
• Inadequate medical knowledge and/or provided misinformation
• Could not focus in on this patient's problem
• Demonstrated poor communication and/or interpersonal skills
• Actions taken may harm this patient
• Actions taken may be imminently dangerous to this patient
• Other
• Do you have concerns regarding this candidate's ethical and/or professional behavior?
• Yes (please specify) No
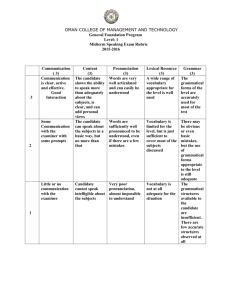
Rating Scales
• Each station will have an associated interaction rating scale;
– Ethical Conduct (inappropriate – effective)
– Compliance optimization (negative–highly effective
– Facilitates Informed Decision making (deceptiveclear, organized and effective)
– Responds to Questions (ignores-empathetic)
– Organized Physical Exam (not attemptedpurposeful)
– Attentive to patient comfort (NOT-consistent)
– Patient Relationship (None-at ease with patient)
Common Mistakes
• Not reading the question!
• Asking too many unfocused questions (shotgun)
• Not explaining what you are doing during physical examination stations
– Rectal, vaginal and inguinal exams not allowed
BUT you will not be given credit unless you indicate that you would do them when appropriate.
• Talking too fast and too much – maintain professional courtesy
• Trying to guess what the station is about and not listening to the patient
MCCQE Part II