Paying for Health Care Reform - Physicians for a National Health
advertisement

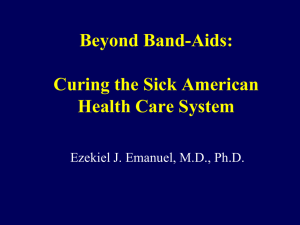
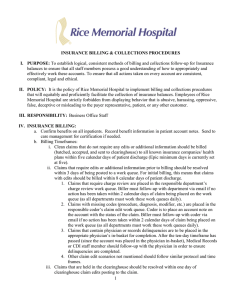
Health Care Reform Post-Election: What is “Realistic”? Leonard Rodberg, PhD Urban Studies Dept., Queens College/CUNY and NY Metro Chapter, Physicians for a National Health Program November 18, 2008 len@infoshare.org Parasitical middleman American Way cartoon Wall Street Bailout NYTimes Editorial re international comparisons November 18, 2008 Editorial The Wrong Place to Be Chronically Ill Chronically ill Americans suffer far worse care than their counterparts in seven other industrial nations, according to a new study by the Commonwealth Fund…the latest telling evidence that the dysfunctional American health care system badly needs reform. Three Possibilities for the Non-elderly Non-poor • Private insurance • Private insurance with a public option • Public plan/national health program McCain/Wyden-Bennett: Individual Responsibility “You’re On Your Own” • End employer-based insurance by eliminating the employers’ tax deduction for health insurance • Make individuals more cost-conscious consumers • Use tax credits to help low-income individuals • Control costs through market competition No evidence - “Faith-based health policy” Will Mom & Pop do better than GM and the Federal Government (FEHBP)? “Mainstream”Mandate/ Building Blocks Model • • • • • • Obama/Baucus/Ted Kennedy(?) Commonwealth/Hacker/HCAN The problem : Too many uninsured The solution: Everyone should buy insurance Employers should contribute or offer insurance Continued reliance on private insurance, with the option of a public plan “Keep what you have” Expansion of Medicaid/SCHIP No regulation of insurance company premiums or reimbursement and denial practices The Mandate/Building Blocks Model Won’t Work • It won’t lead to 100% coverage • Private health insurance will be a continuing consumers nightmare (copay, deductible, denials) • Doesn’t address widespread underinsurance • Increases cost of the system by billions of dollars • Many payers remain, so the savings from a single funding source can’t be achieved. • There is no way to control costs. It treats the symptom – the uninsured – while ignoring the disease – private insurance. Even Its Supporters Recognize the Superiority of Single Payer “Compared to a Medicare-for-All approach, the Building Blocks framework would not achieve the simplicity, consolidated risk, administrative overhead, and provider payment net savings of covering nearly everyone through Medicare.” -- Cathy Schoen, Karen Davis and Sara R. Collins, “Building Blocks For Reform: Achieving Universal Coverage with Private and Public Group Health Insurance, Health Affairs, May-June 2008 Conyers/Kucinich/et al Expanded and Improved Medicare for All “single payer national health insurance” HR 676 • Automatic enrollment - everyone receives a card assuring payment for all needed care • Doctors and hospitals remain independent, negotiate fees, budgets with public agency • Public agency processes and pays bills • Financed through progressive taxes Where the Private Insurance Dollar Goes: Nearly 30% for Billing Allocation of Spending for Hospital and Physician Care Paid through Private Insurers Other Insurer Costs and Profit 11% Insurer Billing 8% Hospital Billing 4% Medical Care 62% Physician Billing 5% Medical Care Administration 10% Source: James G. Kahn et al, The Cost of Health Insurance Administration in California: Estimates for Insurers, Physicians, and Hospitals, Health Affairs, 2005, and private communication, 2008 Covering Everyone and Saving Money through Single Payer Additional costs Covering the uninsured and poorly-insured Elimination of cost-sharing and co-pays Total Costs Savings Reduced hospital administrative costs Reduced physician office costs Reduced insurance administrative costs Bulk purchasing of drugs & equipment Primary care emphasis & reduce fraud Total Savings $B +6.4% 134 +5.1% 107 +11.5% 241 -1.9% -21 -3.6% -76 -5.3% -111 -2.8% -59 -2.2% -46 -15.8% -313 Source: Health Care for All Californians Plan, Lewin Group, January 2005 Obama on Single Payer 2003 “I happen to be a proponent of a single payer universal health care program. I see no reason why the United States of America, the wealthiest country in the history of the world, cannot provide basic health insurance to everybody. A single payer health care plan, a universal health care plan, that’s what I’d like to see. We may not get there immediately, because first we have to take back the White House, the Senate, and the House.” -- June 30, 2003. Obama on Single Payer 2007 "A single-payer system--a government-managed system like Canada's, which disconnects health insurance from employment--would probably make sense. But we've got all these legacy systems in place, and managing the transition, as well as adjusting the culture to a different system, would be difficult to pull off. So we may need a system that's not so disruptive that people feel like suddenly what they've known for most of their lives is thrown by the wayside." -- The New Yorker, May 7, 2007 Obama on Single Payer 2008 "If I were designing a system from scratch, I'd probably set up a single-payer system. But the problem is, we're not starting from scratch. Making that transition in a rapid way would be very difficult. You’ve got a whole system of institutions that have been set up. A lot of people work for insurance companies, a lot of people work for HMOs. So my attitude is: People don’t have time to wait. They need relief now. Let’s build up the system we’ve got, let’s make it more efficient. Maybe over time — as we make the system more efficient and everybody is covered — we’ll decide that there are other ways for us to provide care more effectively.” -- August 18, 2008 A FALSE POLICY CHOICE Assertion: “Let’s first cover everybody. Then we can deal with the system’s inefficiencies.” Fact: We will never have enough money to provide everyone with decent coverage until we eliminate the principal sources of waste and inadequate coverage. Why Health Care Is On the Agenda: Escalating Cost Average Annual Premiums for Single and Family Coverage, 1999-2008 $2,196 $2,471* 2000 Family Coverage $6,438* $2,689* $7,061* $3,083* 2002 Single Coverage $5,791 $8,003* $3,383* $9,068* $3,695* 2004 $9,950* $4,024* $10,880* $4,242* 2006 $11,480* $4,479* $12,106* $4,704* 2008 $0 $2,000 $4,000 $6,000 $12,680* $8,000 $10,000 * Estimate is statistically different from estimate for the previous year shown (p<.05). Source: Kaiser/HRET Survey of Employer-Sponsored Health Benefits, 1999-2008. $12,000 $14,000 The Growth in Cost Must be Addressed if Any Plan is to Succeed Single payer offers real tools to contain costs – • Budgeting, especially for hospitals • Investment planning • Emphasis on primary care and coordination of care Mandate plans offer only hopes – • Computerization • Chronic disease management • Insurance company competition There is no data or experience to suggest that these will cut costs or limit the rise in cost. The Bottom Line The Mandate/Building Block model will – • • • • • Make the world’s most costly health system even costlier. Not improve insurance coverage for the average person. Not make affordable insurance available. Not address the problem of underinsurance. Not contain the continuing growth in cost. In other words, they won’t work! Only national health insurance will – • Cover everyone for comprehensive services. • Cost no more than we are now spending. • Provide mechanisms for containing the growth in cost. Leadership Conference for Guaranteed Health Care – The National Single Payer Coalition • Meeting in Washington, DC Nov. 10-11 at AFL-CIO Headquarters, but limited involvement of labor • Sponsors: California Nurses Association, PNHP, Healthcare NOW, Progressive Democrats of America, faith groups • Health care reform = Economic and moral issue • Media campaign: Need to “Start from Scratch” • Congressional visits “the train is moving” Strategic Questions in this Post-election Period • Should “mainstream” health reform be passed quickly, perhaps providing an economic stimulus? • Should we oppose early action, urging limited reforms (SCHIP, Medicare reforms, IT) while the country engages in a lengthy debate towards real reform? • Our Rodney Dangerfield problem: How do we get respect and visibility for the single payer option? • How do we mobilize latent majority public support? Will We Get Real Health Care Reform Before the Premium Takes All our Income? Today Source: American Family Physician, November 14, 2005 Physicians for a National Health Program For more information: www.pnhp.org www.pnhpnymetro.org