PPT

National Training Program – RO V & RO VII
St. Louis, August 10-11, 2015
Special Needs Plans
Medicare SNPs are a type of Medicare Advantage Plan
(like an HMO or PPO). Medicare SNPs limit membership to people with specific diseases or characteristics, and tailor their benefits, provider choices, and drug formularies to best meet the specific needs of the groups they serve.
1
SNP Legislative History Highlights
• Medicare Modernization Act (MMA) of 2003 – created SNPs
– Dual SNPs (D-SNPs)
– Chronic Care SNPs (C-SNPs)
– Institutional SNPs (I-SNPs)
• State Children's Health Insurance Program (SCHIP) Extension Act of 2007– extended SNPs through Dec 2009, but placed moratorium on approving new SNPs
• Medicare Improvements for Patients and Providers Act (MIPPA) of 2008 – lifted moratorium, but added requirement of state contract for new or expanding D-SNPs; required panel of experts to approve clinical conditions for C-SNPs; first required Model of Care (MOC) approval process
• Affordable Care Act (ACA) of 2010 – required approval of MOC’s by National
Committee for Quality Assurance (NCQA), and extended SNPs through 2012
• Relief Act of 2012 (i.e., “Fiscal Cliff legislation”) – extends SNPs through
January 2015
2
SNP Basics
• MMA of 2003 created SNPs
• SNPs are Medicare Advantage (MA) plans authorized by the MMA to allow
Medicare Advantage Organizations (MAOs) to target enrollment to 3 specific vulnerable populations:
– Beneficiaries who are dually eligible for Medicare and Medicaid (D-SNPs)
– Beneficiaries who live in long-term care institutions (or would otherwise require an institutional level of care) (I-SNPs or I-SNP equivalent)
– Beneficiaries who have certain severe and disabling chronic conditions (C-
SNPs)
• SNPs focus on care management of the targeted beneficiary population
– SNPs are required to develop a Model of Care (MOC)
– SNPs are required to perform a health risk assessment (HRAT) at time of enrollment, annually, and when change in health status
3
SNP - Enrollment Basics
• SNPs may limit enrollment to beneficiaries with special needs (beneficiary must qualify) – all other MA’s must be open to all Medicare beneficiaries
• Beneficiaries may enroll in SNPs at times other than the Annual
Enrollment Period (AEP)
• SNPs are required to cover Part A and Part B services AND Part D
• Any SNP type may request an End Stage Renal Disease (ESRD) waiver as part of its application
• SNPs are offered by MA’s at plan benefit package level
4
SNP Provider Network
• Medicare SNP network used for hospitals and doctors
• Require Primary Care Doctor or Care Coordinator
• Referral needed for Specialists
• Except emergency or urgent care, such as care you get for a sudden illness or injury that needs medical care right away, or if you have End-Stage Renal Disease (ESRD) and need out-ofarea dialysis
• Medicare SNPs typically have specialists in the diseases or conditions that affect their members.
5
SNP Eligibility
1) people who live in certain institutions (like a nursing home) or who require nursing care at home
2) people who are eligible for both Medicare and Medicaid
3) people who have specific chronic or disabling conditions (like diabetes, End-Stage Renal Disease (ESRD), HIV/AIDS, chronic heart failure, or dementia). Plans may further limit membership
6
SNP Costs
• For duals, most if not all costs for services are covered
• For non-duals, depends on SNP but you'll pay the basic costs of having a
Medicare Advantage plan .
7
Care Coordinators
• Some Medicare SNPs use a care coordinator to help you stay healthy and follow your doctor's orders.
• A care coordinator is someone who helps make sure people get the right care and information.
• A Medicare SNP for people with diabetes might use a care coordinator to help members monitor their blood sugar, follow their diet, get proper exercise, schedule preventive services (like eye and foot exams), and get the right prescriptions to prevent complications.
• A duals SNP might use a care coordinator to help members access community resources and coordinate their different Medicare and
Medicaid services.
8
Leaving a SNP
• You can stay enrolled in a SNP only if you continue to meet the special conditions served by the plan.
• A duals SNP requires both Medicare and Medicaid eligibility
• The grace period is at least one month long, but plans can choose to have a longer grace period.
• SEP if you lose eligibility for the SNP
• SEP begins with notice of ineligibility, continues during plan’s grace period, and for 2 months after coverage ends.
9
18%
SNP Basics –
Comparing SNP Types
SNP Types
14%
68%
D-SNPs C-SNPs I-SNPs
10
SNP Basics –
Enrollment Compared with MA
12%
2013 SNP Enrollment
Non-SNP Enrollment
(13 million)
SNP Enrollment
(1.7 million)
88%
Total 2013 Enrollment –
14.7 million beneficiaries in MA and SNP plans
11
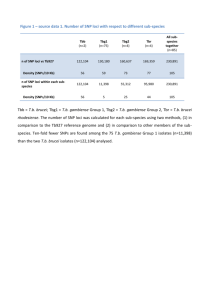
Aggregate SNP Data - July 2015
SNP Type
Chronic condition
Dual-Eligible
Institutional
Totals
Number of
Contracts
52
209
44
305
Number of
Plans
148
336
57
541
Sub Total
Enrollment
326,219
1,705,556
51,074
2,082,849
12
D-SNP Subtypes
• All-Dual – Enrollment includes all types of dual eligibles
• Full-Benefit – Enrollment is limited to individuals eligible for full Medicaid benefits (QMB+ and SLMB+) and other full benefit duals
• Medicare Zero-Cost-share – Enrollment is limited to QMBs-only and
QMB+
• Dual eligible subset – enrolls any eligibility category or combination of categories, as long as specified in State contract.
– Dual eligible subset zero cost-share – Enrollment of individuals other than just
(QMB and QMB+) for whom the State pays Medicare cost-sharing
– Dual eligible subset nonzero cost-share – Enrollment of individuals who pay some part of the Medicare cost-share
13
C-SNP – Basics
• C-SNPs must classify their C-SNP application as:
– One of the 15 CMS-approved chronic conditions including:
• Chronic alcohol & drug abuse
• Auto Immune disorders cancer
• CV-disorders
• CHF
• Dementia
• Diabetes
• ESRD
• End state liver disease
• Severe hematologic disorders
• HIV/AIDS
• Lung disorders
• Disabling mental health conditions
• Neurological disorders
• Stroke
14
Chronic Condition SNPs
• CMS will accept applications with the following five CMS approved multicondition groupings:
– Group 1: Diabetes mellitus and chronic heart failure
– Group 2: Chronic heart failure and cardiovascular disorders
– Group 3: Diabetes mellitus and cardiovascular disorders
– Group 4: Diabetes mellitus, chronic heart failure, and cardiovascular disorders
– Group 5: Stroke and cardiovascular disorders
• Beneficiaries need only to have one of the qualifying conditions for enrollment.
15
I-SNP Types – Basics
• I- SNP – Institutional SNP (3 types)
– I-SNP (Facility) – Enrolls Individuals residing in long term care facilities
– I-SNP (Equivalent) – Enrolls Individuals residing in the
Community but requiring institutional level of care
– I-SNP (Both) – Enrolls Individuals in Institutions & residing in the Community
16
Key Differences Between SNPs and Standard MA Plans
Categories Special Needs Plans Medicare Advantage Plans
Enrollment Must limit enrollment to targeted special needs individuals (duals, chronic/disabling conditions, institutionalized)
Must be open to all
Medicare-eligible beneficiaries
Duals and institutionalized beneficiaries may enroll/disenroll anytime. Chronic care beneficiaries have one-time enrollment option outside AEP
Benefits Must offer Part D Rx drug coverage
Lock-in provision with annual open-enrollment period
Part D coverage is voluntary
Marketing May target special needs populations Must include all Medicareeligible beneficiaries in the market area
17
NCQA SNP Performance Analysis
• National Committee Quality Assurance, www.ncqa.org
• Non-profit organization that accredits and certifies health care organizations to ensure adherence to health care quality
• Performs SNP Performance Analysis every year for CMS
• Latest report in 2014 compares 2011-2013 SNP data
• As of 2012, all SNPs Model of Care must be approved by
NCQA
18
S&P Key Findings
• Wide range of performance within and across S&P measures
• SNPs showed improvement on majority of measures that did not change between 2011 and 2012
• D-SNPs compose majority of plans and enrollment, so drive overall performance results
– 262 of 394 SNPs (66.5%)
– 1.12 million enrollees of 1.35 million total SNP members
(83%)
S&P Key Findings Continued
• I-SNPs tend to outperform other SNP types
– Smallest # of plans (58), overall enrollment
(46,000) and avg. # of members (793)
– Dominated by a few organizations
• 5 organizations comprise nearly ¾ of I-SNP plans
• One organization has >40% of the I-SNP market: their results drive overall I-SNP performance
• C-SNPs had lowest performance across all measures
Model of Care Results-SNPs
• SNP Results
– CMS raised the bar in 2013—One cure; only for SNPs scoring
<70% after initial review (receive 1-year approval)
– Many SNPs submitted same/similar MOC as in previous years
– 3-year approval (85+%): 149 plans
– 2-year approval (75%-84%): 20 plans
– 1-year approval (70%-74%): includes cure 1 plan scores): 6 plans
– Not approved (<70%): 2 plans
– Withdrew application: 33
Results for SNPs
Final Score by SNP Type and MOC Element
4,00
3,50
3,00
2,50
2,00
1,50
1,00
0,50
0,00
MOC 1 MOC 2 MOC 3 MOC 4 MOC 5 MOC 6 MOC 7 MOC 8 MOC 9 MOC10 MOC11
Final Score for Chronics
Final Score for Duals
Final Score for Institutionals
SNP HEDIS 2013 Overview
• 415 SNPs Eligible to Report (>30 members)
• 40 HEDIS measures reported
– 28 clinical performance measures
– 4 board certification measures
– 8 utilization measures
• Audited by NCQA-Certified HEDIS Compliance Auditors
• Reflects care provided in 2012
• Compares performance among SNPs and to non-SNP MA plans
Key Findings
• Steady improvement from 2011-2013
• Performance gap between SNP and MA plans continues to narrow
– 6 measures-SNP performance is higher
– 8 measures-no statistically significant difference in performance
– 13 measures – SNP performance is lower
• Performance differences among SNP types
– D-SNPs-most measures with statistically significant improvement from 2012-2013