(audio with pics)
advertisement
")
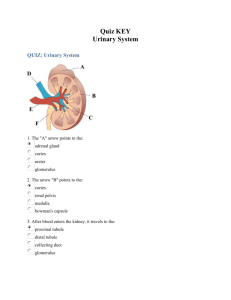
Module 11: Renal 11 February 2010 Marivic V. Bustos, MD Histology of the Renal System - Know where a structure is located because if you know what to look for in the cortex/medullar, you’ll not be confused - Medullary rays – do not look for it in the gross specimen, only in histologic slides Arcuate – found in the arch of the corticomedullary junction Interlobar – side of medullary pyramid o Vein – bigger lumen o Artery – smaller lumen In the gross anatomy, it’s not wise to ask interlobar and arcuate, difficult to differentiate. It can be asked in Histology. OUTLINE Don’t be alarmed! It’s long because of the pictures - I. URINARY SYSTEM A. Nephron 1. Renal Corpuscle Uriniferous Tubules – old term for the Renal Corpuscle; refer to the NEPHRON and collecting tubules Other Names: nephrons - excretory collecting tubules ureter - collecting system Nephron – functional unit of the kidney; concerned with urine formation Includes corpuscle, Proximal Convoluted Tubule (PCT), Henle’s Loop, Distal Convoluted Tubule (DCT) - Nephrons There are 2 kinds o Juxtamedullar – makes up 1/7 of the cortex o Cortical – makes up 6/7; up the cortex o Both participates in filtration of blood, absorption and secretion “Convoluted portion” also refer to PCT and DCT “Straight portions” refer to Henle’s Loop Kidney (monkey) Jones' methenamine silver AA arcuate artery Ai interlobar artery AV arcuate vein C calyx Cx cortex G glomerulus IA interlobular artery MR medullary ray P renal pelvis RC renal corpuscles RP renal papilla T tubule U ureter V interlobular vein Figure 1. Anatomic and Histologic Picture Cortex - Straight layer of in the gross anatomy of the kidney Conains renal corpuscle Medullary Pyramid Collecting tubules Henle’s Loop Some Henle’s loop and collecting tubules in the cortex, but I’m going to ask them in the medulla so you’ll be sure about the structures Group 01 Figure 2. Histologic Scan of the Kidney 2. - Renal Corpuscle Try to differentiate the renal corpuscles (ONLY found in the CORTEX), and the medullary pyramid Page 1 of 8 BATCH 2014 HISTOLOGY OF THE URINARY SYSTEM - Absence of corpuscles means you are in looking at the Renal Pyramid Arcuate Artery - Vessel between the cortex and medulla Figure 3. Renal Corpuscle in the Renal Cortex Renal Corpuscle A afferent- arteriole BC Bowman's capsule BS Bowman's space C glomerular - capillary E endothelial cell GBM glomerular basement membrane I interstitium M mesangium N mesangial cell nucleus P podocyte PCT proximal convoluted tubule S squamous cell - - BS - BC Physiology: Afferent arteriole comes from the interlobar artery enters corpuscle divides into 4 branches forms several capillaries forming the GLOMEROLUS Thus, glomerulus is made of cup of capillaries, where blood enters to be filtered Glomerular capsule divides into two: o Parietal layer – external layer; will form the outer limit of renal corpuscle o Visceral layer – envelops the glomerulus; this layer cannot be differentiated from glomerulus in the light microscope Figure 4. Renal Cortex showing parts of two renal corpuscles, macula densa, and distal and proximal convoluted tubules. Arrows - Collagen type IV of the basement membrane of the glomerular capillaries Arrowheads - collagen of the parietal layer of Bowman's capsule and the basal membrane of a distal tubule are shown Group 09 - Bowman’s Space – receives filtered fluid from the glomerulus Vascular pole o Area where afferent and efferent can be found o But afferent and efferent are difficult to see through the light microscope o Once parietal and visceral meet = area of vascular pole Urinary pole o If you have found the vascular pole, the opposite of it is the urinary pole (forms an indention at the upper part of the corpuscle but not very clear in all specimens) o Break in the parietal layer becomes continuous as PCT, that’s your urinary pole o Thus, what is brought to the Bowman’s space will be brought to PCT Tips for the exam: When the whole structure is bracketed – that’s your renal corpuscle But when pointed, or there’s an arrow – that’s your glomerulus Glomerulus + BowmanS capsule = renal corpuscle Parietal layer – where you see the Bowman’s capsule It’s not right to write Bowman’s capsule – write parietal layer of Bowman’s capsule since the capsule and the parietal is not that differentiated - Bowman’s capsule As the parietal layer approachesthe vascular polem, the simple squamous epithelium becomes simple cuboidal Visceral Layer o Cannot be well-delineated o Envelopes glomerulus o Cannot be separated from glomerulus using the microscope o No epithelium but visceral layer is made of cells called Podocytes o Structure: Cell body of podocyte foot podocytes/foot processes/primary process several finger like extensions, secondary processes or pedicles. o Pedicles interdigitate with other pedicles, forming spaces in between called filtration pits (spaces found between the pedicles) o In between endothelium of capillaries and filtration pits are your Glomerular Basement membrane, serving as filtration barrier composed of 2 layers Page 2 of 8 BATCH 2014 HISTOLOGY OF THE URINARY SYSTEM Lamina densa- acts as physical barrier, molecules of >10nm in diameter cannot pass through Lamina rara – negatively charged; anionic; acts as negative barrier with regards to substances that are negatively charged like proteins except albumin which can pass through In the urinalysis, you can only find <5 WBC, RBC and a trace of protein Problem in this membrane: substances that should not pass through this barrier like in patients with glomerular nephritis or neprhotic syndrome heavy proteinuria (heavy protein in the urine); protein normally does not pass through FILTRATION Barrier (Berns, Scribe na to) Other structures in the nephron, near the corpuscle Mesangial (means “between capillaries”) o Found in glomerulus o Angiotensin II is for Vasoconstriction decreased blood flow o NF – produced in the cardiac atrial cells; a vasodilator; opposite of angiotensin II; favors blood filtration o Thus, depends on the needs of the body a hormone is released appropriately o Macrophage for substances trapped inside the glomerulus Ex: Mesangial hypercellularity – there’s inflammation inside the glomerulus o Dr. Bustos: Honestly, I don’t know where we can find the mesangial cells it’s not even pointed in the book. But renal pathologists can identify. o 2-3 cells should be between renal capillaries Figure 5. Schematic representation of a glomerular capillary with the visceral layer of Bowman's capsule (formed by podocytes). Figure 7. Mesangial Cells 1 2 1 P 2 Figure 6 Electron Micrograph P – Podocytes; 1 – primary process; 2 – secondary process/pedicels; arrows – filtration pits Group 09 Uriniferous Tubules Blood filtration o Afferent arteriole glomerulus (filtered substances pass through) Bowman’s space PCT PCT Found only in the CORTEX (!!!) Seen near the renal corpuscles; surrounding…. Lined by simple cuboidal or low columnar WITH BRUSH BORDER Function: increased surface area for absorption; numerous in PCT because it needs toABSORB! o About 85% of fluid and Na is reabsorbed in PCT o Reabsorbed any AA and glucose that will pass through Page 3 of 8 BATCH 2014 HISTOLOGY OF THE URINARY SYSTEM o Otherwise, it EXCRETES your creatinine (substances not needed by the body) so it will not accumulate in the body, indicates renal failure Laboratory: Need to Differentiate from DCT - Figure 8. Renal Cortex P- Proximal CT; D – Distal CT; proximal (P) and distal (D) convoluted tubules. Henle’s Loop (refer back to Figure 1) Straight portions of the nephron Abundant in medulla / medullary pyramid Two types of nephrons o Significance: juxtamedullary – important in maintenance of hypertonicity within the medullary pyramid o Compositions: Proximal – 85% Thin descending – 5% thin ascending (juxta) – impermeable to water Thick ascending – transports chloride from tubule to medullary interstitium increased hypertonicity of medullary interstitium Thin loops – NOT found in the cortex o Look for it in the medulary pyramid In the laboratory:Thick ascending and descending – cannot differentiate between the two because they are in cross-section; Looks similar to DCT and PCT; can differentiate from them because Henle’s Loop has no renal corpuscle Thin Loop of Henle – Simple Squamous o In some instances, you can see structures with simple squamous but with RBCs, that’s your vasa recta (a capillary) o Thus, without RBC – that’s your thin loops, o Iif with blood - that’s your vasa recta As thick descending penetrates the cortex, it becomes the DCT Only in the CORTEX! Near renal corpuscle Just like PCT and thick loop of Henle – simple cuboidal epithelium WITHOUT brush border In the presence of vasopressin, they reabsorb some amounts of water Functions are important in Physiology Exam Tips DCT vs PCT is always asked beside the RENAL CORPUSCLE, so you’ll not mistake it as the Thick Loop of Henle DCT and PCT – simple cuboidal epithelium (Berns, eto ata ay nasa table din so you can opt to erase this and highlight na lang yung contents ng table) o PCT – more acidophilic o Brush border function – PCT for majority of reabsorption o DCT – no brush border thus, larger lumen Numerous nuclei, nicely spaced even in the lateral border o PCT – not well delineated Figure 9. Distal convoluted tubules (DCT) Note: absence of brush border. THL: thin portion of Henle's loop Arrowhead: blood capillary Macula Densa As the DCT approaches the vascular pole A portion of DCT actually becomes columnar, closely-packed, appear dark in color Juxtaglomerular cells (JG cells) Near vascular poles, where your a. arteriole, can be modified, named JG Cells Very important because it secretes RENIN (important in conversion of Angiotensinogen to Angiotensin I) Angiotensin II – important in cases of hemorrhage where the body has the converse fluid Aldosterone – secreted from the adrenal cortex DCT Group 09 Page 4 of 8 BATCH 2014 HISTOLOGY OF THE URINARY SYSTEM o o helps reabsorb the sodium and in the process, also reabsorb water fluid retention maintains blood pressure; BUT fluid retention can occur only at a certain time i.e. immediate response of the body to cope with fluid loss Figure 10. Collecting Ducts Figure 10. Note Juxtaglomerular Cells Erythropoietin – produced in the cortical interstitial cells (cells found in between the PCT and DCT) COLLECTING DUCTS More columnar, like the tubules Exam Tips: For the exam, its hard to distinguish Collecting ducts from tubules, you can write either But differentiate from Thick descending loop RENAL INTERSTITIUM Spaces found between the tubules Increased in medulla Erythpoeitin is secreted here Laboratory: No need to identify this! Mahirap hanapin ang afferent and efferent arteriole COLLECTING TUBULES Filtrate from renal corpuscle PCT loop of Henle DCT Collecting tubules Found in the cortex and in the medulla Found in the medullary rays, but more abundant in the medullary pyramid Forms collecting ducts Collecting Ducts As collecting ducts approaches apex of medullary pyramid enlarges Initially lined by simple cuboidal but as it approaches the deep part of medullary pyramid, becomes simple columnar (since they grow bigger) Collecting tubules: Laboratory: Principal and intercalated cells – no need to find in histologic slides ADH –produced in hypothalamus and stored in posterior pituitary Collecting tubules – very sensitive to ADH o I.e. when you’re trapped in the desert, you won’t urinate CALYCES, RENAL PELVIS, URETER, and URINARY BLADDR Grouped together because they are lined with transitional epithelium Also lined by smooth muscle layer Urinary bladder – covered by peritoneum, making up the serosa URETER Figure 11. Ureter Exam Group 09 Page 5 of 8 BATCH 2014 HISTOLOGY OF THE URINARY SYSTEM Tip: Should be able to identify this even if natutulog kayo! It has the distinct stellate-shpaed lumen Middle to lower part of the ureter: muscle layer is complete… - Internal smooth muscle forms internal urethral sphincter It’s above the urogenital diaphragm URINARY BLADDER Serosa: transitional epithelium What is unique about the bladder’s epithelium: varies if full or empty o Empty: 6-8 layers of thickness o Full: 3-4 layer of thickness o Note: Only true for epithelium of urinary bladder, not for ureter and calyces Smooth muscle is called the detrusor muscle Figure 12. Bladder IL – Inner Longitudinal OC – Outer Circular Muscle OL – Outer Longitudinal Muscle A - Adventitia URETHRA Male Lining is still transitional because it is continuous with the bladder As it approaches your external urethral meatus, becomes stratifed squamous non keratinized (Laboratory: no slide for this but you may find it in the penis) Female Close to vagina Lined by stratified (or for some satisfied squamous ) squamous non keratinizing Group 09 Figure 13. Male Urethra EMBRYOLOGY (so you’ll be able to appreciate some abnormalities huhu) Three embryonic stages of kidney o Pronephros o Mesonephros Replaced pronephros o Metanephros Replaced mesonephros Forms the definitive permanent kidney, ONLY IN THIS STAGE Just located in the pelvic region, will ascend by the 8th week of fetal life to lumbar region Becomes functional beyond the 6th week, around 7th to 8th so that urine production starts by 9th week Metanephros o Development: Metanephric mesoderm excretory system Ureteric bud collecting system Urinary bladder is from cloaca urorectal septum divides into urogenital sinus and anorectal canal Urogential sinus urinary bladder and urethra Formation of nephrons – until birth only; after birth, no production o 1-2M per kidney o Begins functioning by the 9th week of fetal life Page 6 of 8 BATCH 2014 HISTOLOGY OF THE URINARY SYSTEM Fetal urine goes to amniotic fluid so that the fetus can also swallow the urine Trivia: The boxer Marquez drinks his own urine (yuuuucccck) Kidneys – may actually be lobated o Disappears because nephrons starts to grow o But lobes do not increase in number Urinary bladder – abdominal organ until 6., 6-12greater pelvis, puberty-lesser pelvis o - - Abnormalities Ectopic kidney o Kidney is trapped in the pelvic area, near pelvic vessels Horsehoe Polycystic kidney o Accumulation of fluid/urine in the cyst o What happens here: failure of union between DCT with collecting tubules thus, urine is formed in the collecting tubule forming a cyst Double collecting system o 2 ureters and 2 renal pelvis Vesico-ureteral reflux o Ureter should be appropriately placed to act as a physiologic valve and prevent reflux o Pathologic: intramural portion of ureter is not inserted well in the mucosa Placement is not that oblique or embedded in the detrussor muscle Or obstruction from the urinary bladder to urethra Or poorly functioning bladder where bladder contraction is not synchronized with opening and closing of urethral sphincter of bladder o Primary cause of UTI in children o Bottomline: There should be a one way flow traffic between urine (di pwedeng may bumabalik) o DIAGNOSTIC TEST: Radiocontrast (used VCUG ) insert cathether and fill up bladder with dye) May see a Grade 1 or grade 2 reflux- that is, reflux up to mid ureter Bladder Extrophy o Failure of fusion of abdominal wall o Defect in ventral bladder wall Followed by rupture of thin layer of ectoderm Protrusion of the bladder, exposure of mucosa o Can occur with here is not fused Group 09 o - Sometimes, associated with undescended testis o Very hard to repair. It’s a multistage repair and there are only a few pediatric surgeons in the country o Occurs in 1 in 25,000. Hypospadias o When External Urethral Meatus is in the ventral portion of the penis o In some instances, its dorsal – this is called epispedias Horseshoe-shaped Kidney Ectopic Kidney Horseshoe Shaped Kidney Polycystic Kidney Bladder Extrophy Hypospadia Page 7 of 8 Module 11: Renal Histology of the Renal System 11 February 2010 Marivic V. Bustos, MD APPENDIX Summary of activities of different parts of the tubule and Comparison of epithelial structure in different parts of the renal tubule Group 01 Page 8 of 8