Vitamin B2
Riboflavin
Structure
• Riboflavin consists of flavin (isoalloxazine ring), to
which is attached a ribitol (sugar alcohol) side
chain.
• The structures of riboflavin determined in 1933.
• Riboflavin was isolated and then later
synthesized.
• The name riboflavin signifies the presence of a
ribose likeside chain (ribo) and its yellow color
(flavus means “yellow” in Latin).
Structure
• Riboflavin consists of three rings structure
(isoalloxazine) linked to ribityl moiety. (sugar
alcohol) side chain.
• Kuhn and coworkers are determining its
structure along with Szent-Gyorgyi and
Wagner-Jaunergy in 1933.
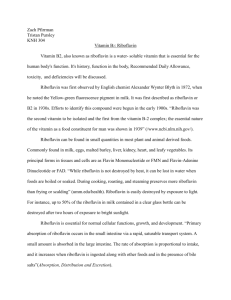
Structure of riboflavin and its coenzyme
• Riboflavin
• Flavin mononucleotide
(FMN) (coenzyme)
• Flavin adenine
dinucleotide (FAD)
(coenzyme).
Sources
• Riboflavin is found in a wide variety of foods, especially animal
origin.
• Milk and milk products such as cheeses are thought to contribute
most dietary riboflavin.
• Eggs, meat, and legumes also provide riboflavin in significant
quantities.
• Green vegetables like spinach provide fairly good riboflavin content.
• Fruits and cereal grains are minor contributors of dietary riboflavin.
• The form of riboflavin in food varies. Free or proteinbound
riboflavin is found in milk, eggs, and enriched breads and cereals.
• In most other foods the vitamin occurs as one or the other of its
coenzyme derivatives, FMN or FAD, although phosphorus-bound
riboflavin is also found in some foods.
Sources
Stability
• Stabile to heat, oxidation & acid.
• Unstable to light in both acidic and basic
medium.
• Addition of baking soda to beans destroy
much of their riboflavin content.
• Milk in proper containers is protected against
losses
• Dried sun fruits lose some of their riboflavin.
DIGESTION, ABSORPTION, TRANSPORT,
AND STORAGE
• In stomach
• Riboflavin attached to proteins may be freed by the action
of hydrochloric acid HCL secreted within the stomach and
by gastric and intestinal enzymatic hydrolysis of the protein.
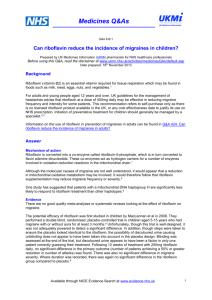
• Within intestinal lumen,
• FAD converted to FMN and FMN in turn is converted to free
riboflavin by FMN phosphatase.
FAD pyrophosphatase
FAD
FMN
FMN phosphatase
Riboflavin
ABSORPTION
• Not all bound riboflavin is hydrolyzed and absorbed.
• A small amount (~7%) of FAD is covalently bound to
either of two amino acids, histidine or cysteine.
• For example, following consumption of foods
containing succinate dehydrogenase or monoamine
oxidase, these proteins are degraded; however, the
riboflavin remains bound, typically to histidine or
cysteine residues, and cannot function in the body.
• The complex is excreted unchanged in the urine.
ABSORPTION
• Generally, animal sources of riboflavin are
thought to be better absorbed than plant
sources.
• Divalent metals such as copper, zinc, iron, and
manganese have been shown to chelate (bind
to) riboflavin and FMN and to inhibit riboflavin
absorption.
• Ingestion of alcohol also impairs riboflavin
digestion and absorption.
ABSORPTION
• In small intestine:
• Free riboflavin is absorbed by a saturable, energydependent carrier mechanism.
• It also occurs by sodium-independent carriers.
• When large amounts of the vitamin are ingested,
riboflavin may be absorbed by diffusion.
• Absorption rate is proportional to dose.
• About 95% of riboflavin intake from foods is absorbed,
up to a maximum of about 25 mg.
• Peak concentrations of the vitamin in the plasma
correlate with intakes of 15 to 20 mg.
ABSORPTION
• Within intestinal cells:
• Riboflavin is phosphorylated to form FMN, a
reaction catalyzed by flavokinase and
requiring ATP.
ABSORPTION
• At the serosal surface
• Most of the FMN is dephosphorylated by a nonspecific
alkaline phosphatase to riboflavin, which enters portal
blood for transport to the liver.
• In liver:
• The vitamin is converted to FMN and to its other
coenzyme derivative FAD.
• FAD is the predominant flavoenzyme in tissues.
TRANSPORTED
• Most flavins in systemic plasma are found as riboflavin
rather than as one of its coenzyme forms.
• All vitamin forms are transported in the plasma by
proteins, including albumin, fibrinogen, and globulins
(principally immunoglobulins).
• Albumin appears to be the primary transport protein.
• Immunoglobulins use riboflavin to activate the
antibody-catalyzed water H2O2
• Hydrogen peroxide assists in the destruction of foreign
antigens.
TRANSPORTED
• The free riboflavin is the form that traverses most
cell membranes by a carrier-mediated process.
• Riboflavin carriers in some tissues such as the
liver regulated by calcium/calmodulin.
• Diffusion, may also contribute when riboflavin
concentrations are high.
• Riboflavin is stored in the liver, kidney, and heart
in form of FAD (70-90%) or FMN) or Riboflavin. .
TRANSPORTED
• Free riboflavin is transported into and out of cells, within cells .
• Riboflavin is typically converted to its coenzyme forms by
flavokinase and FAD synthetase, both of which are widely
distributed in tissues, especially the liver, small intestine, kidneys,
and heart.
• Synthesis of FMN and FAD regulated by hormones: aldosterone,
and the thyroid hormones.
• They accelerate the conversion by increasing the activity of
flavokinase product inhibition in the case of FAD synthesis.
• After that, vitamin coenzymes become bound to apoenzymes.
• FMN and FAD function as prosthetic groups for enzymes involved in
oxidation reduction reactions called flavoproteins.
FUNCTIONS AND MECHANISMS OF ACTION
• FMN and FAD
• Are coenzymes for a wide variety of oxidative
enzyme systems and remain bound to the
enzymes during the oxidation-reduction
reactions.
• Flavins
• Act as oxidizing agents , which has an ability to
accept a pair of hydrogen atoms.
• The isoalloxazine ring is reduced and yielding
reduced forms of the flavoprotein, which can be
found in FMNH2 and FADH2.
METABOLISM AND EXCRETION
• Riboflavin and its metabolites are excreted
primarily in the urine, with only small amounts
lost in the feces.
• Fecal riboflavin metabolites may also arise from
the catabolism of riboflavin by intestinal flora.
• Most riboflavin (~60%–70%) is excreted intact in
the urine in amounts >120 μg/day.
• Urinary excretion of riboflavin may be noticeable
after two hours of ingestion of the vitamin.
RDA
• The latest (2005) recommendations for
riboflavin
• For adults 1.2 mg (for person with <2.000 kcal)
• For adult men
1.3 mg/d
• For adult women 1.1 mg/d
• For pregnancy
1.4 mg/d
• For lactation
1.6 mg/d
DEFICIENCY: ARIBOFLAVINOSIS
• Rarely occurs in isolation but most often is accompanied by
other nutrient deficits.
• Clinical symptoms of deficiency after almost 4 months of
inadequate intake include lesions on the outside of the lips
(cheilosis) and corners of the mouth (angular stomatitis),
inflammation of the tongue (glossitis), redness or bloody
(hyperemia) and swollen (edema) mouth/oral cavity, an
inflammatory skin condition seborrheic dermatitis, anemia
and eye disorders.
• Severe deficiency of riboflavin may diminish the synthesis
of the coenzyme form of vitamin B6 and the synthesis of
niacin (NAD) from tryptophan.
DEFICIENCY: ARIBOFLAVINOSIS
TOXICITY
• Toxicity associated with large oral doses of
riboflavin has not been reported, and no
tolerable upper intake level for riboflavin has
been established.
• Trials have shown use of large amounts (400
mg) of the vitamin to be effective in treating
migraine headaches without side effects.
 0
0