Paper - IAOS 2014 Conference
advertisement

Application of Life Table Method for Measuring Mortality Risk
of Non-communicable Diseases in Hong Kong
Andrew Kai-ming KWANa,∗, Lee Yuen-hoa, Dr Eddy NGa, Dr Regina CHINGa
a
Centre for Health Protection, Department of Health, Hong Kong, China
∗ Corresponding author: Tel.: +852 2961 8569; Fax: +852 2893 9425;
E-mail: stat_hs1@dh.gov.hk
Abstracts
In this paper, we apply the actuarial, or life table method to study the mortality risk between
ages 30 and 70 from four non-communicable diseases namely, cardiovascular diseases,
cancers, chronic respiratory diseases and diabetes (4 NCDs) from 1980 to 2012 in Hong
Kong based on the methodology laid down in ‘A Comprehensive Global Monitoring
Framework and Voluntary Global Targets for the Prevention and Control of NCDs’ of the
World Health Organization.
An indicator, namely ‘unconditional probability of dying between ages 30 and 70 from 4
NCDs’, is compiled by the life table method, which allows calculation of the risk of death in
the absence of other causes of death. This indicator is useful for monitoring the morality
trend in Hong Kong and comparing the mortality risk of 4 NCDs internationally across
1
countries/territories on the same basis.
In Hong Kong, the unconditional probability of death from 4 NCDs from age 30 to age 70
decreased from 0.215 in 1980 to 0.091 in 2012. The annual average rate of decline of this
probability over the period 1980-2010 is 2.7% per year. It reflects that Hong Kong is a
well-performing territory during the past three decades. The annual rate of decline was
2.9% and 5.9% in 2011 and 2012 respectively.
Keywords: age-specific mortality rate, unconditional probability of death
2
1. Introduction
1.1. World Health Organization’s global monitoring framework for non-communicable
diseases
Non-communicable diseases (NCDs) are the leading global cause of death worldwide [1].
Of the 57 million global deaths in 2008, 36 million (63%) of these were due to NCDs,
comprising mainly cardiovascular diseases, cancers, chronic respiratory diseases and
diabetes (4 NCDs). The combined burden of these diseases is rising rapidly among
lower-income countries, populations and communities. About one-fourth of global
NCD-related deaths take place before the age of 60 [2].
The 2008–2013 Action Plan was developed by the World Health Organization (WHO) and
Member States to translate the Global Strategy for the Prevention and Control of
Non-communicable Diseases [3] into concrete action. The Action Plan provides Member
States of WHO and the international community with a roadmap to establish and
strengthen initiatives for the surveillance, prevention and management of NCDs.
The importance of surveillance and monitoring of progress made in the prevention and
control of NCDs, was emphasized at the United Nations High-level Meeting of the General
Assembly on the Prevention and Control of Non-Communicable Diseases held in
September 2011 and the Political Declaration of the High-level Meeting of the General
Assembly on the Prevention and Control of Non-Communicable Diseases [4] was adopted
3
by the General Assembly. The Political Declaration urges Member States to consider the
development of national targets and indicators, based on national situations, building on
guidance provided by WHO.
Following the Political Declaration on NCDs, WHO developed a global monitoring
framework to enable global tracking of progress in preventing and controlling the 4 NCDs
and their key risk factors. The framework comprises 9 voluntary global targets and 25
indicators. Member States are encouraged to consider the development of national NCD
targets and indicators building on the global framework [5]. Among these 25 indicators,
‘unconditional probability of dying between ages 30 and 70 from 4 NCDs’ is the indicator
recommended by WHO for global monitoring of progress towards reducing premature
mortality from NCDs.
1.2. Measuring mortality risk of NCDs in Hong Kong
Of the 43 672 deaths in Hong Kong in 2012, 61% were due to the 4 NCDs. In this paper,
we apply the actuarial, or life table method to study the mortality risk between ages 30 and
70 from 4 NCDs from 1980 to 2012 in Hong Kong based on the methodology laid down in
‘A Comprehensive Global Monitoring Framework and Voluntary Global Targets for the
Prevention and Control of NCDs’ of WHO [6,7,8]. The indicator ‘unconditional probability of
dying between ages 30 and 70 from 4 NCDs’ is compiled from age-specific death rates for
the combined four causes (in terms of 5-year age groups 30-34, …, 65-69). The life table
4
method allows calculation of the risk of death between ages 30 and 70 from any of these
causes, in the absence of other causes of death. This indicator is useful for monitoring the
morality trend in Hong Kong and comparing the mortality risk of 4 NCDs internationally
across countries/territories on the same basis.
2. Methodology
2.1. WHO recommended indicator for NCD surveillance within the global monitoring
framework [6,7,8]
According to WHO’s discussion papers in 2011 and 2012, WHO recommended
‘unconditional probability of dying between ages 30 and 70 from 4 NCDs ( 40 q 30 )’ as an
indicator for global monitoring of progress toward reducing NCDs. This indicator is
calculated from age-specific death rates and the probability of dying from 4 NCDs between
ages 30 and 70 is derived by the life table method. This form of indicator was chosen to
exclude confounding across countries or over time due to differences or changes in
mortality rates for other competing causes and to control for differences in population age
structure.
The lower age limit for the indicator of 30 years represents the point in the life cycle where
the mortality risk for the four selected chronic diseases starts to rise in most populations
from very low levels at younger ages. The upper limit of 70 years was chosen for two
reasons:
5
(a) to identify an age range in which these chronic disease deaths can truly be considered
premature deaths in almost all regions of the world. It shows that estimated regional
life expectancies at age 30 for the year 2009; in all regions except the African region,
the average expected age at death for 30 year olds already exceeds 70 years; and
(b) estimation of cause-specific death rates becomes increasingly uncertain at older ages
because of increasing proportions of deaths coded to ill-defined causes, increasing
levels of co-morbidity, and increasing rates of age misstatement in mortality and
population data sources.
2.2.
WHO recommended voluntary target for NCD surveillance within the global
monitoring framework
WHO recommended the voluntary global mortality target to be set at 25% relative
reduction in overall mortality from 4 NCDs over the 15 year period 2010 - 2025.
The recommended target was based on an analysis of the historically achieved trends in
the indicator in recent decades. To set this target, WHO analysed data from 81 Member
States with at least 15 years of vital registration data between 1980-2010 that passed
quality criteria on completeness and cause-of-death assignment. WHO calculated the
average annual rate of decline in the
40 q 30
for each country from the available data within
this 30 year time period and computed the top 24th percentile for the 81 countries. On the
conservative assumption that the other Member States without such high-quality historical
6
data would all fall below this level, this percentile corresponds to the 10th percentile for all
193 Member States, and corresponds to an annual average decline of the order of 2% per
year [7,8].
The target for the 15-year period 2010-2025 was thus set at a 25% relative reduction (2%
annual reduction compounded for 15 years). The historic experience of best performing
countries over the period 1980-2010 has shown that very substantial declines in NCD
death rates can be achieved, and that the proposed target is achievable.
2.3.
Calculation of
40 q 30
2.3.1. Notations
The following notations are used for abridged life table:
x
exact age in years.
n
length of interval in years. This symbol is omitted when n 1 .
n Dx
number of deaths occurring to persons aged x to x n of the period under
consideration.
n Px
number of persons aged x to x n alive at the mid-point of the period under
consideration.
nMx
age-specific death rates calculated from information on deaths among persons
aged x to x n during a given year and the population aged x to x n at
the mid-point of the same year.
7
n qx
Probability of dying between exact ages x and x n .
2.3.2. Age-specific mortality rate from 4 NCDs
First, we calculate age-specific mortality rate from 4 NCDs for each five-year age group, for
each 5-year age range between 30 and 70:
5Mx
5 Dx
from 4 NCDs
5 Px
2.3.3. Probability of death in each 5-year age range
We then translate the 5-year death rate to the probability of death in each 5-year age range
by the actuarial method [9]:
5 qx
5 5M x
1 2.5 5 M x
The above formula is derived on the assumption that deaths are linearly distributed
throughout the year. For the derivation of this formula, see Appendix.
2.3.4. Unconditional probability of death from age 30 to age 70
We then calculate
40 q 30 :
40 q30
1 1 5 q30 1 5 q35 1 5 q65
2.3.5. Average annual rate of decline
At this point, we have
40 q 30
for each year from 1980 to 2010. We next calculate the
average annual rate of decline by regressing log probability of death on year using ordinary
least squares regression:
ln 40 q30 year
This generates a coefficient ( ) for each country/territory, from which we calculate the
8
equivalent 30-year relative decline as follows:
Annual average change in
We can use this annual average change in
40 q30
40q30
1 e
for international comparison of mortality
risk of 4 NCDs across countries/territories on the same basis.
2. The Data
Data of registered death records in Hong Kong for each year from 1980 to 2012 is used in
this study. A database of registered death records is maintained by the Department of
Health.
Registration of death is a legal requirement in Hong Kong and all deaths must be
registered at the Deaths Registries of the Immigration Department. For deaths that are not
classified as ‘reportable deaths’ under the Coroners Ordinance, doctors are required by
law to provide information related to cause of death for deceased persons who were under
their care by completing the Medical Certificate of the Cause of Death.
The International Classification of Diseases (ICD), developed by WHO, has been adopted
for disease coding in Hong Kong and the reason of adopting lCD is to provide good quality
of mortality and morbidity statistics for formulating health policy.
In this study, the classification of diseases and causes of death is based on the Ninth
Revision of the ICD (ICD-9) for each year from 1980 to 2000, while the classification of
diseases and causes of death is based on the Tenth Revision of the ICD (ICD-10) for each
9
year from 2001 to 2012. Table 1 exhibits the coverage of the four selected NCDs.
Table 1
Coverage of four selected NCDs
Four selected NCDs
ICD-9 codes and descriptions
ICD-10 codes and descriptions
(data: 1980-2000)
(data: 2001-2012)
Diseases of the circulatory system
Diseases of the circulatory system
(390-459)
(I00-I99)
Cancer
Malignant neoplasms (140-208)
Malignant neoplasms (C00-C97)
Chronic respiratory
Other diseases of upper respiratory
Other diseases of upper respiratory
disease
tract, chronic obstructive pulmonary
tract, chronic lower respiratory
disease and allied conditions,
diseases, lung diseases due to
pneumoconioses and other lung
external agents, other respiratory
diseases due to external agents and
diseases principally affecting the
other diseases of the respiratory
interstitium, suppurative and necrotic
system (470-478, 490-519)
conditions of lower respiratory tract,
Cardiovascular disease
other diseases of pleura and other
diseases of the respiratory system
(J30-J98)
Diabetes
Diabetes mellitus (250)
Diabetes mellitus (E10-E14)
Figures for 1980-2000 based on ICD-9 are comparable with those figures for 2001-2012 based on
ICD-10.
3. Results
3.1
Age-specific mortality rate from the combined four NCD causes of Hong Kong
Figure 1 exhibits the age-specific mortality rates from the combined four causes for each
5-year age group (30-34, 35-39, …, 65-69) over the period 1980-2012.
10
0.02
Age-specific mortality rate
0.015
₅M₃₀
₅M₃₅
0.01
₅M₄₀
₅M₄₅
₅M₅₀
₅M₅₅
₅M₆₀
0.005
₅M₆₅
0
1980
1985
1990
2000
1995
2005
2010
Year
Fig. 1. Age-specific mortality rate for each 5-year age group, 1980-2012
Figure 1 shows that the age-specific mortality rates from the combined four causes for all
5-year age groups declined over the past three decades.
3.2
Probability of death from the combined four NCD causes of Hong Kong
Figure 2 exhibits the probability of dying from the combined four causes for each 5-year
age group (30-34, 35-39, …, 65-69) over the period 1980-2012.
11
0.1
0.09
Probabbility of dying between exact age x and x+5
0.08
0.07
0.06
₅q₃₀
₅q₃₅
0.05
₅q₄₀
₅q₄₅
0.04
₅q₅₀
₅q₅₅
0.03
₅q₆₀
₅q₆₅
0.02
0.01
0
1980
1985
1990
1995
2000
2005
2010
Year
Fig. 2. Probability of dying between exact age x and x+5, 1980-2012
Figure 2 shows that the probability of dying from the combined four causes for all 5-year
age groups declined over the past three decades.
3.3
40 q 30
of Hong Kong
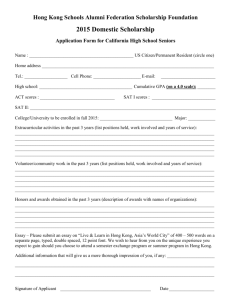
Figure 3 exhibits
40 q 30
of Hong Kong over the period 1980-2012.
12
0.25
Probability of dying
0.2
0.15
0.1
0.05
0
1980
1985
1990
1995
2000
2005
2010
Year
Fig. 3. Probability of dying from age 30 to age 70 (₄₀q₃₀), 1980-2012
Figure 3 shows that
3.4
40 q 30
decreased from 0.215 in 1980 to 0.091 in 2012.
Average annual rate of decline of
40 q 30
We next calculate the average annual rate of decline of
40 q 30
over the period 1980-2010
by regressing ln 40 q 30 on year using ordinary least squares regression:
ln 40 q30 year
This generates a coefficient ( ), from which we calculate the equivalent 30-year relative
decline as follows:
Annul average change in
40q30
1 e
Figure 4 exhibits the regression results of ln 40 q 30 on year by fitting ordinary least
squares regression over the period 1980-2010.
13
Year
-1.5
1980
1985
1990
1995
2000
2005
2010
Log probability of dying
-1.75
-2
-2.25
ln(₄₀q₃₀)
Ordinary least squares regression line
-2.5
Fig. 4. Log probability of dying from age 30 to age 70 (ln(₄₀q₃₀)), 1980-2012
The fitted regression line over the period 1980-2010:
ln 40 q30 53.1686 0.0276 year
F Ratio 2037 .8 with p 0.001 , and R 2 98.6%
Regression results show that the annual average rate of decline of
40 q 30
of Hong Kong
over the period 1980-2010 is 2.7% per year, which is comparable to the declining rate of
the order of 2% per year of the 10th percentile of all Member States of WHO over the same
period [7,8]. It reflects that Hong Kong is a well-performing territory during the past three
decades. The annual rate of decline persisted in 2011 and 2012 at 2.9% and 5.9%
respectively.
4. Discussion
The mortality risk of the four major NCDs is highly associated with a wide spectrum of
14
lifestyle or behavioral risk factors. For example,
(a) WHO estimated that eight risk factors – alcohol use, tobacco use, high blood pressure,
high body mass index, high cholesterol, high blood glucose, low fruit and vegetable
intake, and physical inactivity – account for 61% of cardiovascular deaths. Reducing
exposure to these eight risk factors would increase global life expectancy by almost 5
years [10]. Additional mortality reductions are feasible through targeted health service
interventions for people with high cardiovascular risk and for patients who have
experienced an acute cardiovascular disease event [7].
(b) WHO estimated that the five leading behavioral and dietary risks – high body mass
index, low fruit and vegetable intake, physical inactivity, tobacco use and alcohol use –
are responsible for 30% of cancer deaths. Cancers with the largest proportions
attributable to preventable risk factors are cervical cancer (100%) and lung cancer
(71%). Seventy percent of liver cancers and 60% of stomach cancers are due to
infectious agents [11].
(c) Around 60% of chronic respiratory disease deaths are attributable to tobacco smoking
or exposure to indoor smoke from solid fuels [7,10].
(d) Around 60% of the risk of Type 2 diabetes mellitus can be prevented through life style
modifications [13] and additional mortality reductions can be achieved through
diagnosis and treatment [7].
15
Strong NCD surveillance system, along with proper public health policies such as health
promotion, risk communication, disease prevention and treatment interventions, can result
in large reduction in death rates for 4 NCDs in Hong Kong.
5. Conclusions
In this paper, we apply the actuarial, or life table method to study the mortality risk between
ages 30 and 70 from 4 NCDs from 1980 to 2012 in Hong Kong based on the methodology
laid down in ‘A Comprehensive Global Monitoring Framework and Voluntary Global Targets
for the Prevention and Control of NCDs’ of WHO.
An indicator ‘unconditional probability of dying between ages 30 and 70 from 4 NCDs’ is
compiled from age-specific death rates of the combined four cause categories. The life
table method is employed to calculate the unconditional probability of dying. The method
allows calculation of the risk of death between ages 30 and 70 from any of these causes, in
the absence of other causes of death.
In Hong Kong, the age-specific mortality rates from the combined four causes for all 5-year
age groups declined over the past three decades. The unconditional probability of death
from 4 NCDs from age 30 to age 70 decreased from 0.215 in 1980 to 0.091 in 2012. The
annual average rate of decline of this probability over the period 1980-2010 is 2.7% per
year, which is comparable to the declining rate of the order of 2% per year of the 10th
percentile of all Member States of WHO over the same period. It reflects that Hong Kong is
16
a well-performing territory during the past three decades. The annual rate of decline was
2.9% and 5.9% in 2011 and 2012 respectively.
This indicator is useful for monitoring the morality trend in Hong Kong and for comparing
the mortality risk of 4 NCDs internationally across countries/territories on the same basis.
Acknowledgements
The authors wish to express their sincere thanks to Louis FAN, Iris CHOW, and Carol
TSANG for their valuable support in preparing the mortality dataset and statistical
computing for this study.
References
[1]
A. Alwan, D.R. MacLean, L.M. Riley, E.T. d’Espaignet, C.D. Mathers, G.A. Stevens
and D. Bettcher, Monitoring and surveillance of chronic non-communicable diseases:
progress and capacity in high-burden countries. The Lancet 376 (2010), 1861-1868.
[2]
Global status report on noncommunicable diseases 2010. Geneva, World Health
Organization, 2011.
[3]
2008 - 2013 Action plan for the global strategy for the prevention and control of
noncommunicable diseases. Geneva, World Health Organization, 2008.
[4]
Political declaration of the high-level meeting of the general assembly on the
prevention and control of non-communicable diseases. New York, United States of
America, United Nations, 2011.
17
[5]
Resolutions and decisions of the sixth-fifth world health assembly. Geneva, World
Health Organization, 21-26 May 2012.
[6]
WHO discussion paper, A comprehensive global monitoring framework and voluntary
global targets for the prevention and control of NCDs. World Health Organization,
2011.
[7]
Second WHO discussion paper, A comprehensive global monitoring framework
including indicators and a set of voluntary global targets for the prevention and
control of noncommunicable diseases World Health Organization, 2012.
[8]
Revised WHO discussion paper, A comprehensive global monitoring framework
including indicators, and a set of voluntary global targets for the prevention and
control of noncommunicable diseases, World Health Organization, 2012.
[9]
L.J. Reed and M. Merrell, A short method for constructing an abridged life table. The
American Journal of Hygiene 30 (1939), 993-1022.
[10] Global health risks: mortality and burden of disease attributable to selected major
risks. Geneva, World Health Organization, 2009.
[11] J.J. Ott, A. Ullrich, M. Mascarenhas and G.A. Stevens, Global cancer incidence and
mortality caused by behavior and infection. Journal of Public Health 32(2011),
223-33.
[12] J. Tuomilehto, J. Lindström, J.G Eriksson , T.T. Valle, H. Hämäläinen,
18
P. Ilanne-Parikka, S. Keinänen-Kiukaanniemi, M Laakso, A. Louheranta, M. Rastas ,
V. Salminen and M. Uusitupa M, Prevention of type 2 diabetes mellitus by changes in
lifestyle among subjects with impaired glucose tolerance. The New England Journal
of Medicine (2001), 1343-50.
19
Appendix
Derivation of the Formula Relating Observed Death Rate and Probability of Death
Notation and derivations
(a) Notation:
x exact age in years.
n length of interval in years. This symbol is omitted when n 1.
For the observed vital statistics:
deaths in the age group x to x n .
n Dx
n Px
population in the age group x to x n .
nMx
n Dx
n Px
death rate in the age group x to x n .
For the life table population:
l x survivors to age x out of a given initial number. If the initial number is unity, l x
is the probability of surviving from the initial age to age x
(b) Derivation of the formula
n
qx
n nM x
:
n
1 nM x
2
Assume that over the interval n,
l s a bs
20
By definition
Mx
n
l x l xn
xn
x
n
{
qx
(1)
ls ds
l x l xn
lx
(2)
Then, equations (1) and (2) becomes
nMx
{
n
qx
a bx a b( x n )
xn
x ( a
bs)ds
b
bn
a bx
2
a bx a b( x n)
bn
a bx
a bx
(3)
(4)
Eliminating a bx between equations (3) and (4) gives
n
qx
n nM x
n
1 nM x
2
For n 5 ,
5 qx
5 5M x
1 2.5 5 M x
21