2013-gemc-res-lex-bursitis__tendonitis-oer
advertisement

Project: Ghana Emergency Medicine Collaborative
Document Title: Bursitis, Tendonitis, Fibromyalgia, and RSD
Author(s): Joe Lex, MD, 2013 (Temple University School of Medicine)
License: Unless otherwise noted, this material is made available under the
terms of the Creative Commons Attribution Share Alike-3.0 License:
http://creativecommons.org/licenses/by-sa/3.0/
We have reviewed this material in accordance with U.S. Copyright Law and have tried to maximize your
ability to use, share, and adapt it. These lectures have been modified in the process of making a publicly
shareable version. The citation key on the following slide provides information about how you may share and
adapt this material.
Copyright holders of content included in this material should contact open.michigan@umich.edu with any
questions, corrections, or clarification regarding the use of content.
For more information about how to cite these materials visit http://open.umich.edu/privacy-and-terms-use.
Any medical information in this material is intended to inform and educate and is not a tool for self-diagnosis
or a replacement for medical evaluation, advice, diagnosis or treatment by a healthcare professional. Please
speak to your physician if you have questions about your medical condition.
Viewer discretion is advised: Some medical content is graphic and may not be suitable for all viewers.
1
Attribution Key
for more information see: http://open.umich.edu/wiki/AttributionPolicy
Use + Share + Adapt
{ Content the copyright holder, author, or law permits you to use, share and adapt. }
Public Domain – Government: Works that are produced by the U.S. Government. (17 USC § 105)
Public Domain – Expired: Works that are no longer protected due to an expired copyright term.
Public Domain – Self Dedicated: Works that a copyright holder has dedicated to the public domain.
Creative Commons – Zero Waiver
Creative Commons – Attribution License
Creative Commons – Attribution Share Alike License
Creative Commons – Attribution Noncommercial License
Creative Commons – Attribution Noncommercial Share Alike License
GNU – Free Documentation License
Make Your Own Assessment
{ Content Open.Michigan believes can be used, shared, and adapted because it is ineligible for copyright. }
Public Domain – Ineligible: Works that are ineligible for copyright protection in the U.S. (17 USC § 102(b)) *laws in
your jurisdiction may differ
{ Content Open.Michigan has used under a Fair Use determination. }
Fair Use: Use of works that is determined to be Fair consistent with the U.S. Copyright Act. (17 USC § 107) *laws in your
jurisdiction may differ
Our determination DOES NOT mean that all uses of this 3rd-party content are Fair Uses and we DO NOT guarantee that
your use of the content is Fair.
2
To use this content you should do your own independent analysis to determine whether or not your use will be Fair.
Bursitis, Tendonitis,
Fibromyalgia, and RSD
Joe Lex, MD, FAAEM
Temple University School of Medicine
Philadelphia, PA
3
Emergency Medicine
Objectives
1. Explain how bursitis and
tendonitis are similar
2. Explain how bursitis and
tendonitis differ from from another
3. List phases in development and
healing of bursitis and tendonitis
4
Emergency Medicine
Objectives
4. List common types of bursitis and
tendonitis found at the:
Shoulder
Hip
Elbow
Knee
Wrist
Ankle
5. List indications / contraindications
for injection therapy of bursitis
and tendonitis
5
Emergency Medicine
Objectives
6. Describe typical findings in a
patient with fibromyalgia
7. Describe typical findings in a
patient with reflex sympathetic
dystrophy
6
Emergency Medicine
Sports
Society more athletic
Physical activity health benefits
Overuse syndromes increase
25% to 50% of participants will
experience tendonitis or bursitis
7
Emergency Medicine
Workplace
Musculoskeletal disorders from…
…repetitive motions
…localized contact stress
…awkward positions
…vibrations
…forceful exertions
Ergonomic design incidence
8
Emergency Medicine
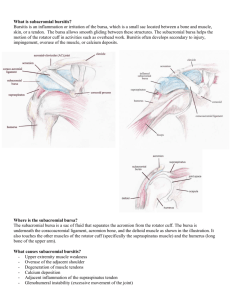
Bursae
Closed, round, flat sacs
Lined by synovium
May or may not communicate with
synovial cavity
Occur at areas of friction between
skin and underlying ligaments /
bone
9
Emergency Medicine
Bursae
Permit lubricated movement over
areas of potential impingement
Many are nameless
~78 on each side of body
New bursae may form anywhere
from frequent irritation
10
Emergency Medicine
Bursitis
Inflamed by…
…chronic friction
…trauma
…crystal
deposition
…infection
…systemic
disease:
rheumatoid
arthritis,
psoriatic
arthritis, gout
ankylosing
spondylitis
11
Emergency Medicine
Bursitis
Inflammation causes
bursal synovial cells to
thicken
Excess fluid
accumulates inside and
around affected bursae
Bemoeial (Wikipedia)
12
Emergency Medicine
Tendons
Tendon sheaths composed of
same synovial cells as bursae
Inflamed in similar manner
Tendonitis: inflammation of tendon
only
Tenosynovitis: inflammation of
tendon plus its sheath
13
Emergency Medicine
Tendons
Inflammatory changes involving
sheath well documented
Inflammatory lesions of tendon
alone not well documented
Distinction uncertain: terms
tendonitis and tenosynovitis used
interchangeably
14
Emergency Medicine
Tendons
Most overuse syndromes are NOT
inflammatory
Biopsy: no inflammatory cells
High glutamate concentrations
NSAIDs / steroids: no advantage
TendonITIS a misnomer
15
Emergency Medicine
Gray's Anatomy (Wikipedia)
16
Bursitis / Tendonitis
Most common causes:
mechanical overload and
repetitive microtrauma
Most injuries
multifactorial
17
Emergency Medicine
Bursitis / Tendonitis
Intrinsic factors: malalignment,
poor muscle flexibility, muscle
weakness or imbalance
Extrinsic factors: design of
equipment or workplace and
excessive duration, frequency, or
intensity of activity
18
Emergency Medicine
Immediate Phase
Release of chemotactic and
vasoactive chemical mediators
Vasodilation and cellular edema
PMNs perpetuate process
Lasts 48 hours to 2 weeks
Repetitive insults prolong
inflammatory stage
19
Emergency Medicine
Healing Phase
Classic inflammatory signs: pain,
warmth, erythema, swelling
Healing goes through proliferative
and maturation
6 to 12 weeks: organization and
collagen cross-linking mature to
preinjury strength
20
Emergency Medicine
History
Changes in sports activity, work
activities, or workplace
Cause not always found
Pregnancy, quinolone therapy,
connective tissue disorders,
systemic illness
21
Emergency Medicine
History
Most common complaint: PAIN
Acute or chronic
Frequently more severe after
periods of rest
May resolve quickly after initial
movement only to become
throbbing pain after exercise
22
Emergency Medicine
Articular vs. Periarticular
In joint capsule
Joint pain / warmth /
swelling
Worse with active &
passive movement
All parts of joint
involved
Periarticular
Pain not uniform
across joint
Pain only certain
movements
Pain character &
radiation vary
23
Emergency Medicine
Physical Exam
Careful palpation
Range of motion
Heat, warmth, redness
24
Emergency Medicine
Lab Studies
Screening tests: CBC, CRP, ESR
Chronic rheumatic disease: mild
anemia
Rheumatoid factor, antinuclear
antibody, antistreptolysin O titers,
and Lyme serologies for follow-up
Serum uric acid: not helpful
25
Emergency Medicine
Synovial Fluid
Especially crystalline, suppurative
etiology
Appearance, cell count and diff,
crystal analysis, Gram’s stain
– Positive Gram’s: diagnostic
– Negative Gram’s: cannot rule out
26
Emergency Medicine
Management
Rest
Pain relief: meds, heat, cold
No advantage to NSAIDs
Exceptions: olecranon bursitis and
prepatellar bursitis have a
moderate risk of being infected
(Staphylococcus aureus)
27
Emergency Medicine
Management
Shoulder: immobilize few days
– Risk of adhesive capsulitis
Lateral epicondylitis: forearm
brace
Olecranon bursitis: compression
dressing
28
Emergency Medicine
Management
De Quervain’s: splint wrist and
thumb in 20o dorsiflexion
Achilles tendonitis: heel lift or splint
in slight plantar flexion
29
Emergency Medicine
Local
Injection
30
Emergency Medicine
Local Injection
Lidocaine or steroid injection can
overcome refractory pain
Steroids universally given, often
with great success
No good prospective data to
support or refute therapeutic
benefit
31
Emergency Medicine
Local Injection
Short course of oral steroid may
produce statistically similar results
Primary goal of steroid injection:
relieve pain so patient can
participate in physical rehab
32
Emergency Medicine
Local Injection
Adjunct to other modalities: pain
control, PT, exercise, OT, relative
rest, immobilization
Additional pain control: NSAIDs,
acupuncture, ultrasound, ice, heat,
electrical nerve stimulation
33
Emergency Medicine
Local Injection
Analgesics + exercise: better
results than exercise alone
Eliminate provoking factors
Avoid repeat steroid injection
unless good prior response
Wait at least 6 weeks between
injections in same site
34
Emergency Medicine
Indications
Diagnosis
Obtain fluid for analysis
Eliminate referred pain
Therapy
Give pain relief
Deliver therapeutic agents
35
Emergency Medicine
Contraindication: Absolute
Bacteremia
Infectious arthritis
Periarticular cellulitis
Adjacent osteomyelitis
Significant bleeding disorder
Hypersensitivity to steroid
Osteochondral fracture
36
Emergency Medicine
Contraindication: Relative
Violation of skin integrity
Chronic local infection
Anticoagulant use
Poorly controlled diabetes
Internal joint derangement
Hemarthrosis
Preexisting tendon injury
Partial tendon rupture
37
Emergency Medicine
Preparations
Local anesthetic
Hydrocortisone / corticosteroid
Rapid anti-inflammatory effect
Categorized by solubility and
relative potency
High solubility short duration
– Absorbed, dispersed more rapidly
38
Emergency Medicine
Preparations
Triamcinolone hexacetonide: least
soluble, longest duration
– Potential for subcutaneous atrophy
– Intra-articular injections only
Methylprednisolone acetate
(Depo-Medrol®): reasonable first
choice for most ED indications
39
Emergency Medicine
Dosage
Large bursa: subacromial,
olecranon, trochanteric: 40 – 60
mg methylprednisolone
Medium or wrist, knee, heel
ganglion: 10 – 20 mg
Tendon sheath: de Quervain,
flexor tenosynovitis: 5 – 15 mg
40
Emergency Medicine
Site Preparation
Use careful aseptic technique
Mark landmarks with skin pencil,
tincture of iodine, or thimerosal
(Merthiolate®) (sterile Q-tip)
Clean point of entry: povidoneiodine (Betadine®) and alcohol
Do not need sterile drapes
41
Emergency Medicine
Technique
Make skin wheal: 1% lidocaine or
0.25% bupivacaine OR…
…use topical vapocoolant: e.g.,
Fluori-Methane®
Use Z-tract technique: limits risk of
soft tissue fistula
Agitate syringe prior to injection:
steroid can precipitate or layer
42
Emergency Medicine
Complications: Acute
Reaction to anesthetic: rare
– Treat as in standard textbooks
Accidental IV injection
Vagal reaction: have patient flat
Nerve injury: pain, paresthesias
Post injection flare: starts in hours,
gone in days (~2%)
43
Emergency Medicine
Complications: Delayed
Localized subcutaneous or
cutaneous atrophy at injection site
Small depression in skin with
depigmentation, transparency, and
occasional telangiectasia
– Evident in 6 weeks to 3 months
– Usually resolve within 6 months
– Can be permanent
44
Emergency Medicine
Complications: Delayed
Tendon rupture: low risk (<1%)
Dose-related
Related to direct tendon injection?
Limit injections to no more than
once every 3 to 4 months
Avoid major stress-bearing
tendons: Achilles, patellar
45
Emergency Medicine
Complications: Delayed
Systemic absorption slower than
with oral steroids
Can suppress hypopituitaryadrenal axis for 2 to 7 days
Can exacerbate hyperglycemia in
diabetes
Abnormal uterine bleeding
reported
46
Emergency Medicine
Some
specific
entities…
47
Emergency Medicine
Shoulder Region
Gray's Anatomy (Wikipedia)
48
Emergency Medicine
Shoulder Region
“Bursitis of the shoulder”
•Supraspinatus tendon and subdeltoid bursa
“Bicipital tendonitis”
•Tendon of long head of biceps
49
Emergency Medicine
Bicipital Tendonitis
Risk: repeatedly flex elbow against
resistance: weightlifter, swimmer
Tendon goes through bicipital
(intertubercular) groove
Pain with elbow at 90° flexion,
arm internally / externally rotated
50
Emergency Medicine
Bicipital Tendonitis
Range of motion: normal or
restricted
Strength: normal
Tenderness: bicipital groove
Pain: elevate shoulder, reach hip
pocket, pull a back zipper
51
Emergency Medicine
Bicipital Tendonitis
Lipman test: "rolling" bicipital
tendon produces localized
tenderness
Yergason test: pain along bicipital
groove when patient attempts
supination of forearm against
resistance, holding elbow flexed at
90° against side of body
52
Emergency Medicine
Calcific Tendonitis
Supraspinatus Tendonitis
Subacromial Bursitis
Calcific (calcareous) tendonitis:
hydroxyapatite deposits in one or
more rotator cuff tendons
– Commonly supraspinatus
Sometimes rupture into adjacent
subacromial bursa
Acute deltoid pain, tenderness
53
Emergency Medicine
Calcific Tendonitis
54
Calcific Tendonitis
Supraspinatus Tendonitis
Subacromial Bursitis
Clinically similar: difficult to
differentiate
Rotator cuff: teres minor,
supraspinatus, infraspinatus,
subscapularis
– Insert as conjoined tendon into
greater tuberosity of humerus
55
Emergency Medicine
Calcific Tendonitis
Supraspinatus Tendonitis
Subacromial Bursitis
Jobe’s sign, AKA “empty can test”
Abduct arm to 90o in the scapular
plane, then internally rotate arms
to thumbs pointed downward
Place downward force on arms:
weakness or pain if supraspinatus
56
Emergency Medicine
Calcific Tendonitis
Supraspinatus Tendonitis
Subacromial Bursitis
Other tests: Neer, Hawkins
Passively abduct arm to 90°, then
passively lower arm to 0° and ask
patient to actively abduct arm to
30°
57
Emergency Medicine
Calcific Tendonitis
Supraspinatus Tendonitis
Subacromial Bursitis
If can abduct to 30° but no
further, suspect deltoid
If cannot get to 30°, but if placed
at 30° can actively abduct arm
further, suspect supraspinatus
If uses hip to propel arm from 0°
to beyond 30°, suspect
supraspinatus
58
Emergency Medicine
Calcific Tendonitis
Supraspinatus Tendonitis
Subacromial Bursitis
Subacromial bursa: superior and
lateral to supraspinatus tendon
Tendon and bursa in space
between acromion process and
head of humerus
Prone to impingement
59
Emergency Medicine
Calcific Tendonitis / Supraspinatus
Tendonitis / Subacromial Bursitis
Patient holds arm protectively
against chest wall
May be incapacitating
All ROM disturbed, but internal
rotation markedly limited
Diffuse perihumeral tenderness
X-ray: hazy shadow
60
Emergency Medicine
Calcific Tendonitis / Supraspinatus
Tendonitis / Subacromial Bursitis
61
Drongo (Wikipedia)
Emergency Medicine
Rotator Cuff Tear
62
Nucleus Communications (Wikimedia Commons)
Emergency Medicine
Rotator Cuff Tear
Drop arm test: arm passively
abducted at 90o, patient asked to
maintain dropped arm
represents large rotator cuff tear
Shrug sign: attempt to abduct arm
results in shrug only
63
Emergency Medicine
Elbow and Wrist
• “Student’s elbow”
Olecranon bursa
• “Tennis Elbow”
Extendor tendons posteriorly at ischial tuberosity
• De Quervain’s tenosynovitis
Tendons of extensor pollicis brevis and abductor pollicis longus
• “Acute tendonitis of the wrist”
Flexor carpi ulnaris and other wrist flexor tendons
64
Emergency Medicine
Elbow and Wrist
Pngbot (Wikipedia)
65
Emergency Medicine
Lateral Epicondylitis
Pain at insertion of extensor carpi
radialis and extensor digitorum
muscles
Radiohumeral bursitis: tender over
radiohumeral groove
Tennis elbow: tender over lateral
epicondyle
66
Emergency Medicine
Lateral Epicondylitis
67
Gray's Anatomy (Wikipedia)
Emergency Medicine
Lateral Epicondylitis
History repetitive overhead motion:
golfing, gardening, using tools
Worse when middle finger
extended against resistance with
wrist and the elbow in extension
Worse when wrist extended
against resistance
68
Emergency Medicine
Radial Tunnel Syndrome
69
Gray's Anatomy (Wikipedia)
Emergency Medicine
Medial Epicondylitis
“Golfer's elbow” or “pitcher’s
elbow” similar
Much less common
Worse when wrist flexed against
resistance
Tender medial epicondyle
70
Emergency Medicine
Cubital Tunnel Syndrome
Ulnar nerve passes through cubital
tunnel just behind ulnar elbow
Numbness and pain small and ring
fingers
Initial treatment: rest, splint
71
Emergency Medicine
Cubital Tunnel Syndrome
Area of Pain
Schplook (Open Clipart)
Area of Numbness
Schplook (Open Clipart)
Emergency Medicine
72
Olecranon Bursitis
“Student's” or “barfly elbow”
Most frequent site of septic bursitis
Aseptic: motion at elbow joint
complete and painless
Septic: all motion usually painful
73
Emergency Medicine
Olecranon Bursitis
Aseptic olecranon bursitis
Cosmetically bothersome, usually
resolves spontaneously
If bothersome, aspiration and
steroid injection speed resolution
Oral NSAID after steroid injection
does not affect outcome
74
Emergency Medicine
Olecranon Bursitis
Source Undetermined
75
Emergency Medicine
Septic Olecranon Bursitis
Most common septic bursitis:
olecranon and prepatellar
2o to acute trauma / skin breakage
Impossible to differentiate acute
gouty olecranon bursitis from
septic bursitis without laboratory
analysis
76
Emergency Medicine
77
Arcadian (Wikimedia Commons)
Ganglion Cysts
Swelling on dorsal wrist
~60% of wrist and hand soft tissue
tumors
Etiology obscure
Lined with mesothelium or
synovium
Arise from tendon sheaths or near
joint capsule
78
Emergency Medicine
Ganglion Cysts
79
Source Undetermined
Emergency Medicine
Ganglion Cysts
Cieslaw (Wikipedia)
80
Emergency Medicine
Source Undetermined
Source Undetermined
81
Source Undetermined
Carpal Tunnel Syndrome
Median nerve compression in
fibro-osseous tunnel of wrist
Pain at wrist that sometimes
radiates upward into forearm
Associated with tingling and
paresthesias of palmar side of
index and middle fingers and radial
half of the ring finger
82
Emergency Medicine
Carpal Tunnel Syndrome
83
BruceBlaus (Wikipedia)
Emergency Medicine
Carpal Tunnel Syndrome
Numbness
Schplook (Open Clipart)
Pain
Schplook (Open Clipart)
Emergency Medicine
84
Carpal Tunnel Syndrome
Patient wakes during night with
burning or aching pain, numbness,
and tingling
Positive Tinel sign: reproduce
tingling and paresthesias by
tapping over median nerve at volar
crease of wrist
85
Emergency Medicine
Carpal Tunnel Syndrome
www.hulc.co.uk (Wikimedia Commons)
86
Emergency Medicine
Carpal Tunnel Syndrome
Positive Phalen test: flexed wrists
held against each other for several
minutes in effort to provoke
symptoms in median nerve
distribution
87
Emergency Medicine
Carpal Tunnel Syndrome
Source Undetermined
88
Emergency Medicine
Carpal Tunnel Syndrome
May be idiopathic
Known causes: rheumatoid
arthritis pregnancy, diabetes,
hypothyroidism, acromegaly
89
Emergency Medicine
Carpal Tunnel Syndrome
Insert needle just radial or ulnar to
palmaris longus and proximal to
distal wrist crease
Ulnar preferred: avoids nerve
Direct needle at 60° to skin
surface, point toward tip of middle
finger
90
Emergency Medicine
de Quervain’s Disease
Chronic tenosynovitis due to
narrowed tendon
sheaths around
abductor policis
longus and
extensor pollicis
brevis muscles
Gray’s Anatomy (Wikipedia)
91
Emergency Medicine
de Quervain’s Disease
1st dorsal compartment
Radial border of anatomic snuffbox
1st compartment may cross over
2nd compartment (ECRL/B)
proximal to extensor retinaculum
Steroid injections relieve most
symptoms
92
Emergency Medicine
de Quervain’s Disease
Source Undetermined
Finkelstein’s Test
93
Emergency Medicine
Trigger Finger
Digital flexor tenosynovitis
Stenosed tendon sheath
– Palmar surface over MC head
Intermittent tendon “catch”
“Locks” on awakening
Most frequent: ring and middle
94
Emergency Medicine
Trigger Finger
www.med.und.edu
95
Emergency Medicine
Trigger Finger
Tendon sheath walls lined with
synovial cells
Tendon unable to glide within
sheath
Initial treatment: splint, moist heat,
NSAID
Steroid for recalcitrant cases
96
Emergency Medicine
Hip and Groin
• “ischial bursitis”
Located medial to the sciatic nerve
• “trochanteric bursitis”
Gluteus medius and minimus tendons
• “iliopectineal bursitis”
Located lateral to femoral vessels
97
Emergency Medicine
Hip and Groin
98
Beth Ohara (Wikipedia)
Emergency Medicine
Anterior View
Hip and Groin
Posterior View
99
Gray's Anatomy (Wikipedia)
Gray's Anatomy (Wikipedia)
Emergency Medicine
Trochanteric Bursitis
Second leading cause of lateral
hip pain after osteoarthritis
Discrete tenderness to deep
palpation
Principal bursa between gluteus
maximus and posterolateral
prominence of greater trochanter
100
Emergency Medicine
Trochanteric Bursitis
Pain usually chronic
Pathology in hip abductors
May radiate down thigh, lateral or
posterior
Worse with lying on side, stepping
from curb, descending steps
101
Emergency Medicine
Trochanteric Bursitis
Patrick fabere sign (flexion,
abduction, external rotation, and
extension) may be negative
Passive ROM relatively painless
Active abduction when lying on
opposite side pain
Sharp external rotation pain
102
Emergency Medicine
Ischiogluteal Bursitis
Weaver's bottom / tailor’s seat:
pain center of buttock radiating
down back of leg
Often mistaken for back strain,
herniated disk
Pain worse with sitting on hard
surface, bending forward, standing
on tiptoe
103
Emergency Medicine
Ischiogluteal Bursitis
Tenderness over ischial tuberosity
Ischiogluteal bursa adjacent to
ischial tuberosity, overlies sciatic /
posterior femoral cutaneous
nerves
104
Emergency Medicine
Some Other Back Pains
Low back pain: Spasm and
tenderness of lumbosacral
musculature and straightening
of normal lumbar lordosis
Trochanteric bursitis: localized pain
over greater trochanter
Coccygodynia: Pain localized
to the coccyx
Sciatica: localized tenderness
at the sciatic notch
Ischial bursitis: localized tenderness
105
medial to the sciatic nerve
Gray's Anatomy (Wikipedia)
Emergency Medicine 120
Legs and Feet
“Housemaid’s knee”
prepatellar bursa
“Infrapatellar bursitis”
infrapatellar bursa
“Anserine bursitis”
anserine bursa
“Bursitis of the heel”
Achilles tendon
Gray's Anatomy (Wikipedia)
106
Gray's Anatomy (Wikipedia)
Emergency Medicine
Knee
BruceBlaus (Wikipedia)
107
Emergency Medicine
Prepatellar Bursitis
Housemaid’s knee / nun’s knee:
swelling with effusion of superficial
bursa over lower pole of patella
Passive motion fully preserved
Pain mild except during extreme
knee flexion or direct pressure
108
Emergency Medicine
Prepatellar Bursitis
Pressure from repetitive kneeling
on a firm surface: rug cutter's knee
Rarely direct trauma
Second most common site for
septic bursitis
109
Emergency Medicine
Prepatellar Bursitis
110
Source Undetermined
Emergency Medicine
Prepatellar Bursitis
111
Source Undetermined
Emergency Medicine
Baker’s Cyst
Pseudothrombophlebitis syndrome
Herniated fluid-filled sacs of
articular synovial membrane that
extend into popliteal fossa
Causes: trauma, rheumatoid
arthritis, gout, osteoarthritis
Pain worse with active knee flexion
112
Emergency Medicine
Baker’s Cyst
Can mimic deep venous
thrombosis
Ultrasound eseential
Many resolve over weeks
May require surgery
Steroid injections not performed:
risk of neurovascular injury
113
Emergency Medicine
Baker’s Cyst
114
Source Undetermined
Emergency Medicine
Baker’s Cyst
Source Undetermined
115
Emergency Medicine
Anserine Bursitis
Cavalryman's disease / pes
bursitis / goosefoot bursitis: obese
women with large thighs, athletes
who run
Anteromedial knee, inferior to joint
line at insertion of sartorius,
semitendinous, and gracilis tendon
116
Emergency Medicine
Anserine Bursitis
Abrupt knee pain, local tenderness
4 to 5 cm below medial aspect of
tibial plateau
Knee flexion exacerbates
117
Emergency Medicine
Iliotibial Band Syndrome
Lateral knee pain
Cyclists, dancers, distance
runners, football players
Pain worse climbing stairs
Tenderness when patient supine,
knee flexed to 90o
118
Emergency Medicine
Ankle and Foot
119
Gray's Anatomy (Wikimedia Commons)
Emergency Medicine
Peroneal Tendonitis
Peroneal tendons cross behind
lateral malleolus
Running, jumping, sprain
Holding foot up and out against
downward pressure causes pain
120
Emergency Medicine
Peroneal Tendon Rupture
Torn retinaculum
Have patient dorsiflex and plantar
flex with foot in inversion
Feel for “snapping” behind lateral
malleolus
121
Emergency Medicine
Foot
Gray's Anatomy (Wikipedia)
Gray's Anatomy (Wikipedia)
122
Emergency Medicine
Retrocalcaneal Bursitis
Ankle overuse: excessive walking,
running, or jumping
Heel pain: especially with walking,
running, palpation
Haglund disease: bony ridge on
posterosuperior calcaneus
Treatment: open heels (clogs),
bare feet, sandals, or heel lift
123
Emergency Medicine
Plantar Fasciitis
Policeman's heel / soldier's heel:
associated with heel spurs
Degenerated plantar fascial band
at origin on medial calcaneous
Heel pain worse in morning and
after long periods of rest
May be relieved with activity
124
Emergency Medicine
Plantar Fasciitis
125
Davius (Wikipedia)
Emergency Medicine
Plantar Fasciitis
Microtears in fascia from overuse?
Eliminate precipitators, rest,
strength and stretching exercises,
arch supports, and night splints
Sometimes need steroid injection
Risk of plantar fascia rupture and
fat pad atrophy
126
Emergency Medicine
Tarsal Tunnel Syndrome
Between medial malleolus and
flexor retinaculum
Vague pain in sole of foot: burning
or tingling
Worse with activity, especially
standing, walking for long periods
Tender along course of nerve
127
Emergency Medicine
Tarsal Tunnel Syndrome
Between medial malleolus and
flexor retinaculum
Vague pain in sole of foot: burning
or tingling
Worse with activity, especially
standing, walking for long periods
Tender along course of nerve
128
Emergency Medicine
Achilles Tendonitis
Grook Da Oger (Wikipedia)
129
Emergency Medicine
Fibromyalgia
Sav vas (Wikimedia Commons)
130
Emergency Medicine
Fibromyalgia
mitopencourseware (Flickr)
131
Emergency Medicine
132
Google
133
Amazon
Emergency Medicine
Fibromyalgia
Pain in muscles, joints, ligaments
and tendons
“Tender points“
– Knees, elbows, hips, neck
5% of population, including kids
Main symptom: sensitivity to pain
134
Emergency Medicine
Fibromyalgia
Pain: chronic, deep or burning,
migratory, intermittent
Fatigue, poor sleep
Numbness or tingling
“Poor blood flow”
Sensitivity to odors, bright lights,
loud noises, medicines
135
Emergency Medicine
Fibromyalgia
Jaw pain
Dry eyes
Difficulty focusing
Dizziness
Balance problems
Chest pain
Rapid or irregular heartbeat
136
Emergency Medicine
Fibromyalgia
Shortness of breath
Difficulty swallowing
Heartburn
Gas
Cramping abdominal pain
Alternating diarrhea & constipation
Frequent urination
137
Emergency Medicine
Fibromyalgia
Pain in bladder area
Urgency
Pelvic pain
Painful menstrual periods
Painful sexual intercourse
Depression
Anxiety
138
Emergency Medicine
Compare to Somatization
Somatization Fibromyalgia
Vomiting
Abdominal pain
Nausea
Bloating
Diarrhea
Leg / arm pain
Back pain
139
Emergency Medicine
Compare to Somatization
Somatization Fibromyalgia
Joint pain
Dysuria
Headaches
Breathlessness
Palpitations
Chest pain
Dizziness
140
Emergency Medicine
Compare to Somatization
Somatization Fibromyalgia
Amnesia
Dysphagia
Vision changes
Weak muscles
Sexual apathy
Dyspareunia
Impotence
141
Emergency Medicine
Compare to Somatization
Somatization Fibromyalgia
Dysmenorrhea
Irregular
menstruation
Excessive
menstrual flow
142
Emergency Medicine
Fibromyalgia
Treatment
143
Emergency Medicine
Reflex Sympathetic Dystrophy
Causalgia
Shoulder-hand syndrome
Sudeck's atrophy
Post-traumatic pain syndrome
Complex regional pain syndrome
type I and type II
Sympathetically maintained pain
144
Emergency Medicine
Reflex Sympathetic Dystrophy
Distal extremity pain, tenderness
Bone demineralization, trophic skin
changes, vasomotor instability
Precipitating event in 2/3: injury,
stroke, MI, local trauma, fracture
Associated with emotional liability,
depression, anxiety
145
Emergency Medicine
Reflex Sympathetic Dystrophy
Treatments: medication, physical
therapy, sympathetic nerve blocks,
psychological support
– Possible sympathectomy or dorsal
column stimulator
Pain Clinic with coordinated plan
may be helpful
146
Emergency Medicine